
Abstract
Background
High blood pressure, left ventricular hypertrophy and diastolic dysfunction may cause hemodynamic and morphological changes in the left atrium, consequently instability and heterogeneity in atrial conduction. This is seen as an increase in maximum P wave duration (Pmax) and P wave dispersion (PD) on the electrocardiogram (ECG). P wave dispersion on ECG has been encountered as a risk factor for atrial fibrillation (AF). The aim of this study is to examine whether PD and Pmax can be used as a non-invasive marker of target organ damage (LVH and diastolic dysfunction) in a hypertensive population.
Material and methods
The study registered a total of 120 cases (mean age 46.9 ± 10.6 years; 58 [48.3%] males and 62 [51.7%] females), of whom 60 were patients diagnosed as essential hypertension (group 1), and 60 were healthy individuals, who constituted the control group (group 2). Systolic and diastolic functions of all cases were evaluated by echocardiography, and maximum P wave duration (Pmax), and PD was calculated.
Results
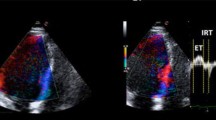
Maximum P wave duration was 91.6 ± 10.2 ms in group 1, and 64 ± 10.2 ms in group 2 (p < 0.01), while PD was 56.1 ± 5.8 ms in group 1, and 30.3 ± 6.6 ms in group 2 (p < 0.01). Blood pressure, left atrium diameter, DT, IVRT, and E/A ratio, as well as left ventricular mass index increased markedly in group 1.
Conclusion
High blood pressure, LVH, diastolic dysfunction and increased left atrium diameter and volume shows parallelism in hypertensive cases. These physiopathological changes may cause different and heterogeneous atrial electrical conduction. This led to a marked increase in Pmax and PD in our cases. Thus, the results support the hypothesis that PD can be used as a non-invasive marker of target organ damage (LVH and LV diastolic dysfunction) in the hypertension population.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Gifford RWJ, Kirkendall W, O’Connor DT, Weidman W (1989) Office evaluation of hypertension. A statement for health professionals by a writing group of the Council for High Blood Pressure Research. American Heart Association. Circulation 79:721–731
Sharp PS, Chaturvedi N, Wormald R, McKeigue PM, Marmot MG, Young SM (1995) Hypertensive retinopathy in Afro-Caribbeans and Europeans. Prevalence and risk factor relationships. Hypertension 25:1322–1325
Aeschbacher BC, Hutter D, Fuhrer J, Weidmann P, Delacretaz E, Allemann Y (2001) Diastolic dysfunction precedes myocardial hypertrophy in the development of hypertension. Am J Hypertens 14:106–113
Modena MG, Mattioli AV, Parato VM, Mattioli G (1992) Effectiveness of the antihypertensive action of lisinopril on left ventricular mass and diastolic filling. Eur Heart J 13:1540–1544
Cha YM, Redfield MM, Shen WK, Gersh BJ (2004) Atrial fibrillation and ventricular dysfunction: a vicious electromechanical cycle. Circulation 109:2839–2843
Lip GY (2001) Regression of left ventricular hypertrophy and improved prognosis: some HOPE now or hype? Circulation 104:1582–1584
Schmieder RE, Schrader J, Zidek W, Tebbe U, Paar WD, Bramlage P et al (2007) Low-grade albuminuria and cardiovascular risk: what is the evidence? Clin Res Cardiol 96:247–257
Tsang TS, Barnes ME, Gersh BJ, Bailey KR, Seward JB (2002) Left atrial volume as a morphophysiologic expression of left ventricular diastolic dysfunction and relation to cardiovascular risk burden. Am J Cardiol 90:1284–1289
Tukek T, Akkaya V, Atilgan D, Demirel E, Ozcan M, Guven O et al (2001) Effect of left atrial size and function on P-wave dispersion: a study in patients with paroxysmal atrial fibrillation. Clin Cardiol 24:676–680
Aytemir K, Amasyali B, Abali G, Kose S, Kilic A, Onalan O et al (2005) The signal-averaged P-wave duration is longer in hypertensive patients with history of paroxysmal atrial fibrillation as compared to those without. Int J Cardiol 103:37–40
Yilmaz R, Demirbag R (2005) P-wave dispersion in patients with stable coronary artery disease and its relationship with severity of the disease. Journal of Electrocardiology 38:279–284
Tukek T, Akkaya V, Demirel S, Sozen AB, Kudat H, Atilgan D et al (2000) Effect of Valsalva maneuver on surface electrocardiographic P-wave dispersion in paroxysmal atrial fibrillation. Am J Cardiol 85:896–899
ACC/AHA guidelines for the clinical application of echocardiography: executive summary (1997) A report of the American College of Cardiology/ American Heart Association Task Force on practice guidelines (Committee on Clinical Application of Echocardiography). J Am Coll Cardiol 29:862–879
European Study Group on Diastolic Heart Failure (1998) How to diagnose diastolic heart failure. Eur Heart J 19: 990–1003
Devereux RB, Reichek N (1977) Echocardiographic determination of left ventricular mass in man. Anatomic validation of the method. Circulation 55:613–618
Chapman N, Mayet J, Ozkor M, Foale R, Thom S, Poulter N (2001) QT intervals and QT dispersion as measures of left ventricular hypertension in an unselected hypertensive population. Am J Hypertens 14:455–462
Calhoun DA, Bakir S, Oparil S (2001) Etiology and pathogenesis of essential hypertension. In: Crawford MH, DiMarco JP (eds) Cardiology. Mosby London, pp 3 1.1–3 1.10
Brilla CG, Funck RC, Rupp H (2000) Lisinopril-mediated regression of myocardial fibrosis in patients with hypertensive heart disease. Circulation 102:1388–1393
Mattioli AV, Bonatti S, Monopoli D, Zennaro M, Mattioli G (2005) Left atrial remodelling after short duration atrial fibrillation in hypertrophic hearts. Heart 91:91–92
Dilaveris PE, Gialafos EJ, Andrikopoulos GK, Richter DJ, Papanikolaou V, Poralis K et al (2000) Clinical and electrocardiographic predictors of recurrent atrial fibrillation. Pacing Clin Electrophysiol 23:352–358
Ozer N, Aytemir K, Ataler E, Sade E, Aksoyek S, Ovunc K et al (2000) P wave dispersion in hypertensive patients with paroxysmal AF. Pacing Clin Electrophysiol 23:1859–1862
Senen K, Turhan H, Riza Erbay A, Basar N, Saatci Yasar A, Sahin O et al (2004) P-wave duration and P-wave dispersion in patients with dilated cardiomyopathy. Eur J Heart Fail 6:567–569
Turhan H, Yetkin E, Sahin O, Yasar AS, Senen K, Atak R et al (2003) Comparison of P-wave duration and dispersion in patients aged N or=65 years with those aged b or = 45 years. J Electrocardiol 36:321–326
Erbay AR, Turhan H, Yasar AS, Bicer A, Senen K, Sasmaz H et al (2005) Effects of long-term beta-blocker therapy on P-wave duration and dispersion in patients with rheumatic mitral stenosis. Int J Cardiol 102:33–37
Lammers WJ, Kirchhof C, Bonke FI, Allessie MA (1992) Vulnerability of rabbit atrium to reentry by hypoxia. Role of inhomogeneity in conduction and wavelength. Am J Physiol 262:H47–55
Kelm M, Schafer S, Mingers S, Heydthausen M, Vogt M, Motz W et al (1996) Left ventricular mass is linked to cardiac noradrenaline in normotensive and hypertensive patients. J Hypertens 14:1357–1364
Cha YM, Dzeja PP, Shen WK, Jahangir A, Hart CY, Terzic A et al (2003) Failing atrial myocardium: energetic deficits accompany structural remodeling and electrical instability. Am J Physiol Heart Circ Physiol 284:H1313–H1320
Cheema AN, Ahmed MW, Kadish AH, Goldberger JJ (1995) Effects of autonomic stimulation and blockade on signal-averaged P wave duration. J Am Coll Cardiol 26:497–502
Dagli N, Karaca I (2006) Hipertansif olgularda nebivolol tedavisinin P dispersiyonu üzerine etkisi. Firat Medical Journal 11:154–159
Vaziri SM, Larson MG, Lauer MS, Benjamin EJ, Levy D (1995) Influence of blood pressure on left atrial size: the Framingham Heart Study. Hypertension 25:1155–1160
Lorell BH, Carabello BA (2000) Left ventricular hypertrophy: pathogenesis, detection, and prognosis. Circulation 102:470–479
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dagli, N., Karaca, I., Yavuzkir, M. et al. Are maximum P wave duration and P wave dispersion a marker of target organ damage in the hypertensive population?. Clin Res Cardiol 97, 98–104 (2008). https://doi.org/10.1007/s00392-007-0587-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00392-007-0587-8