
Abstract
Introduction
Laparoscopic resection of low rectal cancer poses significant technical difficulties for the surgeon. There is a lack of published follow-up data in relation to the surgical, oncological and survival outcomes in these patients.
Aim
The aim of this study is to evaluate the surgical, oncological and survival outcomes in all patients undergoing laparoscopic resection for low rectal cancer.
Methods
Consecutive patients undergoing laparoscopic resection for low rectal cancers were included in the study. Clinical, pathological and follow-up data were recorded over a 4-year period. The mean follow-up was 25 months
Results
A total of 53 patients were included in the study, 30 of whom were males. The mean age was 64.14 years (range, 34–86 years). The mean hospital stay was 8.2 days (range, 4–42 days). Fifty were completed laparoscopically and three were converted to an open procedure. Thirty-eight were anterior resections and 15 were abdominoperineal resections. Twenty-four patients received neoadjuvant chemoradiotherapy. The total mesorectal excision was optimal in 51 (98%) cases. There were no anastomotic sequelae and no surgical mortality. There was no local recurrence detected. The overall survival (mean follow-up, 25 months) was 93.5%.
Conclusion
Laparoscopic resection for low rectal cancers permits optimum oncological control. In our series, this technical approach is associated with excellent 4-year survival and clinical outcomes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Several large randomised controlled trials (MRC CLASICC, COST, COLOR) have demonstrated that oncological concerns surrounding laparoscopic resection for colon cancer are unfounded and are comparable to that of the conventional open approach [1–3]. This operative approach permits faster recovery, a shorter hospital stay, less post-operative pain, less post-operative ileus and improved cosmesis. Such data have led some authors to advocate that laparoscopic colon cancer resection should be the approach of choice for all patients whenever feasible [4]. Despite this, laparoscopic resection of colorectal cancer continues to be performed by the minority of colorectal surgeons. The procedure can be technically challenging and is associated with a steep learning curve, reported as being up to 55 cases for a right hemicolectomy and up to 62 resections for left-sided lesions [5]. In 2007, the percentage of colorectal resections performed laparoscopically in the UK was 8.82% [6]. It remains controversial whether laparoscopic resection of rectal cancer should be considered in the same manner. The optimum laparoscopic resection of rectal cancers poses unique technical challenges to the surgeon. This is secondary to the anatomical constraints of the pelvis, the possibility of the operative field being irradiated (post-neoadjuvant therapy) and the restriction in the degrees of freedom that current laparoscopic instrumentation provides. The resection of low rectal cancer necessitates employing a wide spectrum of operative approaches in order to ensure optimum oncological clearance. Intestinal continuity can be re-established using a coloanal anastomosis with a colonic reservoir (J-pouch or transverse coloplasty) and temporary diverting ileostomy. Alternatively, an abdominoperineal procedure may be performed. Each of these approaches in turn can be associated with considerable inpatient morbidity. These confounding factors of technique, restricted access and the morbidity associated with both reservoir formation and coloanal anastomosis are intensified when undertaking resection for low rectal cancers laparoscopically.
Despite established objective measures of oncological quality including circumferential radial margin (CRM) positivity, lymph node harvest and intact total mesorectal excision (TME), there is a dearth of published data relating to the oncological and survival outcomes in patients undergoing laparoscopic resection for rectal cancer [7]. Laparoscopic resection of low rectal cancers represents arguably the most technically challenging aspect of colorectal cancer surgery. The assessment of these quality assurance parameters and ultimately survival outcomes in such patients merits objective evaluation. We report our own unit’s oncological, operative and survival outcomes following laparoscopic resection of low rectal cancers.
Methods
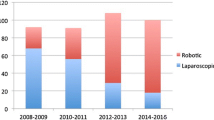
For the purposes of this study, we define low rectal cancer as that in which the proximal tumour margin lies completely below the pelvic peritoneal reflection. All tumours in this study were within 8 cm of the anal verge. Over a 4-year period from July 1, 2005 to June 30, 2009, 53 consecutive patients underwent laparoscopic resection for low rectal carcinoma. Patients were identified from a prospectively recorded database of all rectal cancers treated at the AMNCH (Fig. 1). Patients were selected on an intention to treat basis. There were no exclusion criteria. Data recorded included patient demographics, operative data, disease stage adjuvant treatments as well as data relating to the pathological, clinical and overall survival outcomes. Ethical approval for this study was granted by the ethics committee of AMNCH.

Management of rectal cancer at AMNCH between July 2005 and June 2009
Pre-operative workup
All patients were evaluated pre-operatively with a colonoscopy, biopsy, CT scan, MRI scan and endorectal ultrasound. The level (in centimetres) of the distal tumour margin from the anal verge was determined using a rigid sigmoidoscope. All cases were discussed both pre- and post-operatively at the institutional multidisciplinary meeting. Tumours staged as ≥T3, those with nodal disease or those with a threatened CRM underwent neoadjuvant long-course chemoradiotherapy. These patients received 45 Gy in 25 fractions over a 5-week period and a concomitant course of 5-fluorouracil (on weeks 1 and 5). The operation was carried out 6 weeks after completion of treatment. Locally confined T1 and T2 tumours underwent primary resection without neoadjuvant therapy.
Procedure
Patients received pre-operative bowel preparation with two sachets of sodium picosulphate. Antibiotic prophylaxis and thromboprophylaxis were administered in accordance with international guidelines. A standardised operative technique approach was used, encompassing a medial to lateral approach with initial isolation, control and early flush ligation of the inferior mesenteric artery [8].
The splenic flexure was mobilised for all anterior resections to facilitate a tension-free anastomosis following total mesorectal excision but not for abdominoperineal excisions. The rectal dissection was completed to facilitate adequate distal clearance of the tumour. The rectum was transected using a roticulating Endo GIA® stapling device (45 mm) from Covidien Autosuture, Norwalk. The specimen was delivered through a 5-cm incision in the left iliac fossa using a 3M® Steri-Drape® wound edge protector. The tumour was removed, and pneumoperitoneum was re-established. An end-to-end stapled colorectal anastomosis was constructed using a circular stapling device. Following completion of the air leak test, a defunctioning loop ileostomy was usually constructed in the right iliac fossa. If the tumour lay within 3 cm of the anal verge, an abdominoperineal excision was completed in the prone position following completion of the abdominal component and construction of an end colostomy in the left iliac fossa. Post-operatively, patients were managed according to a standardised post-operative care pathway (RAPID) protocol involving ambulation, early removal of tubes and parenteral analgesia with early resumption of diet [9].
Outcome measures examined included histopathological data such as the quality of the TME, nodal yield, distal resected margin, CRM and TNM data. All specimens were reviewed by two senior histopathologists. The quality of the TME is a macroscopic assessment. It is determined by the bulk of the specimen and the presence or absence of defects in the mesorectal envelope (fascial plane). The mesorectal surface should be smooth with no defect deeper than 5 mm. The mesorectum itself should be of good bulk anteriorly and posteriorly with no ‘coning’ close to the tumour [10].
Operative data recorded included operative time, post-operative morbidity, inpatient stay and the presence of a defunctioning stoma. Disease-free and overall survivals were evaluated in all patients who underwent surgical resection for low rectal cancer. The mean follow-up was 25 months (median, 24months; range, 7–48 months; interquartile range, 16–37 months). In those patients undergoing anterior resection, a defunctioning loop ileostomy was performed in all patients in whom the distal tumour margin was within 7 cm of the anal verge on rigid sigmoidoscopy or following neoadjuvant long-course chemoradiotherapy. Closure of this loop ileostomy was planned to occur 90 days post-formation. In those patients receiving adjuvant treatment, the plan to close the loop ileostomy was made in conjunction with the relevant radio/chemo oncologist. We defined a peri-operative death as one which occurs within 30 days of the procedure.
Follow-up
Patients were seen 1 month following their surgery. Following this initial assessment, patients were then seen every 3 months for the first 2 years, then biannually until 5 years post-operatively and then yearly. Post-operative surveillance consists of a medical history, physical examination and laboratory studies including measurement of carcinoembryonic antigen. Computed tomographies of the thorax, abdomen and pelvis were completed every 6 months. A complete colonoscopy was performed yearly.
Statistical analysis
Analysis of numerical data was completed using the statistical analysis software programme SPSS Version 16.0®. Data were reported and analysed based on the post-operative histopathological staging. This staging is determined by the Royal College of Pathologists guidelines which reflect the American Joint Committee on Cancer (AJCC) guidelines [10]. A Kaplan–Meier survival graph was created using the same software package to illustrate survival based on AJCC stage (Fig. 2).

Kaplan–Meier graph demonstrating survival based on AJCC classification
Results
Fifty-three consecutive patients underwent laparoscopic resection for low rectal cancer. Thirty (57%) were male and 23 were female. The mean age was 64.14 years (range, 34–86 years). ASA grades included: I = 5, II = 31, III = 15 and IV = 2. The mean body mass index was 29 (range, 18–42). There were 38 (72%) sphincter preserving low anterior resections and 15 abdominoperitoneal resections included in the study. The mean distance between the distal tumour margin and the anal verge was 4.51 cm (range, 1–8 cm). Of the APRs, the mean tumour distance from the anal verge was 2.8 cm (range, 1–4 cm). In those undergoing anterior resection, the mean distance from the distal tumour margin to the anal verge (as measured with pre-operative rigid sigmoidoscopy) was 5.2 cm (range, 3–8 cm). Thirty-four (89%) of the anterior resections had a defunctioning loop ileostomy.
Three operations (6%) (two anterior resections) were converted from a laparoscopic to an open procedure. Fifty (94%) procedures were completed laparoscopically. Indications for conversion included dense adhesions (n = 1), ureteric injury requiring repair (n = 1) and progressive metabolic acidosis relating to the prolonged steep Trendelenburg position of the patient (n = 1).
Oncological outcome
Twenty-four (45.2%) patients underwent neoadjuvant treatment prior to surgical intervention. Five (20%) of this cohort of patients had a complete pathological response, with no evidence of residual malignancy found in the resected specimen.
The mean lymph node harvest in those undergoing pre-operative neoadjuvant treatments was 7.5 nodes (range, 2–15). In those (N = 29) who underwent primary resection without neoadjuvant treatment, the nodal harvest was 12.9 (range, 8–22). One positive circumferential margin was reported. TME was optimal in 51 (98%) cases.
Survival
Disease stage and related number of cases along with associated survival are outlined in Table 1. There were no peri-operative mortalities. There was no instance of locoregional recurrence identified in our cohort of patients with a mean follow-up of 25 months. The overall survival (mean follow-up, 25 months) in this cohort of patients was 93.5%. Patients who died (N = 4) had stage IIIb (1), stage IIIc (2) and stage IV (1) diseases, and all died due to disease progression. In patients with non-metastatic low rectal cancer (stages I, IIa and IIb) and those identified with stage IIIa disease, the disease-free survival and overall survival were 100%. This group had a mean follow-up of 24.8 months. There were no port-site metastases identified.
Surgical morbidity
Mean operating time was 230 min (range, 120–425 min). The mean post-operative hospital stay was 8.2 days (range, 4–42 days). Of the 38 patients who had a defunctioning loop ileostomy, 29 (76.3%) underwent a reversal of this with a return to normal bowel function. The mean waiting time to reversal was 154 days (range, 92–420 days). Table 2 outlines all post-operative complications encountered. One ureteric injury occurred during laparoscopic resection. This necessitated conversion to an open procedure in order to repair the involved ureter. It was identified, stented and repaired at open surgery. There were two re-operations during the same admission relating to (a) repair of a symptomatic port-site hernia and (b) refashioning of a colostomy. Both patients made an uneventful recovery and were discharged well.
There were no clinically apparent anastomotic leaks, and there were no inpatient mortalities. Although we do not routinely image the rectal anastomosis, unless clinically indicated in the immediate post-operative inpatient period, all patients with a defunctioned anastomosis had a gastrograffin enema prior to reversal of their stoma.
Discussion
Over the last 20 years, many advances relating to the investigation, diagnosis and treatment of colorectal cancer have occurred. This has resulted in improved survival [11, 12]. Advances in the delivery of adjuvant treatments such as chemotherapy and radiotherapy have contributed greatly to this progress. However, adequate surgical resection remains the cornerstone of the treatment of colorectal cancer. Since its initial application more than 10 years ago, curative colorectal resection may now be achieved via a laparoscopic approach allowing the much documented advantages to patients such as a more rapid recovery, reduced post-operative pain, a shorter hospital stay [13] and improved cosmesis to be achieved. Despite this, the majority (approximately 90%) of colorectal resections continue to be carried out using the conventional open approach. In the case of low rectal cancer, this bias for open resection is even more apparent. The reasons for this are multiple. Low rectal resection poses significant technical difficulties, and the learning curve to achieve adequate laparoscopic oncological control is steep [5].
Data from recent large randomised controlled trials suggest that laparoscopic resection of colorectal cancer is oncologically equivalent to the traditional open approach. However, concerns arising from the MRC CLASICC trial regarding a higher (though non-significant) instance of a positive circumferential margin (CRM) (16% vs 14%) [1] in those undergoing laparoscopic rectal resection and specifically in the subgroup undergoing anterior resection (12% vs 6%) for rectal cancer when compared to those undergoing open resection have been raised by Nelson [14, 15].
Despite this finding, the increase in the number of positive CRMs did not translate into increased local recurrence or negatively impact upon survival.
We examined our data in relation to surgical, oncological and follow-up outcomes for low rectal cancer over a 4-year period. Our data reveal that adequate oncological clearance can be achieved using a laparoscopic approach for resection of low rectal cancers. Adequate lymph node resection at the time of surgery along with accurate retrieval by the pathologist is crucial for correct staging. Lymph node retrieval also directly correlates with incidence of local recurrence [16]. National Cancer Institute guidelines indicate that the minimum number of nodes that should be retrieved in the resected specimen in order to accurately stage the cancer is 12.
Twenty-seven (93%) of the patients undergoing primary resection without neoadjuvant chemoradiotherapy of their cancer reached or surpassed this number. A reduced nodal yield in resected specimens in those patients undergoing neoadjuvant treatment was noted. This finding is well recognised in the literature [17]. Five (20%) patients in this subgroup had a complete pathological response following neoadjuvant chemoradiotherapy. This underscores the importance of accurate pre-operative staging to ensure optimal treatment for each patient. Analysis of all resected specimens revealed one (1.8%) positive CRM. This compares favourably to other reports where positive circumferential margins have reached a level of 16% in those undergoing low anterior resection [1]. Total mesorectal excision (TME) has been shown to reduce local recurrence and to increase disease-free survival [18]. TME was achieved in 98% of all resections. In two patients, it was reported as suboptimal.
These results correlate positively when compared to previous published studies [1, 6]. The conversion rate from a minimal invasive approach to open surgery was 6% (N = 3). On retrospective review, there were no specific pre-operative features that would have suggested an increased likelihood for conversion. In those that were converted to an open procedure, the post-operative morbidity and survival outcomes were similar to those completed laparoscopically, although we acknowledge that no substantial comparison can be made between the two groups.
The intra-operative complication rate in this study is low. One instance of ureteric injury which was recognised and repaired at the time of surgery was reported. The overall post-operative morbidity rate was 28%. In two patients, a re-operation during the same admission was required. There were no clinically significant anastomotic leaks detected, and there was no mortality. This finding may be explained by the high number (89%) of those patients undergoing sphincter preserving surgery having a defunctioning loop ileostomy. In those patients (N = 4) who did not have ileostomy formed, the distal tumour border lay between 7 and 8 cm. None of these four patients had neoadjuvant treatment. The mean post-operative hospitalisation was 8.2 days (range, 4–42 days).
Bowel function and associated quality of life are important considerations in those undergoing rectal surgery. The majority (89%) of the patients undergoing low anterior resection had a defunctioning ileostomy. At the time of completion of this study, 76.3% of patients who had an ileostomy formed had it reversed. The mean time from the date of diagnosis to the restoration of bowel continuity/function in this cohort was 6 months (range, 4–14 months). However, in this study, we have not objectively measured patient quality of life after laparoscopic resection for low rectal cancer.
The magnified view of the operating field associated with laparoscopy lends itself to accurate identification of all important anatomical structures in the narrow confines of the pelvis. Hartley et al. [19] state that laparoscopic resection permits an enhanced view of the pelvic dissection plane and that the magnification of the image facilitates the identification of the avascular plane of the mesorectum both posteriorly and laterally. Published data show that despite the magnified pelvic views, there is an increased rate of sexually active males reporting impotence or retrograde ejaculation after laparoscopic rectal resection [20].We did not specifically examine this entity, but on retrospective review of these patient’s medical records, there were no recordings of this.
In our series, no local recurrence has been identified with a mean follow-up of 25 months. This compares favourably with other published data where the incidence of local recurrence in those undergoing laparoscopic rectal resection has ranged from 3.2% to 6.7% (follow-up of 46.3 and 46.1 months, respectively) [21, 22]. The local recurrence rate following open resection has been shown to lie between 3% and 13%.
This absence of recurrence in our cohort of patients reflects optimal oncological resection with a high rate (98.2%) of negative margins achieved at the time of surgery. Continued surveillance will reveal longer-term outcomes, and we acknowledge that these results may change with time. Our follow-up survival data (overall survival of 93.5%, with mean follow-up of 25 months) indicate that laparoscopic resection for low rectal cancer gives excellent overall and cancer-specific survival. For those patients with non-metastatic rectal cancer (stages I, IIa and IIb), the overall and cancer-specific survivals were 100%.
This data compares positively to previously published evidence regarding survival after laparoscopic rectal resection [21, 22]. The reporting of a 100% disease-free and cancer-related survival in these patients within a protocol driven post-operative surveillance programme is indeed extremely encouraging. Lacy et al. have reported a significant improved survival benefit for patients undergoing laparoscopic colon resection for cancer with a 7-year period [23]. Our data, while extremely early in terms of follow-up, hints at the tantalising prospect that such outcomes may also be possible in low rectal cancer. Further surveillance over time will determine this.
Our results suggest that laparoscopic resection of low rectal cancer is feasible. It is also a safe approach to low rectal tumours, both in relation to surgical morbidity and oncological control. This initial follow-up data (93.5% alive with a mean follow-up of 25 months), in terms of survival and local recurrence, suggest that laparoscopic resection is associated with favourable outcomes. Longer-term (5 to 10 years) survival data are required before we can definitively evaluate the effectiveness of laparoscopic resection of low rectal lesions in relation to these specific outcomes.
We have been unable to compare our outcome data directly to outcomes of the traditional open approach. The number of open low rectal resections (Table 3.) completed in our institution over the same time was low (N = 7). Therefore, we compare our data to widely published outcome data in the literature. We could have used historical controls of open cases carried out within our institution from the 1990s, but this may have given misleading information due to the improvements in all aspects of rectal cancer management ranging from pre-operative staging to changes in adjuvant therapies which have occurred over the same period.
Conclusion
Despite the technical challenges associated with the laparoscopic resection of low rectal cancers, our evaluation of recognised objective oncological indices as surrogate markers of surgical efficacy is reassuring. Our experience demonstrates that laparoscopic resection of low rectal cancer has comparable survival and local recurrence rates to that of published open TME anterior resection data. Optimal oncological resection can also be achieved laparoscopically without significant morbidity. Future prospective randomised studies incorporating data on quality of life and 5-year survival outcomes following laparoscopic resection for rectal cancer may reveal equivalence or superiority to the current gold standard of open TME for rectal cancer.
References
Guillou PJ, Quirke P, Thorpe H, Walker J, Jayne DG, Smith AMH, Heath RM, Brown JM (2005) Short-term endpoints of conventional versus laparoscopic-assisted surgery in patients with colorectal cancer (MRC CLASICC trial). Lancet 365(9472):1718–1726
Tinmouth J, Tomlinson G, Dalibon N, Moutafis M, Fischler M, Nelson H, Sargent DJ (2004) Laparoscopically assisted versus open colectomy for colon cancer. N Engl J Med 351:933–934
Kuhry E, COLOR Study Group et al (2005) Impact of hospital case volume on short-term outcome after laparoscopic operation for colonic cancer. Surg Endosc 19(5):687–692
Lacy AM, García-Valdecasas JC, Delgado S, Castells A, Taurá P, Piqué JM, Visa J (2002) Laparoscopy-assisted colectomy versus open colectomy for treatment of non-metastatic colon cancer: a randomised trial. Lancet 359(9325):2224–2229
Tekkis PP, Senagore AJ, Delaney CP, Fazio VW (2005) Evaluation of the learning curve in laparoscopic colorectal surgery: comparison of right-sided and left-sided resections. Ann Surg 242(1):83–91
Aziz O, Darzi AW (2008) Laparoscopic resection for colorectal cancer: evidence to date. Surg Oncol Clin N Am 17(3):519–531, viii
Delgado S, Momblán D, Salvador L, Bravo R, Castells A, Ibarzabal A, Piqué JM, Lacy AM (2004) Laparoscopic-assisted approach in rectal cancer patients: lessons learned from >200 patients. Surg Endosc Other Interv Tech 18(10):1457–1462
Delaney CP, Neary PC, Heriot AG, Senagore AJ (2006) Operative techniques in laparoscopic colorectal surgery. Lippincott Williams & Wilkins, Philadelphia
Al Chalabi H, Kavanagh DO, Hassan L, Donnell KO, Nugent E, Andrews E, Keane FB, O’Riordain DS, Miller A, Neary P (2010) The benefit of an enhanced recovery programme following elective laparoscopic sigmoid colectomy. Int J Colorectal Dis 25(6):761–766
Williams GT, Quirke P, Shepherd NA (2007) Standards and datasets for reporting cancers. Dataset for colorectal cancer, 2nd edn. The Royal College of Pathologists, London
Taal BG, Van Tinteren H, Zoetmulder FAN (2001) Adjuvant 5FU plus levamisole in colonic or rectal cancer: improved survival in stage II and III. Br J Cancer 85:1437–1443. doi:10.1054/bjoc.2001.2117
Improved survival with preoperative radiotherapy in resectable rectal cancer. Swedish Rectal Cancer Trial (1997). N Engl J Med 336(14):980–987
Ridgway PF, Boyle E, Keane FB, Neary P (2007) Laparoscopic colectomy is cheaper than conventional open resection. Colorectal Dis 9(9):819–824
Soop M, Nelson H (2008) Laparoscopic-assisted proctectomy for rectal cancer: on trial. Ann Surg Oncol 15(9):2357–2359
Soop M, Nelson H (2008) Is laparoscopic resection appropriate for colorectal adenocarcinoma? Adv Surg 42:205–217
Morris EJ, Maughan NJ, Forman D, Quirke P (2007) Identifying stage III colorectal cancer patients: the influence of the patient, surgeon, and pathologist. J Clin Oncol 25(18):2573–2579
Wichmann MW, Müller C, Meyer G, Strauss T, Hornung HM, Lau-Werner U, Angele MK, Schildberg FW (2002) Effect of pre-operative radiochemotherapy on lymph node retrieval after resection of rectal cancer. Arch Surg 137:206–210
Heald RJ, Ryall RD (1986) Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1(8496):1479–1482
Hartley JE, Mehigan BJ, Qureshi AE, Duthie GS, Lee PW, Monson JR (2001) Total mesorectal excision: assessment of the laparoscopic approach. Dis Colon Rectum 44(3):315–321
Quah HM, Jayne DG, Eu KW, Seow-Choen F (2002) Bladder and sexual dysfunction following laparoscopically assisted and conventional open mesorectal resection for cancer. Br J Surg 89(12):1551–1556
Morino M, Allaix ME, Giraudo G, Corno F, Garrone C (2005) Laparoscopic versus open surgery for extraperitoneal rectal cancer: a prospective comparative study. Surg Endosc 19(11):1460–1467
Bärlehner E, Benhidjeb T, Anders S, Schicke B (2005) Laparoscopic resection for rectal cancer: outcomes in 194 patients and review of the literature. Surg Endosc Other Interv Tech 19(6):757
Lacy AM, Delgado S, Castells A, Prins HA, Arroyo V, Ibarzabal A, Pique JM (2008) The long-term results of a randomized clinical trial of laparoscopy-assisted versus open surgery for colon cancer. Ann Surg 248(1):8–9
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Moran, D.C., Kavanagh, D.O., Nugent, E. et al. Laparoscopic resection for low rectal cancer: evaluation of oncological efficacy. Int J Colorectal Dis 26, 1143–1149 (2011). https://doi.org/10.1007/s00384-011-1221-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-011-1221-9