
Abstract
Purpose
Proctalgia fugax (PF) is a benign anorectal condition which has been described in the literature since the nineteenth century commonly presenting to general surgeons. There is little high level evidence on the subject and its therapeutic modalities. We aimed through this systematic literature review to outline the definition and diagnostic criteria of this condition, the aetiology and differential diagnoses and describe the different treatment modalities that have been attempted and their success.
Method
A literature search of Google Scholar™ and Medline using Pubmed as the search engine was used to identify all studies directly related to the definition, aetiology and treatment options for this condition (latest at 12 August 2008) was performed.
Results
The search produced 61 references with three others obtained from the references of these papers. The prevalence of PF in the general population ranges from 4% to 18%. The diagnosis is based on the presence of characteristic symptoms as defined by Rome III guidelines and physical examination. The mainstay of treatment is reassurance and careful counselling with evidence in the literature for warm baths, topical treatment with glyceryl trinitrate or diltiazem and salbutamol inhalation. In persistent cases, local anaesthetic blocks, clonidine or Botox injections can be considered after clarification of risk and benefit.
Conclusion
Based on this we suggest that diagnosis should be made through exclusion of common organic causes such as haemorrhoids, anal fissure or anorectal carcinoma and on the fulfilment of Rome III criteria. The main treatment for this benign condition remains reassurance and topical treatment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Proctalgia fugax (PF) is a benign painful rectal condition which has posed diagnostic and therapeutic challenges to several levels of medical practice, most particularly general practitioners, colorectal surgeons and physicians. It has a modern definition of intermittent, recurring and self-limiting pain in the anorectal region in the absence of organic pathology [1]. It was first described in 1883 by Myrtle [2] and then termed nocturnal proctalgia by the Scottish physician Maclennan [3] as it is thought to occur most particularly at night [4–9]. Attacks tend to be infrequent and seem to occur up to five times a year in 50% of patients [10]. Symptoms rarely set in before puberty [11]. It occurs as part of a spectrum of functional gastrointestinal disorders (therefore addressed by Rome III) but often poses a diagnostic conundrum when the pain persists. It is hence essential to ensure that other pathologies are excluded.
Prevalence in the general population is thought to be between 4% and 18% with many patients presenting to primary health care physicians and due to the fleeting nature of the symptoms, often not requiring further consultations [4, 12–15]. Historically, it was thought to have a predilection to doctors as up to 60% experienced these symptoms [16]. The impact of this condition on the health service is difficult to assess as although it is a condition associated with disability, only 17–20% report their symptoms to their physician [11]. There was also thought to be a male preponderance in early studies [17]; however, more recently a female preponderance is reported [7–10, 13–15, 18, 19].
Although this condition has received considerable attention in the literature, these have mainly been initial reports of definition, review articles surrounding functional gastrointestinal disorders and individual reports of successful treatment modalities. There has been some improvement over the last century due to an increasing understanding of its aetiology; however, firm conclusions and management pathways are yet to be clearly defined. Despite this, we aim through this review to provide a comprehensive guide of the literature available on this subject categorising it into diagnostic and definition criteria, aetiology and treatment options, including a historical perspective concluding with a definitive management pathway based on current evidence that may be followed across all specialities, particularly general practitioners and colorectal surgeons faced with this problem.
Methods
This systematic review was carried out with reference to the AMSTAR measurement tool [20]. This is an 11-item measurement scale developed by an international methodology and systematic review specialist group. It aimed to assess the methodological quality of systematic reviews. Although it is accepted that further work needs to be performed to fully assess the reproducibility and construct validity of AMSTAR, it has demonstrated good face and content validity for measuring the methodological quality of systematic reviews on initial investigations. It was therefore thought to be an appropriate reference tool to be used in this study.
Study selection
A Google Scholar™ and MEDLINE (using Pubmed as the search engine) search was performed using the keywords proctalgia and fugax with no time limits. The “related articles” function was used in Pubmed to broaden the search, and all titles, abstracts, studies and citations scanned were reviewed. References of the articles acquired in full were also reviewed. Only English articles were used except in clinical trials due to limited numbers. The latest date of this search was 12 August 2008.
Date extraction and inclusion criteria
Papers were reviewed by two authors (SJ and SP), and differences were resolved by consensus. All information related to definition, aetiology and therapeutic modalities were extracted from all studies. All studies that had relevant information to these areas were included. The evidence for treatment was assessed by the US preventive services task force (USPSTF) criteria [21], and the articles were rated according to levels A to I; A—USPSTF strongly recommends that clinicians provide [the service] to eligible patients, B—the USPSTF recommends that clinicians provide [this service] to eligible patients, C—the USPSTF makes no recommendation for or against routine provision of [the service], D—the USPSTF recommends against routinely providing [the service] to asymptomatic patients and I—the USPSTF concludes that the evidence is insufficient to recommend for or against routinely providing [the service] [21].
Results
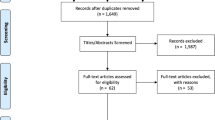
This Medline search produced 90 references. The search was limited to articles in the English language except clinical trials when all articles were included as there were only four studies available for review. This produced 73 references. Articles excluded were those not directly related to PF and were related to dermatology [1, 22], overviews of functional bowel and anorectal disease with short mention of PF [4, 23–26], case reports of rectal pain caused by other pathologies [3, 27–30], paediatric cases [3, 31–34] and an article unrelated to PF but with the term in the title [1, 35]. One paper was cited twice in the search [36].
This gave 61 references which were reviewed with three others obtained searching the references of these papers. There were 2 prospective randomised trials [37, 38], 2 prospective case control studies [18, 39], 10 prospective descriptive studies [1, 8, 10, 13, 15, 40–44], 4 retrospective descriptive studies [19, 45–47], 4 reviews with case reports [6, 36, 48, 49], 17 review articles [4, 5, 9, 11, 12, 14, 17, 50–59], 18 case reports [2, 3, 16, 60–74] and 7 letters [75–81]. A flow chart depicting the selection criteria of the articles reviewed is shown in Fig. 1. A summary of the papers reviewed and the information they include (definition, aetiology/pathogenesis, conservative or surgical management) are presented in Table 1.

Flow chart for literature search
Definition
The term “proctalgia fugax”, a Greek–Latin hybrid term was coined by Thaysen in 1935 [16], and the condition was more firmly defined then as
-
1.
Attacks that begin suddenly at irregular intervals during the day or night.
-
2.
Pain spontaneously disappears without leaving any ill effects except a quickly passing lassitude.
-
3.
The localization of the pain in the rectal region is always at the same place.
-
4.
The degree of pain is so severe that some patients feel faint during the attack.
-
5.
The duration is short, continuing for only a very few minutes in most patients.
-
6.
The pains are very uncomfortable, often described as gnawing, aching or cramp-like.
The pain has been reported to be precipitated by sexual intercourse [4, 5, 9, 19], masturbation [6], stress [1, 5, 6, 44], defaecation [1, 4–6, 9, 10, 14, 48] and menstruation [1] although it can be largely without a trigger. Conversely, other authors report that it is independent of evacuation [50]. There is also a great variation in the length of the pain from a few seconds [7, 19, 58] to 2 h [19]. The average duration has only been reported twice as 15 min [1, 8] and occurs less than five times per year in 51% of patients [12].
Presently, it is very clearly defined by the Rome III Criteria (Table 2) as recurrent episodes of recurrent episodes of pain localised to the anus or lower rectum which last from seconds to minutes with no anorectal pain between episodes [11]. Proctalgia fugax is differentiated from chronic proctalgia, also a functional anorectal pain disorder based on duration, frequency and characteristic quality of pain [51, 56]. It is necessary to exclude other causes of anorectal pain such as haemorrhoids, cryptitis, ischaemia, intramuscular abscess or fissure, rectocele, malignancy and inflammation and to differentiate from other urogenital and pelvic pain disorders when making the diagnosis, and this can be done successfully with the criteria defined [53].
Chronic proctalgia is also called levator ani syndrome, levator spasm, puborectalis syndrome, pyriformis syndrome or pelvic tension myalgia. This is described as a vague, dull ache or pressure sensation high in the rectum, often worse with sitting than with standing or lying down which lasts at least 20 min. Chronic proctalgia may be further characterized into levator ani syndrome where there is tenderness during posterior traction of the puborectalis or unspecified anorectal pain when this tenderness is absent based on digital rectal examination [11]. Chronic proctalgia differs from proctalgia fugax by the length of time each episode lasts, in that PF lasts seconds to minutes whereas chronic proctalgia lasts for at least 20 min [11].
Aetiology
There are several proposed aetiological mechanisms for proctalgia fugax with anal sphincter spasm being the overridingly quoted cause [6, 18, 43, 49, 66, 82]. This spasm has been observed during an attack by one author [18] but refuted by another who did not observe this spasm during the episode of pain [9].
Measurement of the colonic and intraluminal pressures during an attack showed increased pressure in the sigmoid [43]. A more recent study showed a significantly increased resting pressure in these patients but no other differences in anorectal function. In subjects who developed symptoms during the study, there was a further rise in anal resting tone and increased slow wave amplitude [18]. Anal resting pressure is mainly derived from internal anal sphincter tone [83, 84], and slow waves are considered to be an intrinsic activity of the smooth muscle [83]. This activity is thought to be increased by sympathetic activity [83] which may explain the correlation of the symptom with stress.
Thaysen suggested the pain may be due to a haemorrhoidal tumour compressed by the action of the sphincter ani [16]. In patients with this condition, a shelf above the anal sphincter has been described but its significance is unclear [57]. It has also been attributed to constipation [5, 19], sitting in a chair [19], drinking alcohol [19], cold nights [58], sexual frustration [4] and sexual activity [4, 5, 9, 19, 72]. Sclerotherapy for haemorrhoids and vaginal hysterectomy have also been cited as causes [6].
A familial form of proctalgia fugax has been described which is autosomal dominantly inherited [36, 65, 67, 68]. These patients also suffer with constipation [63]. Endo-anal ultrasound showed pathological thickening of the internal anal sphincter, and histology shows vacuolar changes with polyglysan inclusion bodies [45, 60, 68]. These patients also demonstrate increased resting pressures and slow wave amplitude on examination of anorectal physiology through manometry [67]. It is a rare cause of this problem with only two families reported in England. In these patients, constipation has been shown to be improved with internal anal sphincter myomectomy but is not as effective in resolving pain [65, 68].
Pudendal nerve compression has also been reported to cause proctalgia fugax [76]. In these patients perianal sensation is impaired with subnormal rectal neck and squeezing pressure. Electromyography showed reduced external anal sphincter activity and pudendal nerve terminal latency leading to the diagnosis of pudendal nerve compression. Decompression can be performed by opening the pudendal canal through a perineal approach with symptomatic and electromyographic improvement in five of six patients [76].
Some authors suggest that as a functional pathology, proctalgia fugax coexists with up to 52% of patients with irritable bowel syndrome (IBS) [43, 44] although others dispute this [10]. This relationship with IBS may also be related to the increased sigmoid pressures reported previously [43]. It has also historically been thought to be strongly psychoneurotic in nature [16, 80] precipitated by stressful life events or anxiety [65]. Psychological testing suggests that patients are perfectionistic, anxious or hypochondriacal with a higher incidence of neurotic symptoms in childhood [44]; however, a causal relationship has not been confirmed. Patients with proctalgia fugax have also been shown to have greater neuroticism, psychoticism, depression and pain than patients with the organic pathology of anal fissure [42].
A study in normal multiparous middle aged women found a higher prevalence of proctalgia fugax in women with pelvic organ prolapse compared to those with urinary incontinence. This association may explain the female preponderance seen, and it may be due to lack of distinguishing between gynaecologic prolapse from the vagina and anorectal pain [41].
Treatment
There are few case series and fewer still randomised control trials resulting in a significant shortage of evidence upon which to base management of PF. Each of the treatments are summarised below along with the USPSTF categorisation for each modality (Table 3)
Simple treatments
Most historical accounts for resolving symptoms lead to sphincter relaxation and anorectal dilatation. These measures include the forced effort to evacuate the bowels [16] or digital dilatation [77]. Other initial reports suggest taking food or drink to initiate the gastrocolic reflex to alleviate spasm [17], positional changes such as sitting up or squatting [17, 47], assumption of the knees to chest position with knees widely apart and clutch each buttock and pull hard as possible expelling gas [79]. Historically, MacLennan and Thaysen suggested that when attributed to neurosis, chloroform should be used [3, 16].
Water at 40°C has been shown to reduce resting anal canal pressure [39], hence the recommendation of hot baths as symptomatic treatment [52]. Tap water at body temperature inserted as an enema has been reported to be successful in a self reporting physician and three of his patients with immediate symptomatic relief as well as by earlier authors [40, 46]. However, it is often the case that there is insufficient time for any of these measures be taken [16].
Topical treatments
There have been reports of effective treatment with antispasmodics [6, 74] and nitroglycerin [6, 64, 85].
Oral and systemic treatments
Treatment with the calcium channel blocker nifedipine has been shown to reduce anal sphincter pressure [67, 68], and others such as diltiazem [71] are reportedly successful but not verified.
There have also been single reports of the efficacy of oral clonidine [70] (an alpha 2 adrenoceptor agonist) which acts by inhibiting the post synaptic neurone or inhibiting release of the neurotransmitter from the presynaptic neurone. These receptors are located on sympathetic and parasympathetic nerve terminals in the GI tract [86] so may have caused relaxation of the rectal muscle and sphincter; it also has an antispastic effect which may cause sphincter relaxation [70, 87].
There is a single report of administration of an IV infusion of lidocaine (1 mg/kg) which led to resolution of symptoms in a patient with intractable pain after trying all the above preparations [61]. Systemic lidocaine is believed to have its suppressive effects on spontaneous ectopic discharges of injured nerve without blocking normal nerve conduction [88] and may produce complete elimination of the pain through a change in the nerve action potential setting [89].
Inhaled salbutamol was first described by a physician who self-treated [78]. This author attempted an RCT but, due to poor compliance, reached no reportable significant conclusion [81]. However, more recently a single double blind, placebo controlled randomised trial in 18 patients was performed. Inhalation of salbutamol, a β-adrenergic agonist, was more effective than placebo for shortening of duration of episodes of proctalgia for those patients in whom episodes last longer than 20 min [38] although when symptoms last this long, it may be considered chronic proctalgia. The mechanism of this action is unclear although may be due to beta agonist inhibition of sphincteric smooth muscle of the GI tract reducing tone and motility.
Invasive treatments
Botulinum toxin has also been used in a single patient with limited success [62] and then in a later study of five patients versus controls with resolution of symptoms for up to 2 years with 25 units of Botox, with a further 50 units in one patient with persistence of symptoms [37]. In these patients, prior to treatment they had increased mean resting pressure on anal manometry compared to controls which returned to normal values after treatment. Its action is thought to be through the prevention of release of acetylcholine resulting in reduced sphincter spasm.
Patients with diagnosed pudendal nerve compression with PF found relief with a local pudendal nerve block and complete resolution with pudendal nerve decompression [75]. Superior hypogastric plexus block has also been described to provide symptomatic relief in a wide variety of patients with perineal pain and may have a role in proctalgia fugax [69].
There is little evidence for surgical procedures, particularly internal anal sphincterotomy except in patients with the autosomal dominantly inherited form of PF, where there is pathological thickening of the internal anal sphincter. As mentioned previously, there may be improvement in symptoms of constipation in these patients but is not as effective in improving pain [65, 68].
A therapeutic regimen has been suggested by other authors consisting of reassurance, warm baths and oral benzodiazepines (dose unstated) as a first step, sublingual nifedipine (10 mg; or topical 0.2% nitroglycerin ointment) at the time of symptoms as a second step and a third step of internal anal sphincterotomy when endoanal ultrasound showed internal anal sphincter thickening of greater than 3.5 mm. This treatment was sequentially provided and showed an improvement in 50–60% of patients at each stage in a total of 15 patients [8].
Conclusions and management pathway
In the drive to tailor colorectal services to the rapid assessment and exclusion of colorectal cancer, there is a risk of failing to address the underlying symptoms in groups of patients that may be significantly debilitated by ‘benign’ anorectal conditions. Lack of understanding of such problems and a consequent failure to address them may potentially disadvantage a sizeable group of patients.
The diagnosis of PF is based on the presence of characteristic symptoms as defined by Rome III guidelines and physical examination. In diagnosis of levator ani syndrome, during puborectalis palpation, tenderness may be predominantly left sided, and massage of this muscle generally elicits the characteristic discomfort [11].
Anorectal and pelvic pathology requires exclusion although some authors suggest that diagnosis can be made by symptoms alone [54–56]. We suggest, however, that it is mandatory to exclude all other organic causes of anorectal pain first. Proctoscopy, rigid sigmoidoscopy, endoanal ultrasound and MRI imaging should be considered, although hypertrophy of the internal anal sphincter may be seen in those with the hereditary form of this condition. Anorectal manometry may demonstrate an increased internal anal sphincter pressure. It is also important to exclude a depressive symptomatology contributing to chronic pain syndrome.
The Rome III guidelines state that symptoms that are otherwise consistent with the diagnosis warrant treatment in clinical practice. In most patients where organic causes are excluded, symptoms are mild enough such that reassurance and explanation suffice. Patients with frequent symptoms or over a prolonged period may require other treatment methods.
We suggest that once the diagnosis is confirmed, most patients may find resolution of symptoms with reassurance and warm baths. If symptoms persist, beyond 3 months treatment with topical glyceryl trinitrate (0.2%) or diltiazem (2%) depending on the onset of headache is suggested. If topical therapy does not work, salbutamol inhalation (200 μg) should be suggested. In the event that these options may not result in improvement or resolution, other treatments such as warm water enema, clonidine (150 μg, twice a day), local anaesthetic blocks or Botolinum toxin injection to the internal anal sphincter can be attempted as long as patients are counselled clearly about the risks and benefits as well as the existing evidence. We do not advocate internal anal sphincterotomy due to the lack of evidence surrounding this treatment except in patients with pathological thickening of the internal anal sphincters, particularly those with the familial condition. This management pathway is outlined in Fig. 2. The most effective of the treatment options are of the simplest nature, and these can be easily instituted by primary care practitioners.

Suggested management pathway for patients presenting with anorectal pain
We conclude that PF has very clear definitions to aid diagnosis; however, it should be should be a diagnosis of exclusion rather than one that can be made on symptomatology alone particularly in light of the numerous potentially serious differential diagnoses of the presentation. Although there is little level A evidence, more randomised control trials may be required. However, due to the short-lived nature of the symptoms and the nocturnal pattern, this may be difficult to achieve. Given the information that is currently available, we suggest that our management pathway can be adhered to with confidence and should provide relief to most patients.
References
de Parades V, Etienney I, Bauer P, Taouk M, Atienza P (2007) Proctalgia fugax: demographic and clinical characteristics. What every doctor should know from a prospective study of 54 patients. Dis Colon Rectum 50(6):893–898
Myrtle AS (1883) Some common afflictions of the anus often neglected by medical men and patients. BMJ 1:1061–1062
MacLennan A (1917) A short note of rectal crises of non-tabetic origin. Glasgow Medical Journal 88:129–131
Ibrahim H (1961) Proctalgia fugax. Gut 2:137–140
McEwin R (1956) Proctalgia fugax. Med J Aust 43(9):337–340
Karras JD, Angelo G (1951) Proctalgia fugax. Am J Surg 82(5):616–625
Lans WR (1994) Proctalgia fugax: curable after all? Coloproctology 16:128–132
Gracia Solanas JA, Ramirez Rodriguez JM, Elia Guedea M, Aguilella Diago V, Martinez Diez M (2005) Sequential treatment for proctalgia fugax. Mid-term follow-up. Rev Esp Enferm Dig 97(7):491–496
Douthwaite AH (1962) Proctalgia fugax. Br Med J 2(5298):164–165
Thompson WG (1984) Proctalgia fugax in patients with the irritable bowel, peptic ulcer, or inflammatory bowel disease. Am J Gastroenterol 79(6):450–452
Bharucha AE, Wald A, Enck P, Rao S (2006) Functional anorectal disorders. Gastroenterology 130(5):1510–1518
Whitehead WE, Wald A, Diamant NE, Enck P, Pemberton JH, Rao SS (1999) Functional disorders of the anus and rectum. Gut 45(Suppl 2):II55–II59
Boyce PM, Talley NJ, Burke C, Koloski NA (2006) Epidemiology of the functional gastrointestinal disorders diagnosed according to Rome II criteria: an Australian population-based study. Intern Med J 36(1):28–36
Thompson WG, Heaton KW (1980) Proctalgia fugax. J R Coll Physicians Lond 14(4):247–248
Drossman DA, Li Z, Andruzzi E, Temple RD, Talley NJ, Thompson WG et al (1993) U.S. householder survey of functional gastrointestinal disorders. Prevalence, sociodemography, and health impact. Dig Dis Sci 38(9):1569–1580
Thaysen TE (1935) Proctalgia fugax. Lancet 2:243–246
Ewing MR (1953) Proctalgia fugax. Br Med J 1(4819):1083–1085
Eckardt VF, Dodt O, Kanzler G, Bernhard G (1996) Anorectal function and morphology in patients with sporadic proctalgia fugax. Dis Colon Rectum 39(7):755–762
Takano M (2005) Proctalgia fugax: caused by pudendal neuropathy? Dis Colon Rectum 48(1):114–120
Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C et al (2007) Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol 7:10
Rockville M (2000–2003) U.S. preventive services task force ratings: strength of recommendations and quality of evidence. Guide to clinical preventive services: Agency for Healthcare Research and Quality
Wollina U, Konrad H, Petersen S (2005) Botulinum toxin in dermatology—beyond wrinkles and sweat. J Cosmet Dermatol 4(4):223–227
Pfenninger JL, Zainea GG (2001) Common anorectal conditions: part I. Symptoms and complaints. Am Fam Physician 63(12):2391–2398
Schmulson M, Ortiz O, Santiago-Lomeli M, Gutierrez-Reyes G, Gutierrez-Ruiz MC, Robles-Diaz G et al (2006) Frequency of functional bowel disorders among healthy volunteers in Mexico City. Dig Dis 24(3–4):342–347
Whitehead WE (1996) Functional anorectal disorders. Semin Gastrointest Dis 7(4):230–236
Peery WH (1988) Proctalgia fugax: a clinical enigma. South Med J 81(5):621–623
Kornel EE, Vlahakos D (1988) Intraspinal schwannoma presenting solely with rectal pain. Neurosurgery 22(2):417–419
Singer MA, Cintron JR, Martz JE, Schoetz DJ, Abcarian H (2003) Retrorectal cyst: a rare tumor frequently misdiagnosed. J Am Coll Surg 196(6):880–886
Khan A, Ahmed M, Talati J (1989) Seminal vesicle cystic dilatation masquerading as proctalgia fugax. Br J Urol 64(4):428–429
Sinaki M, Merritt JL, Stillwell GK (1977) Tension myalgia of the pelvic floor. Mayo Clin Proc 52(11):717–722
Nathan BN (1990) An early clinical account of proctalgia fugax. Dis Colon Rectum 33(6):539
Weizman Z, Binsztok M (1989) Proctalgia fugax in teenagers. J Pediatr 114(5):813–814
Brown ET (1971) Proctalgia fugax infantum. Ann Allergy 29(2):99–100
Pounders CM (1957) Proctalgia fugax infantum: painful defecation in allergic infants. J Pediatr 51(4):413–415
Oatfield H (1962) fugax. Books, the unknown quantity to librarians. Bull Med Libr Assoc 50:224–235
Karras JD, Angelo G (1963) Proctalgia fugax. Clinical observations and a new diagnostic aid. Dis Colon Rectum 6:130–134
Sanchez Romero AM, Arroyo Sebastian A, Perez Vicente FA, Serrano Paz P, Candela Polo F, Calpena Rico R (2006) Treatment of proctalgia fugax with botulinum toxin: results in 5 patients. Rev Clin Esp 206(3):137–140
Eckardt VF, Dodt O, Kanzler G, Bernhard G (1996) Treatment of proctalgia fugax with salbutamol inhalation. Am J Gastroenterol 91(4):686–689
Dodi G, Bogoni F, Infantino A, Pianon P, Mortellaro LM, Lise M (1986) Hot or cold in anal pain? A study of the changes in internal anal sphincter pressure profiles. Dis Colon Rectum 29(4):248–251
Olsen B (2008) Proctalgia fugax—a nightmare drowned in enema. Colorectal Dis 10(5):522–523
Jelovsek JE, Barber MD, Paraiso MF, Walters MD (2005) Functional bowel and anorectal disorders in patients with pelvic organ prolapse and incontinence. Am J Obstet Gynecol 193(6):2105–2111
Magni G, de Bertolini C, Dodi G, Infantino A (1986) Psychological findings in chronic anal pain. Psychopathology 19(4):170–174
Harvey RF (1979) Colonic motility in proctalgia fugax. Lancet 2(8145):713–714
Pilling LF, Swenson WM, Hill JR (1965) The psychologic aspects of proctalgia fugax. Dis Colon Rectum 8(5):372–376
Martin JE, Swash M, Kamm MA, Mather K, Cox EL, Gray A (1990) Myopathy of internal anal sphincter with polyglucosan inclusions. J Pathol 161(3):221–226
Penny RW (1970) The doctor's disease—proctalgia fugax. Practitioner 204(224):843–845
Potthast OJ (1964) The treatment of proctalgia fugax: four more years of experience. South Med J 57:255–258
Eibel P (1970) Proctalgia fugax: recurrent fulminating coccygodynia. A report of three cases with a review of the literature. Clin Orthop Relat Res 73:116–120
Paradis H, Marganoff H (1969) Rectal pain of extrarectal origin. Dis Colon Rectum 12(4):306–312
Mazza L, Formento E, Fonda G (2004) Anorectal and perineal pain: new pathophysiological hypothesis. Tech Coloproctol 8(2):77–83
Wald A (2001) Functional anorectal and pelvic pain. Gastroenterol Clin North Am 30(1):243–251, viii–ix
Potter MA, Bartolo DC (2001) Proctalgia fugax. Eur J Gastroenterol Hepatol 13(11):1289–1290
Wesselmann U, Burnett AL, Heinberg LJ (1997) The urogenital and rectal pain syndromes. Pain 73(3):269–294
Babb RR (1996) Proctalgia fugax: would you recognize it? Postgrad Med 99(4):263–264
Nidorf DM, Jamison ER (1995) Proctalgia fugax. Am Fam Physician 52(8):2238–2240
Vincent C (1999) Anorectal pain and irritation: anal fissure, levator syndrome, proctalgia fugax, and pruritus ani. Prim Care 26(1):53–68
Scott D (1982) Proctalgia fugax. Postgrad Med 72(3):44–45
Thompson WG (1981) Proctalgia fugax. Dig Dis Sci 26(12):1121–1124
Spiesman MG, Malow L (1952) Coccygodynia and proctalgia fugax. Am J Proctol 3(4):310–313
de la Portilla F, Borrero JJ, Rafel E (2005) Hereditary vacuolar internal anal sphincter myopathy causing proctalgia fugax and constipation: a new case contribution. Eur J Gastroenterol Hepatol 17(3):359–361
Peleg R, Shvartzman P (2002) Low-dose intravenous lidocaine as treatment for proctalgia fugax. Reg Anesth Pain Med 27(1):97–99
Katsinelos P, Kalomenopoulou M, Christodoulou K, Katsiba D, Tsolkas P, Pilpilidis I et al (2001) Treatment of proctalgia fugax with botulinum A toxin. Eur J Gastroenterol Hepatol 13(11):1371–1373
Konig P, Ambrose NS, Scott N (2000) Hereditary internal anal sphincter myopathy causing proctalgia fugax and constipation: further clinical and histological characterization in a patient. Eur J Gastroenterol Hepatol 12(1):127–128
Lowenstein B, Cataldo PA (1998) Treatment of proctalgia fugax with topical nitroglycerin: report of a case. Dis Colon Rectum 41(5):667–668
Guy RJ, Kamm MA, Martin JE (1997) Internal anal sphincter myopathy causing proctalgia fugax and constipation: further clinical and radiological characterization in a patient. Eur J Gastroenterol Hepatol 9(2):221–224
Rao SS, Hatfield RA (1996) Paroxysmal anal hyperkinesis: a characteristic feature of proctalgia fugax. Gut 39(4):609–612
Celik AF, Katsinelos P, Read NW, Khan MI, Donnelly TC (1995) Hereditary proctalgia fugax and constipation: report of a second family. Gut 36(4):581–584
Kamm MA, Hoyle CH, Burleigh DE, Law PJ, Swash M, Martin JE et al (1991) Hereditary internal anal sphincter myopathy causing proctalgia fugax and constipation. A newly identified condition. Gastroenterology 100(3):805–810
Waldman SD, Wilson WL, Kreps RD (1991) Superior hypogastric plexus block using a single needle and computed tomography guidance: description of a modified technique. Reg Anesth 16(5):286–287
Swain R (1987) Oral clonidine for proctalgia fugax. Gut 28(8):1039–1040
Boquet J, Moore N, Lhuintre JP, Boismare F (1986) Diltiazem for proctalgia fugax. Lancet 1(8496):1493
Mountifield JA (1986) Proctalgia fugax: a cause of marital dysharmony. Cmaj 134(11):1269–1270
Burdick GE (1979) Proctalgia fugax: a pain in the rear. Ariz Med 36(7):511–512
Schuster MM (1977) Constipation and anorectal disorders. Clin Gastroenterol 6(3):643–658
Bascom JU (1998) Pudendal canal syndrome and proctalgia fugax: a mechanism creating pain. Dis Colon Rectum 41(3):406
Shafik A (1997) Pudendal canal syndrome and proctalgia fugax. Dis Colon Rectum 40(4):504
Rockefeller R (1996) Digital dilatation for relief of proctalgia fugax. Am Fam Physician 54(1):72
Wright JE (1985) Inhaled salbutamol for proctalgia fugax. Lancet 2(8456):659–660
Kaufman W (1982) Treatment of proctalgia fugax. Dig Dis Sci 27(10):955
Stanley OT (1981) Proctalgia fugax and psychiatric illness. Med J Aust 1(2):90
Wright JE (1991) Trial of inhaled salbutamol for proctalgia fugax. Lancet 337(8737):359
Hertz AF (1909) Constipation and allied intestinal disorders. Oxford University Press, London
McHugh SM, Diamant NE (1987) Effect of age, gender, and parity on anal canal pressures. Contribution of impaired anal sphincter function to fecal incontinence. Dig Dis Sci 32(7):726–736
Frenckner B, Euler CV (1975) Influence of pudendal block on the function of the anal sphincters. Gut 16(6):482–489
Clayton MR (1985) Therapy for proctodynia. Med J Aust 143(11):532
Starke K (1981) Presynaptic receptors. Annu Rev Pharmacol Toxicol 21:7–30
Jennewein HMS, Stockhaus K, Lehr E (1983) The psychotropic effects of clonidine. Steinkopf, Darmstadt
Mao J, Chen LL (2000) Systemic lidocaine for neuropathic pain relief. Pain 87(1):7–17
Baranowski AP, De Courcey J, Bonello E (1999) A trial of intravenous lidocaine on the pain and allodynia of postherpetic neuralgia. J Pain Symptom Manage 17(6):429–433
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jeyarajah, S., Chow, A., Ziprin, P. et al. Proctalgia fugax, an evidence-based management pathway. Int J Colorectal Dis 25, 1037–1046 (2010). https://doi.org/10.1007/s00384-010-0984-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-010-0984-8