
Abstract
Background and aims
Endothelins, a group of polyfunctional cytokines, induce the adhesion of circulating leucocytes to venous endothelium, an initial step in the pathogenesis of a cellular infiltrate in inflammatory bowel disease (IBD). The effect of bosentan, a non-selective endothelin receptor antagonist, on leucocyte adhesion and inflammation in a murine model of IBD was studied.
Materials and Methods
Thirty BALB/c mice were divided into three groups of 10 animals: untreated controls, chronic colitis [dextran sodium sulphate (DSS), 3% w/v for 30 days], and treatment with bosentan (30 mg/kg i.p. daily on days 26–30). On day 30, adherent and rolling leucocytes and the average rolling velocity were assessed by intravital microscopy. Clinical and histological activity of inflammation were assessed by the disease activity index and modified Dieleman score, respectively.
Statistics
Kruskal–Wallis test was used, followed by Dunn's method. A value of p<0.05 was considered significant.
Results
Compared to healthy controls, mice treated with DSS showed pronounced clinical and histological inflammation, and a higher number of rolling and adhering leucocytes in colonic submucosal venules. Therapy with bosentan significantly reduced clinical and histological inflammation. Adherent leucocyte levels were markedly lower (1.2±0.3 vs 23.7±2.8 adherent cells per 0.01 mm2, p<0.05). The number of rolling leucocytes was lower but not significantly different. However, rolling velocity was significantly higher (91.5±14.0 vs 19.0±1.6 μm/s, p<0.05).
Conclusions
Bosentan reduces the adhesion of leucocytes in colonic submucosal venules and reduces inflammation in this mouse model of IBD. By inhibiting leucocyte adhesion, a crucial step in the recruitment of leucocytes to the inflamed tissue, bosentan is a potent therapeutic drug in this animal model. Further studies are necessary to investigate the role of bosentan as a novel drug in human IBD.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The etiology and pathogenesis of human inflammatory bowel disease (IBD) still remain unclear. Recently, endothelins, a group of polyfunctional cytokines, were recognized to play a potential role in the pathogenesis of IBD. Endothelins are the strongest vasoconstrictors known today; however, endothelins have multiple physiological functions that are not yet completely understood [1, 2]. Four different endothelins (ET-1, ET-2, ET-3 and ET-4) act on two receptor types cloned in humans (ETA and ETB) [2]. In patients with IBD, the plasma level of ET-1 is significantly higher than in healthy controls [3]. Furthermore, in IBD, the density of endothelin positive cells in the bowel wall is increased [4], as well as the expression of endothelin receptors [5].
Endothelins act as proinflammatory agents via several mechanisms: Endothelins can induce the release of proinflammatory cytokines [6, 7], provoke local ischaemia [4], or disturb the intestinal permeability, allowing antigen translocation from lumen to bowel wall [8].
It is of special interest that endothelins induce leucocyte adhesion in submucosal venules of the bowel [9, 10]. This leucocyte adhesion is probably due to endothelin-induced up-regulation of cell adhesion molecules on endothelium and leucocytes [3, 11–15]. Activated leucocyte adhesion is the initial and rate-limiting step in the development of an inflammatory cellular infiltrate. Both endothelin receptors, ETA and ETB, are involved in the endothelin-induced activation of leucocyte adhesion [9, 15, 16]. Based on these facts, endothelin receptor antagonists might be an effective treatment of IBD, blocking the recruitment of leucocytes to the bowel mucosa by reduction of leucocyte adhesion. Indeed, prophylactic oral administration of bosentan, a non-selective endothelin receptor antagonist, reduced clinical inflammation and myeloperoxidase activity in colonic tissue in trinitrobenzene sulphonate (TNBS)-induced colitis in rats [17, 18]. A histological scoring was not performed in previous studies, so the effect on histological inflammation could not be statistically evaluated. Interestingly, reduction of colitis was not observed when drug administration started 1 h after induction of colitis [17]. Hogaboam et al. [17] hypothesized that bosentan might have a prophylactic effect, but no effect on an established inflammation. Thus it remains unclear if bosentan can ameliorate an established chronic colitis. Furthermore, it is not yet known which mechanisms mediate the anti-inflammatory action of bosentan.
In this study, we used dextran sodium sulphate (DSS)-induced chronic colitis of mice as a valid model of IBD [19–21]. Chronic DSS-induced colitis was treated with bosentan, an unspecific endothelin receptor antagonist that blocks ETA and ETB receptors.
The first aim of the study was to clarify the following question: Does bosentan reduce the clinical and histological inflammation of chronic DSS-induced colitis? To answer this question, we assessed the effect of bosentan on clinical and histological inflammation by a clinical disease activity index (DAI) [22] and a histological colitis score [19], respectively. Administration of bosentan started when colitis was fully established (therapeutic setting).
The second aim of the study was to clarify the mechanisms mediating the anti-inflammatory action of bosentan. No study so far has evaluated the effect of endothelin receptor antagonists on leucocyte adhesion in an animal model of IBD. We hypothesized that bosentan reduces leucocyte adhesion in submucosal venules of the inflamed colon. To assess the effect of bosentan on leucocyte adhesion, we performed in vivo microscopy, a method that allows the observation of leucocyte trafficking in vivo. The number of adhering and rolling leucocytes and the rolling velocity of leucocytes were assessed.
In summary, the target parameters of this study were the clinical (DAI) and histological (Dieleman) scores as well as the in vivo assessment of leucocyte–endothelial interaction.
Materials and methods
Drugs
Animals were treated with bosentan (Ro 47-0203, Hoffmann-La Roche, Basel, Switzerland). Bosentan is an orally active, non-selective endothelin receptor antagonist without intrinsic activity.
Animals
All experiments were conducted according to the institution's guidelines for care and use of laboratory animals. Inbred female BALB/c mice (Charles River, Sulzfeld, Germany; body weight approximately 20 g) were housed in standard cages (two mice in one cage) under stable conditions (light–dark cycle 12:12 h, humidity 60±10%, constant temperature 21±1°C.) The mice had free access to standard laboratory chow and to drinking water or DSS in drinking water, respectively.
Study design
A total of 30 animals were divided into three groups.
Healthy controls
In this group, 10 animals underwent in vivo microscopy without previous treatment, and the colon of 9 animals was removed for histological scoring after in vivo microscopy.
Colitis group
In this group, chronic colitis was induced by cyclic administration of DSS (3% w/v) in drinking water for 30 days (see the section “Induction of colitis”). On days 26–30, animals were treated once a day with 0.1 ml aqua ad injectabilia (vehicle) i.p. On day 30, in vivo microscopy was performed in 10 animals, and the colon was removed for histological scoring in 9 animals.
Colitis+bosentan group
In this group, chronic colitis was induced by cyclic administration of DSS in drinking water for 30 days. On days 26–30, animals were treated with 30 mg bosentan/kg body wt in 0.1 ml aqua ad injectabilia i.p. The last dose was injected in the morning of day 30, and in vivo microscopy was performed in 10 animals in the afternoon. The colon of 9 animals was removed afterward for histological scoring.
Induction of colitis
Chronic colitis was induced by cyclic administration of a 3% w/v solution of DSS (mol. wt. 40 kDa; ICN Biochemicals, Aurora, OH, USA) in drinking water or drinking water alone for 30 days, following the time schedule given in Table 1. Each cycle consisted of 5 days of DSS in drinking water followed by 5 days of drinking water alone. Three cycles were completed (=30 days).
Clinical disease activity index
All animals treated with DSS for induction of chronic colitis were examined once a day and the clinical DAI was assessed, as previously described [22]. The score consists of the following three parameters: weight loss, stool consistency and perianal bleeding. The scoring system is shown in Table 2.
Histological colitis score
After in vivo microscopy, the animals were sacrificed by an overdose of anaesthesia. The whole colon was removed, opened longitudinally and divided into four segments (caecum and appendix, proximal third, middle third, and distal third). For each segment, four different sections were stained with haematoxylin/eosin, making up 16 different sections per animal. The sections were scored using a histological colitis score, as previously described [19]. In brief, for each category of the score (inflammation, extent, crypt damage) points were multiplied with a factor of involvement of the visible epithelium. The sum of the three categories makes up the total score of a section (0–40 points) (Table 3). The average of four sections was representative for the colon segment, and the average of the four colon segments was representative for the whole colon.
In vivo microscopy
Leucocytes were stained in vivo by application of 0.1 ml Rhodamine 6G (0.4 mg/ml) (Sigma-Aldrich, R 4127) 15 min before microscopy [23]. Blood from homologous healthy littermates was collected, anticoagulated with heparin, washed with Bicine buffer, and the erythrocytes were purified with Alsever's buffer. Erythrocytes were labelled in vitro by incubation with fluorescein isothiocyanate (FITC; Sigma Aldrich, F-1628) (9 mg/ml suspension of Erythrocytes) for 60 min [24]. After labelling, erythrocytes were washed several times with Bicine buffer. Labelled erythrocytes were administrated at the beginning of microscopy.
Animals were anaesthetized by inhalation of isoflurane. A polyethylene catheter (inner diameter 0.28 mm, Portex Ltd., UK) was inserted in the right jugular vein as central venous line. The left carotid artery was cannulated to monitor blood pressure and heart rate throughout the experiment. The animals were placed in a supine position on a specially designed heated pedestal. A midline laparotomy was performed, and the small bowel was gently exteriorized and covered with a saline-soaked gauze. The descending colon was gently mobilized and a micromanipulator pedestal was inserted under the colon, providing good access to the exteriorized colon for microscopy. Constant superfusion with 37°C Ringer's lactate and coverage with a cyprophane foil kept the bowel from drying and guaranteed stable conditions for temperature and humidity. After 30 min of equilibration (with stable heart rate and blood pressure), the experimental protocol started with the injection of 0.1 ml FITC-labelled erythrocyte suspension.
In vivo epiluminescence microscopy was performed with a fluorescence microscope (Zeiss, Germany) (light source, HBO 12 V/100 W) using a 450- to 490- or 515- to 565-nm filter for visualization of FITC-labelled erythrocytes, and a 510- to 560- or >590-nm filter for visualization of Rhodamine 6G-stained leucocytes. Using a 16×/0.5-mm water-immersion objective (Plan-Neofluar, Zeiss) and a mounted video camera with 0.5 zoom (FK-6990-IQ, Pieper, Germany), we achieved a 760-fold magnification on video screen (IQM 538, Pieper, Germany). The images were tape-recorded (AG 7350, Panasonic, Germany) for offline analysis.
Using water-immersion technique, we easily identified single, unbranched, submucosal venules with a diameter of approximately 50 μm (2V vessels according to Bohlen and Gore [25]) by the FITC-labelled erythrocytes running through the vessel. For each vessel, a sequence of 30 s was recorded for FITC-labelled erythrocytes, and a sequence of 60 s was recorded for Rhodamine 6G-stained leucocytes. Ten 2V venules were recorded, proceeding from the sigmoid to the left colon flexure.
Offline analysis
Computer-based analysis of the videotapes was performed using a morphometric software (AnalySIS, version 2.11, Soft Imaging Systems, Muenster, Germany). Vessel diameter (D) and centreline velocity of erythrocytes (V ery) were measured. Volumetric flow was calculated with the following formula: Q (nl/min)=(V ery/1.6)(D 2/4)×π×60×10−6 [34]. Shear rate (SR) was calculated based on the definition of Newton: SR (s−1)=8V ery/1.6D [26].
For each vessel, the number of rolling and adherent leucocytes was assessed. Adherent leucocytes were defined as cells attached to the endothelial lining for at least 30 s (given as adherent leucocytes per 0.01 mm2 endothelial surface). Rolling leucocytes were defined as cells that pass an imaginary line across the vessel during 30 s, moving with a lower velocity than that of free-flowing leucocytes (given as rolling leucocytes per 100 μm venular diameter per 30 s). The average of rolling and adherent leucocytes of 10 venules was calculated for each animal. In each vessel, the velocity of five randomly chosen rolling leucocytes was measured by frame-to-frame tracking on the videotape. The average speed for each vessel and for each animal (10 vessels) was calculated. The velocity of rolling leucocytes is a well known indicator of adhesive forces between leucocyte and endothelium [27].
Statistics
All results are given as mean ± SEM. For statistical analysis, the non-parametric Kruskal–Wallis test was used, when appropriate, followed by Dunn's method. A p value <0.05 was considered significant.
Results
Clinical disease activity index
Mice treated with DSS had symptoms of colitis 1–2 days after the start of the first cycle (diarrhoea, weight loss, perianal bleeding). The DAI for the period of 30 days is shown in Fig. 1. The colitis and colitis+bosentan groups had similar DAI up to day 26, when treatment with bosentan started. On day 30, the DAI of bosentan-treated animals was significantly lower (0.8±0.4 vs 1.7±0.5 points, p<0.05).

Disease activity index. For all animals treated with DSS for induction of colitis a DAI was calculated daily. The colitis+bosentan group was treated with bosentan (30 mg/kg body weight i.p.) daily on days 26–30. n=10 animals. Mean±SEM. *, p<0.05 vs colitis+bosentan
Histology
Healthy controls had a normal histological morphology. There were infrequent areas of mild inflammatory infiltrate, leading to a histological colitis score >0 (Fig. 2).

Histology. Healthy control: The epithelium is not altered, mucosal architecture is normal, crypts reach the muscularis mucosae, and there is no inflammatory infiltrate. Colitis: This section shows an entire loss of crypts. The lamina propria and submucosa show a moderate inflammatory infiltrate. On the left side, the surface epithelium is lost, on the right side it is retained. Colitis+Bosentan: The epithelium is not altered; mucosal architecture is normal. There is no inflammation
Sections of the colitis group showed all characteristics of a chronic DSS-induced colitis, as previously described [22]. There were dense infiltrates of leucocytes, mostly pronounced in mucosa and submucosa, crypt shortening or even crypt drop out, and focal loss of epithelium. Alterations were rather focal (Fig. 2).
Sections of the colitis+bosentan group showed similar characteristics as the colitis group; however, inflammation was milder. Low-grade lesions were more frequent, and many areas appeared completely normal (Fig. 2).
The histological colitis score for the different segments of the colon and for the entire colon is shown in Fig. 3. In the colitis group, the score for the entire colon was 9.15-fold higher than in healthy controls (p<0.05). Compared with the colitis group, treatment with bosentan reduced the score by 42.4% (p<0.05). However, the score was still significantly higher than in healthy controls (p<0.05).

Histological colitis score. Left, the histological colitis score for the different segments of the colon. Right, the histological colitis score for the complete colon. n=9 animals. Mean±SEM. *, p<0.05 vs healthy controls; §, p<0.05 vs colitis group
Leucocyte adhesion
Venular diameters, centreline velocity of erythrocytes and volumetric flow were significantly higher in the colitis+bosentan group compared to the colitis group; however, shear rate was not different in the three groups (Table 4).
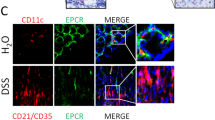
Leucocyte adhesion was visualized by in vivo microscopy (Fig. 4). The number of adherent leucocytes was significantly higher in the colitis group than in healthy controls (p<0.05, Fig. 5). Treatment with bosentan reduced the number to values of healthy controls (p<0.05 vs colitis group, not significant vs healthy controls, Fig. 5).

In vivo microscopy. Vessels can be identified as dark structures on a bright background. Adhering leucocytes are visualized as bright spots in the vessels. Colitis: Many rolling and firmly adhering leucocytes are found in the vessel (rolling and adhering leucocytes cannot be differentiated in a photo). Colitis+Bosentan: In animals treated with bosentan, only few adhering leucocytes can be found in the vessels

Rolling leucocytes in colonic submucosal venules. Leucocytes crossing a line transverse to the vessel during a period of 30 s with a velocity lower than that of free-flowing leucocytes were counted as rolling leucocytes. n=10 animals. Mean±SEM. *, p<0.05 vs healthy controls
The number of rolling leucocytes was markedly higher in the colitis and colitis+bosentan groups compared to healthy controls (p<0.05). Although numbers were lower, there was no significant difference between the colitis+bosentan group and the colitis group (Fig. 6).

Sticking leucocytes in colonic submucosal venules. Leucocytes were defined as firmly adherent if adhering to the endothelial lining for 30 s without movement. n=10 animals. Mean±SEM. *, p<0.05 vs healthy controls and vs colitis+bosentan group
Rolling velocity was significantly lower in the colitis group compared to healthy controls (p<0.05, Fig. 7). With bosentan therapy, leucocytes were significantly faster than in the colitis group (p<0.05). There was a tendency toward a higher velocity compared to healthy controls; however, there was no statistical difference.

Velocity of rolling leucocytes. The average velocity was calculated by frame-to-frame tracking on the videotape. n=10 animals. Mean±SEM. *, p<0.05 vs colitis group
Discussion
This study demonstrates that bosentan reduces the number of adherent leucocytes in submucosal venules of the inflamed colon and increases the velocity of rolling leucocytes in a well-defined animal model of IBD. Bosentan reduced clinical and histological inflammation in chronic colitis.
An increase in the number of adherent and rolling leucocytes, as found in the colitis group, is a typical feature of chronic intestinal inflammation [28, 29]. A slow rolling velocity in the colitis group indicates strong adhesive forces between leucocyte and endothelium [27].
Increased leucocyte adhesion, especially the firm adherence on the endothelial line, is a crucial and rate-limiting step in the development of a cellular inflammatory infiltrate in the colonic tissue. Therapeutic strategies blocking leucocyte adhesion were effective in reducing intestinal inflammation, as we and other authors have shown before [28–30].
Therefore, the decrease in number of adherent leucocytes in the inflamed colon by bosentan treatment is a key finding of this study. Probably, a reduction of adherent leucocytes leads to a reduction of the cellular inflammatory infiltrate developed by extravasation of firmly adhering leucocytes. This might explain the reduction of inflammation by bosentan therapy observed in this study.
The number of rolling leucocytes was not altered by bosentan therapy compared to untreated animals of the colitis group. However, although the number was not different, the adhesive activity of the rolling leucocytes was markedly different. In the colitis group, rolling leucocytes travelled very slowly, only differing from an adherent leucocyte by a minimal movement over 30 s. In the colitis+bosentan group, leucocytes rolled dramatically faster; there was even a (non-significant) tendency toward higher velocities than in healthy controls. Obviously, leucocytes were in a state of lower adhesive activity with bosentan therapy, as high rolling velocity is a well-recognized indicator of low adhesive forces [27].
The mechanisms of bosentan-induced reduction of leucocyte firm adherence remain speculative. Probably, the endothelin receptor antagonist bosentan blocks the endothelin-induced up-regulation of cell adhesion molecules on the endothelium and leucocytes [10–13, 15, 16]. In particular, the finding that the anti-inflammatory effects of endothelin are mediated by vascular cell adhesion molecule 1 (VCAM-1) [11] in isolated endothelial cells suggests that this cell adhesion molecule may play a role in the attenuation of sticking and the elevation of rolling velocity in our study. However, treatment with an anti VCAM-1 oligonucleotide [29] in a similar experimental setting (DSS-induced colitis) exerts a more potent protective effect on leucocyte endothelial adhesion when compared to bosentan, suggesting that whereas bosentan may act via the down-regulation of VCAM-1, this endothelin receptor antagonist is not as potent an inhibitor of VCAM-1. Furthermore, bosentan could reduce the release of secondary mediators, such as IL-1, IL-6, IL-8 or TNF-α, produced by monocytes stimulated with endothelin [6, 7]. Many of these mediators increase expression of cell adhesion molecules and induce leucocyte adhesion [31, 32]. Finally, blockade of the vasoconstrictive properties of endothelins by bosentan could increase flow and flow velocity in the vessels, thus inhibiting leucocyte adhesion. Indeed, flow and centreline velocity were significantly higher in the colitis+bosentan group compared to the colitis group. However, leucocyte adhesion depends on shear rate more than on flow: low shear rate means strong adhesive forces [33–36]. It is a striking fact that the shear rate was not different in the three groups. As vessel diameter and centreline velocity increase similarly, shear rate remains constant.
Bosentan therapy reduced the DAI, compared to untreated animals, by approximately 50%. This finding is consistent with findings of Hogaboam et al. [17] and Güllüoglu et al. [18], who demonstrated a reduction of clinical activity of TNBS-induced colitis in rats by prophylactic bosentan treatment, suggesting that the anti-inflammatory effect of bosentan in IBD is not dependent on the animal model used. The novel finding in our study comes from the experimental approach, wherein bosentan was shown to effectively reduce the clinical disease activity of chronic colitis in a therapeutic setting, with the therapy starting when the colitis was already fully established. This is in contrast to the previous studies mentioned above wherein bosentan was administered in a prophylactic experimental setting. Hogaboam et al. could not see a significant effect of bosentan therapy starting 60 min after induction of rat colitis with TNBS [17]. First, this might be due to the special characteristics of TNBS-induced colitis, including a direct toxicity of the carrier, ethanol, to the intestinal mucosa. Second, the parenteral application used in this study might be superior to the oral administration used before [18, 17].
Bosentan therapy reduced histological colitis score by 42% compared to untreated animals with DSS-induced colitis. Thus, for the first time, the impression of former studies that bosentan can reduce histological inflammation in an animal model of IBD could be statistically secured [18, 17]. In several other animal models, the blockade of endothelin receptors effectively reduced tissue injury: acute pancreatitis [37], malignant hypertension [38, 39], ischaemia/reperfusion injury of the liver [40–42] and myocarditis [43].
No complete remission of histological inflammation was achieved by bosentan therapy, although gut mucosa was able to regenerate within a few days [44]. There might be several reasons for the incomplete histological healing. First, endothelins are only one among many factors playing a role in the pathogenesis of DSS-induced colitis. Cytokines, cellular reactions and oxygen metabolites are involved [19–21]. Second, DSS inhibits mucosal regeneration by reducing cell proliferation rate and cell viability [45]. Indeed, DSS-induced alterations of colon mucosa show prolonged healing [19]. It is possible that longer therapy, beyond day 30, would have further improved histological healing. This could be evaluated in future studies.
One aim of the study was to clarify the anti-inflammatory mechanism of bosentan. First, as this study demonstrates, bosentan impairs leucocyte adhesion necessary for recruitment of leucocytes to the gut mucosa. Second, the parenteral application of bosentan used in this study can inhibit further proinflammatory actions of endothelins, e.g. the release of proinflammatory mediators from leucocytes [6, 7], the provocation of local ischaemia and the impairment of mucosal barrier for luminal antigens [8]. Further studies are necessary to clarify the anti-inflammatory action of bosentan in IBD.
In clinical studies, bosentan was shown to be effective in the treatment of symptomatic heart failure [46–48], primary pulmonary hypertension [49, 50], coronary artery disease [51] or essential hypertension [52]. It is an orally active, well-tolerated drug [53, 54].
These promising clinical results, the involvement of endothelins in the pathogenesis of IBD, and results of experimental studies such as the one presented here encourage further investigation of a potential use of endothelin antagonists in patients with IBD.
References
Yanagisawa M, Kurihara H, Kimura S, Tomobe Y, Kobayashi M, Mitsui Y, Yazaki Y, Goto K, Masaki T (1988) A novel potent vasoconstrictor peptide produced by vascular endothelial cells. Nature 332:411–415
McMillen MA, Sumpio BE (1995) Endothelins: polyfunctional cytokines. J Am Coll Surg 180(5):621–637
Letizia C, Boirivant M, De Toma G, Cerci S, Subioli S, Scuro L, Ferrari P, Pallone F (1998) Plasma levels of endothelin-1 in patients with Crohn's disease and ulcerative colitis. Ital J Gastroenterol Hepatol 30:266–269
Murch SH, Braegger CP, Sessa WC, MacDonald TT (1992) High endothelin-1 immunoreactivity in Crohn's disease and ulcerative colitis. Lancet 339:381–385
Hudson M, Dashwood MR, Pounder RE, Wakefield AJ (1994) [125I] Endothelin-1 binding in normal human intestine and in inflammatory bowel disease. Gastroenterology 106(4):A239 (AGA-Abstract)
Cunningham ME, Huribal M, Bala RJ, McMillen MA (1997) Endothelin-1 and endothelin-4 stimulate monocyte production of cytokines. Crit Care Med 25(6):958–964
McMillen MA, Huribal M, Kumar R, Sumpio BE (1993) Endothelin-stimulated human monocytes produce prostaglandin E2 but not leukotriene B4. J Surg Res 54(4):331–335
Oktar BK, Coskun T, Bozkurt A, Yegen BC, Yüksel M, Haklar G, Bilsel S, Aksungar FB, Cetinel S, Granger DN, Kurtel H (2000) Endothelin-1-induced PMN infiltration and mucosal dysfunction in the rat small intestine. Am J Physiol Gasterointest Liver Physiol 42:G483–G491
Boros M, Massberg S, Baranyi L, Okada H, Messmer K (1998) Endothelin 1 induces leukocyte adhesion in submucosal venules of the rat small intestine. Gastroenterology 114:103–114
Sanz MJ, Johnston B, Issekutz A, Kubes P (1999) Endothelin-1 causes P-selectin-dependent leukocyte rolling and adhesion within rat mesenteric microvessels. Am J Physiol 277:H1823–H1830 (Heart Circ Physiol 46)
Ishizuka T, Takamizawa-Matsumoto M, Suzuki K, Kurita A (1999) Endothelin-1 enhances vascular cell adhesion molecule-1 expression in tumor necrosis factor α-stimulated vascular endothelial cells. Eur J Pharmacol 369:237–245
López Farré A, Riesco A, Espinosa G, Digiuni E, Cernadas MR, Alvarez V, Montón M, Rivas F, Gallego MJ, Egido J, Casado S, Caramelo C (1993) Effect of endothelin-1 on neutrophil adhesion to endothelial cells and perfused heart. Circulation 88(3):1166–1171
McCarron RM, Wang L, Stanimirovic DB, Spatz M (1993) Endothelin induction of adhesion molecule expression on human brain microvascular endothelial cells. Neurosci Lett 156:31–34
Schwarting A, Schlaak J, Lotz J, Pfers I, Meyer zum Büschenfelde K-H, Mayet W-J (1996) Endothelin-1 modulates the expression of adhesion molecules on fibroblast-like synovial cells (FLS). Scand J Rheumatol 25:246–256
Zouki C, Baron C, Fournier A, Filep JG (1999) Endothelin-1 enhances neutrophil adhesion to human coronary artery endothelial cells: role of ETA receptors and platelet-activating factor. Br J Pharmacol 127:969–979
Hayasaki Y, Nakajima M, Kitano Y, Iwasaki T, Shimamura T, Iwaki K (1996) ICAM-1 expression on cardiac myocytes and aortic endothelial cells via their specific endothelin receptor subtype. Biochem Biophys Res Commun 229(3):817–824
Hogaboam CM, Muller MJ, Collins SM, Hunt RH (1996) An orally active non-selective endothelin receptor antagonist, bosentan, markedly reduces injury in a rat model of colitis. Eur J Pharmacol 309(3):261–269
Güllüoglu BM, Kurtel H, Güllüoglu MG, Yegen C, Aktan AÖ, Dizdaroglu F, Yalin R, Yegen BC (1999) Role of endothelins in trinitrobenzene sulfonic acid-induced colitis in rats. Digestion 60:484–492
Dieleman LA, Palmen MJHJ, Akol H, Bloemena E, Pena AS, Meuwissen SGM (1998) Chronic experimental colitis induced by dextran sulphate sodium (DSS) is characterized by Th1 and Th2 cytokines. Clin Exp Immunol 114:385–391
Egger B, Bajaj-Elliott M, MacDonald TT, Inglin R, Eysselein VE, Büchler MW (2000) Characterisation of acute murine dextran sodium sulphate colitis: cytokine profile and dose dependency. Digestion 62:240–248
Okayasu I, Hatakeyama S, Yamada M, Ohkusa T, Inagaki Y, Nakaya R (1990) A novel method in the induction of reliable experimental acute and chronic ulcerative colitis in mice. Gastroenterology 98(3):694–702
Cooper HS, Murthy SNS, Shah RS, Sedergran DJ (1993) Clinicopathologic study of dextran sulfate sodium experimental murine colitis. Lab Invest 69(2):238–249
Baatz H, Seinbauer M, Harris AG, Krombach F (1995) Kinetics of white blood cell staining by intravascular administration of Rhodamine 6G. Int J Microcirc Clin Exp 15(2):85–91
Butcher EC, Weissmann IL (1980) Direct fluorescent labeling of cells with fluorescein or rhodamine isothiocyanate. J Immunol Methods 37:97–108
Bohlen HG, Gore RW (1976) Preparation of rat intestinal muscle and mucosa for quantitative microcirculatory studies. Microvasc Res 11:103–110
Ritter LS, Orozco JA, Coull BM, McDonagh PF (2000) Leukocyte accumulation and hemodynamic changes in the cerebral microcirculation during early reperfusion after stroke. Stroke 31:1153–1161
Lipowsky HH, Scott DA, Cartmell JS (1996) Leukocyte rolling velocity and its relation to leukocyte-endothelium adhesion and cell deformability. Am J Physiol 270:H1371–H1380 (Heart Circ Physiol 39)
Krieglstein CF, Anthoni C, Laukötter MG, Rijcken E, Spiegel HU, Senninger N, Schurmann G (1999) Effect of anti-CD11b (alphaM-MAC-1) and anti-CD54 (ICAM-1) monoclonal antibodies on indomethacin induced chronic ileitis in rats. Int J Colorectal Dis 14(4–5):219–223
Rijcken E, Krieglstein CF, Anthoni C, Laukötter MG, Mennigen R, Spiegel HU, Senninger N, Bennett CF, Schuermann G (2002) ICAM-1 and VCAM-1 antisense oligonucleotides attenuate in vivo leukocyte adherence and inflammation in rat inflammatory bowel disease. Gut 51(4):529–535
Yacyshyn BR, Chey WY, Goff J, Salzberg B, Baerg R, Buchman AL, Tami J, Yu R, Gibiansky E, Shanahan WR, ISIS 2302-CS9 Investigators (2002) Double blind, placebo controlled trial of the remission inducing and steroid sparing properties of an ICAM-1 antisense oligodeoxynucleotide, alicaforsen (ISIS 2302), in active steroid dependent Crohn's disease. Gut 51(1):30–36
Arndt H, Bolanowski MA, Granger DN (1996) Role of interleukin 8 on leucocyte–endothelial cell adhesion in intestinal inflammation. Gut 38:911–915
Panés J, Granger DN (1998) Leukocyte–endothelial cell interactions: molecular mechanisms and implications in gastrointestinal disease. Gastroenterology 114(5):1066–1090
Bienvenue K, Granger DN (1993) Molecular deteminants of shear rate-dependent leukocyte adhesion in postcapillary venules. Am J Physiol 264:H1504–H1508 (Heart Circ Physiol 33)
House SD, Lipowsky HH (1987) Leukocyte–endothelium adhesion: microhemodynamics in mesentery of the cat. Microvasc Res 34(3):363–379
Ley K, Gaehtgens P (1991) Endothelial, not hemodynamic, differences are responsible for preferential leukocyte rolling in rat mesenteric venules. Circ Res 69(4):1034–1041
Ritter LS, McDonagh PF (1997) Low-flow reperfusion after myocardial ischemia enhances leukocyte accumulation in coronary microcirculation. Am J Physiol 273:H1154–H1165 (Heart Circ Physiol 42)
Foitzik T, Eibl G, Buhr HJ (2000) Therapy for microcirculatory disorders in severe acute pancreatitis: comparison of delayed therapy with ICAM-1 antibodies and a specific endothelin A receptor antagonist. J Gastrointest Surg 4(3):240–247
Karam H, Heudes D, Bruneval P, Gonzales M-F, Loffler B-M, Clozel M, Clozel J-P (1996) Endothelin antagonism in end-organ damage of spontaneously hypertensive rats. Hypertension 28(3):379–385
Kohno M, Yokokawa K, Yasunari K, Kano H, Minami M, Ueda M, Tatsumi Y, Yoshikawa J (1997) Renoprotective effects of a combined endothelin type A/type B receptor antagonist in experimental malignant hypertension. Metabolism 46(9):1032–1038
Kitayama Y, Yamanaka N, Kawamura E, Kuroda N, Okamoto E (1997) Hepatoprotective effect of the endothelin receptor antagonist TAK-044 against ischemia–reperfusion injury in the canine liver. Hepatology 25:938–942
Spiegel HU, Uhlmann D, Scommotau S, Giersch B, Sulkowski U (1996) Effect of the endothelin receptor antagonist bosentan on postischemic oxygen supply of the liver. J Invest Surg 9(6):439–445
Spiegel HU, Scommotau S, Uhlmann D, Giersch B (1996) Effect of the endothelin receptor antagonist bosentan on postischemic liver microcirculation. Zentralbl Chir 121(9):788–793
Ono K, Matsumori A, Shioi T, Furukawa Y, Sasayama S (1999) Contribution of endothelin-1 to myocardial injury in a murine model of myocarditis. Circulation 100:1823–1829
Elson CO, Sartor RB, Tennyson GS, Riddell RH (1995) Experimental models of inflammatory bowel disease. Gastroenterology 109:1344–1367
Dieleman LA, Ridwan BU, Tennyson GS, Beagley KW, Bucy RP, Elson CO (1994) Dextran sulfate sodium-induced colitis occurs in severe combined immunodeficient mice. Gastroenterology 107:1643–1652
Givertz MM, Colucci WS, LeJemtel TH, Gottlieb SS, Hare JM, Slawsky MT, Leier CV, Loh E, Nicklas JM, Lewis BE (2000) Acute endothelin A receptor blockade causes selective pulmonary vasodilation in patients with chronic heart failure. Circulation 101(25):2922–2927
Mylona P, Cleland JGF (1999) Update of REACH-1 and MERIT-HF clinical trials in heart failure. Eur J Heart Fail 1(2):197–200
Sütsch G, Kiowski W, Yan X-W, Hunziker P, Christen S, Strobel W, Kim J-H, Rickenbacher P, Bertel O (1998) Short-term oral endothelin-receptor antagonist therapy in conventionally treated patients with symptomatic severe chronic heart failure. Circulation 98:2262–2268
Channick RN, Simonneau G, Sitbon O, Robbins IM, Frost A, Tapson VF, Badesch DB, Roux S, Rainisio M, Bodin F, Rubin LJ (2001) Effects of the dual endothelin-receptor antagonist bosentan in patients with pulmonary hypertension: a randomised placebo-controlled study. Lancet 358:1119–1123
Williamson DJ, Wallman LL, Jones R, Keogh AM, Scroope F, Penny R, Weber C, MacDonald PS (2000) Hemodynamic effects of bosentan, an endothelin receptor antagonist, in patients with pulmonary hypertension. Circulation 102(4):411–418
Wenzel RR, Fleisch M, Shaw S, Noll G, Kaufmann U, Schmitt R, Jones CR, Clozel M, Meier B, Lüscher TF (1998) Hemodynamic and coronary effects of the endothelin antagonist bosentan in patients with coronary artery disease. Circulation 98:2235–2240
Krum H, Viskoper RJ, Lacourciere Y, Budde M, Charlon V (1998) The effect of an endothelin-receptor antagonist, bosentan, on blood pressure in patients with essential hypertension. N Engl J Med 338(12):784–790
Weber C, Schmitt R, Birnboeck H, Hopfgartner G, van Marle SP, Peeters PA, Jonkman JH, Jones CR (1996) Pharmacokinetics and pharmacodynamics of the endothelin-receptor antagonist bosentan in healthy human subjects. Clin Pharmacol Ther 60(2):124–137
Weber C, Schmitt R, Birnboeck H, Hopfgartner G, Eggers H, Meyer J, van Marle S, Viischer HW, Jonkman JH (1999) Multiple-dose pharmacokinetics, safety, and tolerability of bosentan, an endothelin receptor antagonist, in healthy male volunteers. J Clin Pharmacol 39(7):703–714
Acknowledgements
This work was supported by a grant of the Crohn's and Colitis Foundation of Germany, DCCV eV.
Author information
Authors and Affiliations
Corresponding author
Additional information
C. Anthoni and R.B. Mennigen contributed equally to this work
Rights and permissions
About this article
Cite this article
Anthoni, C., Mennigen, R.B., Rijcken, E.J.M. et al. Bosentan, an endothelin receptor antagonist, reduces leucocyte adhesion and inflammation in a murine model of inflammatory bowel disease. Int J Colorectal Dis 21, 409–418 (2006). https://doi.org/10.1007/s00384-005-0015-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00384-005-0015-3