
Abstract
Suction rectal biopsy (SRB) may not include sufficient submucosa for histological diagnosis of Hirschsprung’s disease (HD) and a repeat biopsy is required. Substitution of the conventional syringe for sustained suction from a machine or wall suction unit could provide a more consistently adequate tissue biopsy. This study was conducted to compare the adequacy of SRB specimens using a conventional method of syringe suction (SSRB) with those taken by wall or machine suction (WSRB). Hospital records of patients who had a SRB between 2002 and 2004 were studied retrospectively. The biopsy was considered inadequate if there was insufficient submucosa and a repeat specimen was requested. SSRB were taken using the conventional SSRB technique. WSRB were taken with the same Noblett forceps but with suction from wall suction or from a portable suction machine. Ninety-five infants had 103 SRB, 24 had WSRB and all (100%) were adequate for histopathological diagnosis or exclusion of HD. Seventy nine conventional SSRB were undertaken in 71 infants of which 64 (81.02%) were adequate. The difference in adequacy between WSRB and SSRB was statistically significant (P = 0.02). There were no instances of haemorrhage or bowel perforation in either subgroup. WSRB with the Noblett biopsy forceps is more likely to produce an adequate specimen and to reduce the incidence of repeat biopsies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rectal mucosal suction biopsy (SRB) is usually successful for the diagnosis of Hirschsprung’s disease (HD) in the neonates and infants. However, the biopsy specimen may not include sufficient submucosa for histological assessment and a deeper repeat biopsy under general anaesthesia is then necessary. Substitution of the conventional syringe for sustained controlled suction from a low grade machine or ‘wall’ suction unit may provide a more consistent biopsy specimen with the appropriate submucosal layer, thereby reducing the need for repeat biopsy.
This study was conducted to compare the conventional method of syringe suction (SSRB) biopsy with biopsy specimens taken by wall or machine suction (WSRB), and to explore the null hypothesis that controlled suction does not improve the adequacy of rectal biopsy from suction rectal biopsy apparatus.
Materials and methods
This was a retrospective study of the hospital records (patient case notes and histopathology laboratory database) of patients who had a RSB at Manchsester Children’s Hospitals between January 2002 and February 2004. The biopsy was considered adequate when the histopathology report unequivocally identified normal ganglia and refuted HD, or when there was a confident diagnosis of HD based on absence of ganglia, enlarged nerve trunks and raised acetylcholinesterase levels. The biopsy was considered inadequate if there was insufficient submucosa and a repeat specimen was requested. Specimens considered to be from the ‘normal’ aganglionic zone were excluded.
Syringe suction were taken using the conventional SSRB technique as described by Noblett [1]. WSRB were taken with the same Noblett forceps but with suction from a central source (wall suction) or from a portable suction machine. All connections were pre-tested to exclude leakage, and the degree of suction produced at the sampling hole was tested with the operator’s gloved finger and the wall suction at its maximum.
With the assistant supporting the child in the lithotomy position and the wall suction turned off, the lubricated biopsy forceps was advanced along the posterior rectal wall. The sampling hole was applied firmly 2–3 cm above the dentate line and the cutting blade was opened. The wall suction was allowed to reach a suction pressure of 500 mmHg (65 KPA) and held for 5–10 s, when the cutting blade was advanced to take the biopsy. Two to three biopsies were taken and dispatched on ice directly to histopathology for haematoxylin &and eosin stain and acetyl-cholinesterase activity.
Results
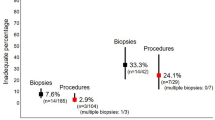
Between January 2002 and February 2004 January 95 infants had 103 SRB (Table 1). WSRB was undertaken on 24 babies (M:F 7:17, age range 1–84 days with a median age 19 days) and all biopsies (100%) were adequate for an unequivocal histopathological diagnosis of HD in 2 infants and normal findings in 22. Seventy-nine conventional SSRB were undertaken in 71 infants (M:F 32:39, age range 1–147 days with a median age of 17 days) of which 64 (81.02%) were adequate for a diagnosis of HD in 5 and normal findings in 59. Fifteen biopsies (18.98%) were inadequate such that six infants had a single repeat biopsy and one child had the biopsy repeated twice. General anaesthesia was used on one occasion for the repeat biopsy. Re-biopsies were undertaken at a median of 6 days, range 2–40 days. Using Fisher’s exact test, the difference in adequacy between WSRB and SSRB was statistically significant at P = 0.02. There were no instances of haemorrhage or bowel perforation in either subgroup.
Discussion
The need for accurate diagnosis is crucial to appropriate management of HD in the neonate. Inadequate suction rectal biopsy (SRB) specimens generate delay in diagnosis with additional anxiety for the parents and irritation and overwork for the pathologist. The SRB without anaesthesia has proved invaluable but carries a failure rate and some have recommend alternative techniques to optimize the yield [2, 3] and to facilitate simpler operation [4]. Success depends on a sharp clean-cutting blade and the ability to achieve adequate sustained suction. It is relevant to note that no additional equipment is required since easy-to-use facilities capable of controlled sustained suction are available as standard bed-side apparatus. By replacing SSRB with controlled sustained WSRB we were able to ensure an adequate volume of submucosa in all specimens obtained from 24 babies. We therefore recommend wall or machine suction with the Noblett biopsy forceps as more likely to produce an adequate specimen and to reduce the incidence of repeat biopsies.
References
Noblett H (1969) A rectal suction biopsy tube for use in the diagnosis of Hirschsprung’s disease. J Pediatr Surg 4:406–409
Alizai NK, Batcup G, Dixon MF et al (1998) Rectal biopsy for Hirschsprung’s disease: what is the optimum method? Pediatr Surg Int 13:121–124
Kobayashi H, Li Zh, Yamataka A et al (2002) Rectal biopsy: what is the ultimate procedure? Pediatr Surg Int 18:753–756
Pini PA, Martucciello G, Jasonni V (2001) Solo-RBT: a new instrument for rectal suction biopsies in the diagnosis of Hirschsprung’s disease. J Pediatr Surg 36:1364–1366
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ali, A.E., Morecroft, J.A., Bowen, J.C. et al. Wall or machine suction rectal biopsy for Hirschsprung’s disease: a simple modified technique can improve the adequacy of biopsy. Pediatr Surg Int 22, 681–682 (2006). https://doi.org/10.1007/s00383-006-1714-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00383-006-1714-8