
Abstract
Introduction
Extrapulmonary skeletal involvement of calvarium in tuberculosis is very uncommon and presentation in an infant has never been reported. It usually presents as a painless scalp swelling, often with a discharging sinus.
Discussion
We report here a case of extensive calvarial tuberculosis seen in an infant presenting as exophytic ulcerated growth on the scalp. Differential diagnosis, neuroimaging, and management issues with pertinent literature are reviewed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Calvarial involvement in tubercular disease is rare, and primary calvarial tuberculosis (CTB) is even rarer, without any evidence of tuberculosis elsewhere in the body [12]. It accounts for less than 1 % of all cases of skeletal tuberculosis [12]. It commonly presents as a painless scalp swelling, often associated with a discharging sinus and most commonly involves the frontal and parietal bones. A high index of suspicion and awareness of this condition is necessary among physicians due to its diverse presentation. Because of its infrequency, the condition is misdiagnosed often as bacterial osteomyelitis/histiocytosis X/malignancy/hemangioma/growing skull fracture especially in children.
Case report
A 10-month-old female baby presented with history of fall from bed 6 months back. Her parents noticed a boggy swelling on the affected site of the head, which later burst and presented as elevated granulomatous growth with on and off discharge from the swelling (Fig. 2a). There was no history of fever, cough, weight loss, or night sweats and without any history of tubercular contact in family. On examination, the patient was afebrile with unremarkable systemic examination. In the scalp, there was a single, nonpulsatile, nontender, fluctuant, soft tissue swelling of size 4 × 4 cm near the right parietal eminence with positive crying impulse with 2 × 3 cm grayish red exophytic granulomatous growth in the center with palpable underlying bony defect of 4 × 3 cm size (Fig. 2a).
Laboratory investigations were normal except for elevated erythrocyte sedimentation rate with normal routine chest roentgenogram (PA view). Imprint cytology was inconclusive and wound swab cultures were sterile. Serial computed tomography (CT) scans showed progressive increase in size of boggy swelling with punched out bone defect with both subgaleal and extradural collection with intact dura with few other discrete punched out bone defects (Fig. 1a and b). Magnetic resonance imaging revealed well-defined area of osteolysis in the right parietal bone with subgaleal and extradural lesion with intact dura with postcontrast heterogenous enhancement with multiple smaller foci of patchy enhancement and osteolysis seen in frontotemporal region of both sides (Fig. 1c–f). With conventional radiography and laboratory investigations, the possibility of neoplastic etiology could not be ruled out.

a NCCT head bone window and b CECT head demonstrating large 6 × 4 × 2 cm sized enhancing soft tissue with osteolysis of right parietal bone with few discrete osteolytic lesions in temporo-orbital region and at vertex, lesion is limited by dura without intra-axial extension. c–f Magnetic resonance imaging axial section showing well-defined area of osteolysis in the right parietal bone. The lytic area with subgaleal lesion appears mildly hyperintense on T1FLAIR (c) and isointense on T2 FLAIR (d). GE (Gradient Echo) sequence in e shows hypointense lesion and postcontrast heterogenous enhancement with osteolysis is seen in f. Smaller foci of patchy enhancement with osteolysis are also seen in frontotemporal region of both sides
The right frontotemporoparietal scalp flap was raised and a pedicled pericranium graft was elevated (Fig. 2b). The right frontoparietal craniotomy flap with 2 cm margin of bone all around the defect was raised (Fig. 2c). The subgaleal and extradural granulomatous and necrotic tissue excised along with curetting of unhealthy bone margins (Fig. 2d and e). Frozen section biopsy was suggestive of inflammatory granulation tissue with caseation necrosis. For bone reconstruction, two ribs were harvested as free bone graft and separated into inner and outer table, spread over the defect, and sutured with margins of bone defect using nylon 3/0 sutures (Fig. 2f). Vascularized pedicled pericranium graft was spread over the bone defect with rib graft in place. The wound was closed in layers. Postoperative course was uneventful and patient was discharged on postoperative day 5 and started on antituberculous therapy. Histopathology from the granulomatous growth and bone margins showed multiple Langhans giant cells, wide areas of necrosis, areas of hemorrhages, lymphocytes and neutrophils, and focal areas of calcification and positive AFB, consistent with tuberculosis. Patient was doing fine at 6 months and is on follow up.

a Exophytic ulcerated growth 2 × 3 cm seen in right parital region. b Intraoperative photograph showing yellowish caseating granulation tissue with bone destruction. c A wide craniotomy with 2–3 cm margins is made, granulation tissue is seen easily separating from dural surface. d Intact dural surface is seen after dissecting off the granulation tissue. e Large bony defect 6.5 × 5.5 cm is seen following curetting off unhealthy bone margins. f Rib graft used for covering the defect in sutured with nylon 3/0 sutures in place
Discussion
Tuberculous involvement of calvarium is uncommon compared to other osseous involvement. The disease affects bones in 1 % of cases and the involvement of skull occurs in 0.2–1.37 % of these [5, 7, 8]. Since the Strauss’s review in 1933 [12], some short series and numerous case reports have appeared [1, 2, 5, 7, 8, 10, 11]. The dura is extremely resistant to cranial tuberculosis [6] but few cases are associated with intradural tuberculosis such as meningitis or brain tuberculomas [1, 6].
CTB may present as an insidious onset subgaleal swelling (Pott’s puffy tumor) [2] with a nonhealing discharging sinus when the outer table is involved. Involvement of the inner table is associated with formation of underlying extradural granulation tissue. The dura acts as a strong barrier to its intradural spread [12] but few cases are associated with intradural tuberculosis such as meningitis or brain tuberculomas [7, 12]. The most common route is the hematogenous seeding of Mycobacterium bacilli to the cancellous dipole.
CTB presenting with exophytic ulcerated granulomatous growth is extremely rare, and not a single case reported so far in the medical literature. It most commonly involves the frontal and parietal bones which are rich in cancellous bone [7]. It commonly affects younger population 10–20 years old [7, 8] but relatively rare in children less than 5 year old due to lack of cancellous bone in calvarium, but not a single case has been reported in an infant less than 1 year. Many authors [5, 11, 12] have hypothesized that trauma or surgery is a predisposing factor in the formation of bony lesions probably related to increased vascularity, decreased resistance, and unmasking of a latent infection secondary to trauma. However, Meng [7] and Barton [1] challenged the significance of trauma as they found no patient with a history of head injury in their series
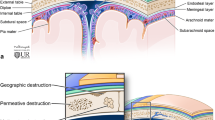
Volkman described “perforating tuberculosis of the skull” as small punched-out lesions with granulation tissue covering both the inner and outer tables of the calvaria [13]. They are commonly known as circumscribed lytic lesions, have little tendency to spread and are usually not associated with periosteal reaction. There is a characteristic sharply circumscribed destruction of both the tables of skull, without causing sclerosis and clinically presenting as a fluctuant, soft tissue, sometimes pulsatile swelling due to bone destruction [4]. Koening in 1888 described “diffuse spreading type of tuberculosis of the cranium” for multiple lesions causing widespread destruction of the skull [6].
Plain X-ray of the skull can be helpful. Areas of rarefaction are seen early in the disease, which develop into punched-out defects with a central sequestrum later on [9]. Both osteolytic and osteoblastic areas may be seen [3, 9]. Rarely, sclerosis may be seen and indicates secondary infection [3, 8].
CT establishes soft tissue swelling with associated destruction of one or both skull tables along with bony sequestrum. It also demonstrates disease spread to the extradural space, meninges, and brain parenchyma [9]. Extradural granulation tissue appears as crescentic or lentiform low-attenuation collection. The surrounding meninges may intensely enhance following contrast medium administration [9]. The CT scan picture of tuberculous osteomyelitis is not very specific and the differential diagnoses include pyogenic osteomyelitis, calvarial metastases, multiple myeloma, hemangioma, giant cell tumor, or even an aneurysmal bone cyst and Langerhans cell histiocytosis [3].
Magnetic resonance imaging can lead to a conclusive diagnosis in most cases. Proton density and T2-weighted images show a high-signal intensity soft tissue mass within the defect in bone (Figs. 1 and 2). This may project into the subgaleal and/or epidural spaces and show peripheral capsular enhancement on the contrast-enhanced image [9]. MR imaging is also sensitive in demonstrating changes in the meninges, ventricular walls, and in detecting parenchymal foci of involvement [9].
Microbiologic or histologic confirmation is essential before starting antituberculous therapy (ATT). The demonstration of acid-fast bacilli in pus smear by using Ziehl–Nelsen stain or isolation of mycobacteria from culture is diagnostic [3]. Microscopic examination reveals a preponderance of lymphocytes, Langhans giant cells, and multiple epithelioid and polymorphonuclear cells with proliferating blood vessels. The presence of caseous granulomas on histopathologic examination provides the most conclusive evidence of tuberculosis infection. Smears and cultures are often negative.
Treatment involves surgery and ATT. Debridement of sequestration not only provides tissue for biopsy but also helps in accelerated healing [8, 10]. Extradural granulation tissue and the involved bone should be removed until normal bone is encountered. The dura mater should be left undisturbed. The indications of surgery appear to be extradural collection, presence of a large sequestrum, and a doubtful diagnosis. Once thorough debridement of granulation tissue and unhealthy bone and toileting is done, cranioplasty may be attempted with healthy bone graft from ribs as in our case or iliac crest. Split calvarial bone graft is not always possible in infants due to very thin bones and the possibility of infection cannot be ruled out. The use of pedicled pericranial graft spread over the bone defect with rib graft was in order to accelerate healing by providing additional blood supply in addition to from overlying skin and underlying dura. Cranioplasty with bone cement in children is not recommended. Recent trends support the administration of five drugs in the treatment of CTB for a period of 18 months [10]. The role of anticonvulsants is controversial and its use in most cases is avoided.
Conclusion
Calvarial tuberculosis is an uncommon presentation of the common disease. It should be kept as differential diagnosis in a case with skull bone defect from eosinophilic granuloma, tumor, hemangioma, and osteomyelitis even in patients without any history or evidence of extracranial tuberculosis. Scalp swelling with or without discharging sinus is the commonest presentation but may also present as exophytic ulcerated growth on scalp. Surgery and a combination of antituberculous chemotherapy are effective.
References
Barton CJ (1961) Tubercolosis of the vault of the skull. Br J Radiol 34:286–290
Brown TS, Franklyn PP, Marikkar MS (1980) Tuberculosis of the skull vault. Clin Radiol 31:313–315
Gupta PK, Kolluri VR, Chandramouli BA, Venkataramana NK, Das BS (1989) Calvarial tuberculosis: a report of two cases. Neurosurgery 25:830–833
Ip M, Tsui E, Wong KL, Jones B, Pung CF, Ngan H (1993) Disseminated skeletal tuberculosis with skull involvement. Tuber Lung Dis 74:211–214
Jadhav RN, Palande DA (1999) Calvarial tuberculosis. Neurosurgery 45:1345–1350
Koening F (1888) Traite de Pathologie et Chirurgie Speciale. Delahaye Et Lecrosnier, Paris, p 184
Meng CM, Wu YK (1942) Tuberculosis of the flat bones of the vault of the skull. A study of forty cases. J Bone Joint Surg Am 24:341–353
Mohanty S, Rao CJ, Mukherjee KC (1981) Tuberculosis of the skull. Int Surg 66:81–83
Patankar T, Varma R, Krishnan A, Prasad S, Desai K, Castillo M (2000) Radiographic findings in tuberculosis of the calvarium. Neuroradiology 42:518–521
Ramdurg SR, Gupta DK, Suri A, Sharma BS, Mahapatra AK (2010) Calvarial tuberculosis: uncommon manifestation of common disease—a series of 21 cases. Br J Neurosurg 24:572–577
Scoggin CH, Schwarz MI, Dixon BW, Durrance JR (1976) Tuberculosis of the skull. Arch Intern Med 136:1154–1156
Strauss DC (1933) Tuberculosis of the flat bones of vault of the skull. Surg Gynaecol Obstet 57:384–398
Volkman R (1880) Die perforierende Tuberkulose der Knochen das Schaldeldaches. Zentralbl Chir 305–307
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dawar, P., Gupta, D.K., Sharma, B.S. et al. Extensive calvarial tuberculosis presenting as exophytic ulcerated growth on scalp in an infant: an interesting case report with review of literature. Childs Nerv Syst 29, 1215–1218 (2013). https://doi.org/10.1007/s00381-013-2097-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-013-2097-5