
Abstract
Objective
The purpose of this study is to assess the role of endoscopic third ventriculostomy (ETV) in the treatment of hydrocephalus in children under 1 year of age. The authors analyzed data of ETV in their institution.
Methods
Between January 1995 and December 2008, 52 ETV procedures were performed for the treatment of hydrocephalus in 49 infants (32 male and 17 female). Their age ranged from 6 days to just under 12 months (mean age 6.2 months). The cause of hydrocephalus was occlusive in 43 patients (aqueduct stenosis in 31, Chiari II malformation in eight, Dandy–Walker cyst in two, quadrigeminal lipoma in one, and cerebellopontine angle arachnoid cyst in one patient). Communicating hydrocephalus was caused by intraventricular hemorrhage, meningitis, and/or ventriculitis in six patients.
Results
The overall success rate was 69.4% with mean follow-up period of 68.2 months. Patients with aqueduct stenosis had a higher success rate of ETV which was 77.4%. Seven infants were born preterm, six of them required a permanent ventriculoperitoneal shunts (VPS; P = 0.003). Malfunctioned VPS was removed in two patients following ETV. There was one death from intracranial hemorrhage, two cerebrospinal fluid leaks, and one meningitis.
Conclusion
Endoscopic third ventriculostomy can be considered a possible treatment procedure alternative to VPS for the treatment of occlusive hydrocephalus in infants. ETV was effective in full-term infants while the results in low birth weight, preterm infants were poor. Success of ETV is not only age dependent but also etiology dependant. Infants with occlusive hydrocephalus treated with VPS, who present with shunt failure, could be treated by ETV and removal of the shunt device.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The development of neuroendoscopic technique has made the procedure safe and easy, and resulted in a significantly widened range of indications. In hydrocephalus, endoscopic third ventriculostomy (ETV) is being used to restore cerebrospinal fluid (CSF) circulation. However, controversy exists regarding whether children under 1 year of age have a higher risk of failure than older children, increased initial risk of complications, and possible need for a second ETV and/or shunt placement [1–8].
Endoscopic third ventriculostomy has become the procedure of choice for the treatment of occlusive hydrocephalus with reported high success rates mainly for aqueduct stenosis [5, 9, 10]. Lower success rates have been reported for patients with hydrocephalus from other causes, such as postinfection, posthemorrhagic, or myelomeningocele [7, 9, 11, 12].
The aim of this study is to analyze and report our experience with ETV for the treatment of hydrocephalus in 49 infants (under 1 year of age), including overall outcome, rate of postoperative decrease in ventricular size, and associated complications. We investigated the effect of age, weight at birth and at the time of surgery, and the pathogenesis of hydrocephalus on the outcomes.
Patients and methods
Out of 171 neuroendoscopic procedures performed between 1995 and 2008, our study population comprised 49 infants under the age of 1 year who underwent 52 endoscopic procedures for the treatment of hydrocephalus, at King Khalid University Hospital, Riyadh, Saudi Arabia. Data were collected in a retrospective manner from medical charts, pertinent imaging studies (CT and MRI), and operative reports.
Thirty-two patients were male and 17 were female. The mean age was 6.2 months, ranged from 6 days to 11.9 months. Out of the 49 infants, seven were born premature and with low birth weight. Hydrocephalus was occlusive in 43 infants; aqueduct stenosis in 31, Chiari II malformation in eight, Dandy–Walker cyst in two, quadrigeminal lipoma deforming the aqueduct, causing its narrowing in one patient and cerebellopontine angle arachnoid cyst in one patient. In another group of patients; communicating hydrocephalus was attributed to IVH associated with prematurity in three patients, and meningitis was the presumed cause in three patients. Four more infants were born preterm, with low birth weight, and underwent ETV for the treatment of occlusive hydrocephalus (aqueduct stenosis, three; and Chiari II malformation, one; Table 1).
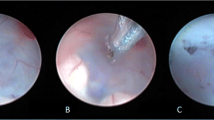
ETV was performed using a rigid pediatric nephroscope (Karl Storz, Tuttlingen, Germany), size 17F. The scope was introduced through the anterior fontanelle or a burr-hole was placed just anterior to the coronal suture in the midpupillary line in patients with small fontanelle. The floor of the third ventricle was punctured using ventriculostomy forceps, and the fenestration was enlarged with a Fogarty catheter. Normal saline at body temperature was used if hemorrhage occurred. The cerebrospinal fluid was then allowed to drain into the basal cistern to the surface of the brain.
All patients included in this study underwent postoperative scans (after 1 week, 1 month, 6 months, and annually) and ventricular size was ascertained using the Evans Index.
Results
A total of 49 infants aged less than 1 year, were studied. Twenty two of them were less than 6 months, and 27 infants aged between 6 and 12 months. Clinical improvement in infants less than 6 months and infants aged 6 months to 1 year was 13 (59%) and 21 (77.8%), respectively. Out of seven premature, low-birth-weight infants, only one has improved, while 33 (78.6%) out of 42 full-term normal birth weight infants showed clinical improvement.
Success of ETV was defined as shunt-free during the period of follow-up which ranged from 6 to 118 months (mean; 68.2 months). Neuroendoscopy was considered failure when there was a subsequent need for redo ETV or shunt implantation, based on clinical and radiological evidence (cranial CT scan) of persistence or progress of hydrocephalus.
The overall success rate of ETV was 69.4%. In patients with obstructive hydrocephalus secondary to aqueduct stenosis, success was 77.4%. Six of the seven preterm infants required a permanent ventriculoperitoneal shunts (VPS; P = 0.003). Malfunctioned VPS was removed in two patients following ETV. Endoscopic exploration and repeat ETV was performed in three infants.
One patient developed pseudomonas meningitis who recovered with proper antibiotic treatment, two patients had temporary CSF leak, which was resolved spontaneously, and one fatal hemorrhagic complication occurred in the youngest patient (6 days). This was due to injury of the premature thin-walled blood vessels while navigating the endoscope through the floor of the third ventricle.
Discussion
The overall clinical success rate in this study was 69.4%. Patients with aqueduct stenosis had the higher success rate of ETV (77.4%). We propose that early failures in infants may result from reduced flow through the stoma, with subsequent closure of the fenestration due to soft skull, and an intracranial pressure that is not high enough to maintain the potency of the fenestration. Other causes have been suggested as high CSF protein causing obliteration of the CSF pathway, and failure of CSF absorption despite a patent stoma [4, 5, 10, 13, 14].
Buxton and his colleagues [2] observed that the presence or absence of flow through the ventriculostomy and the size of the lateral ventricles on postoperative imaging were not an indicator of success or failure. In our cases, ETV was repeated in three patients, after 1, 6, and 10 months from the initial procedure. The reason of failure was found to be second membrane in the first infant and complete closure in the other two patients, confirmed during redo ETV.
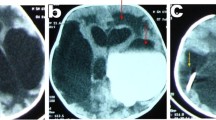
In one infant, obstructive hydrocephalus was caused by quadrigeminal cistern lipoma (Fig. 1a and b). This infant underwent balloon aqueductoplasty, followed by ETV without inserting aqueductal stent. He has been followed up for 7 years, the lipoma marginally increased in size, and although ETV was patent, the ventricles remained large (Fig. 1c and d).

a and b MRI of an infant before surgery showing massively dilated third ventricle due to obstruction of the Aqueduct by a quadrigeminal cistern lipoma. c and d Seven years follow-up MRI scan after endoscopic third ventriculostomy, and aqueductoplasty showing marginal increase in the size of the lipoma, and third ventricle remained dilated.
ETV is not used routinely as the initial treatment for hydrocephalus in patients with Chiari II malformation, as hydrocephalus in those patients has been considered complex and is due to extensive deformity of the posterior fossa and its structures, including small capacity of the posterior fossa, caudal displacement of the fourth ventricle, abnormal disposition of the mid brain and tentorial hiatus, and downward displacement of the cerebellar tonsils through the foramen magnum. This is different from the precipitating mechanism for adult–onset hydrocephalus among patients with Chiari I malformations, which probably involves increasing blockage of CSF flow at the foramen magnum. Although the outcome of third ventriculostomy is expected to be different in both cases, ETV remains an available treatment option of the associated hydrocephalus [15]. We suspected that hydrocephalus was the consequence of obstruction of the outlets of the fourth ventricle in two infants with Chiari II malformation, in whom ETV successfully treated hydrocephalus.
In infants with congenital hydrocephalus associated with posterior fossa cyst, e.g. cerebellopontine angle arachnoid cyst in one patient (Fig. 2a and b) and Dandy–Walker cyst in two patients, ETV proved successful in bypassing the obstruction and treating hydrocephalus (Fig. 2c and d). It has been thought that ETV would be sufficient to decompress the ventricles and the cyst when the aqueduct is patent, and in the presence of aqueductal obstruction, ETV alone may not be enough and must be combined with a procedure draining the posterior fossa cyst [16]. This could be explained by the fact that Dandy–Walker is a complex cystic dilatation of the fourth ventricle, associated with varying extents of vermian hypoplasia and hydrocephalus; while arachnoid cysts arise during development from splitting of arachnoid membrane, and brain volume is actually the same and that it is expected to expand after CSF diversion. However, ETV alone was reported successful in treating obstructive hydrocephalus associated with Dandy–Walker variant in some cases [5, 17, 18].

a Axial MRI, T2-WI showing a large left cerebellopontine angle arachnoid cyst with CSF flowing through it, and causing moderately severe hydrocephalus (b). c and d MRI picture 6 years after ETV showing marginal improvement of the fourth ventricle position, and cyst size remained the same
It has been reported that the use of ETV is safe and effective for the treatment of shunt dysfunction in patients with obstructive hydrocephalus [19, 20]. This can be considered also for infants with shunted hydrocephalus when they present with shunt malfunction. Two of our infants had their obstructed shunts removed after performing successful ETV.
Ventricular size often shows no obvious change following third ventriculostomy, particularly in the early postoperative period, making early postoperative evaluation difficult without expensive and often invasive testing in patients with equivocal clinical responses [12]. The patients underwent CT 1 year after ETV, and we measured the Evans index. Although 64% of the patients showed no or moderate change in ventricular volume as assessed by Evans index, marked reduction in ventricular size was observed in 25% of patients.
Although all our patient populations were younger than 1 year of age and presumably most of them presented with acute rather than chronic hydrocephalus, we found that, there is no statistical significance that age at presentation is related to persistence of postoperative ventricular dilatation (P > 0.05)
None of the patients had a preoperative cognitive function assessment, as all were below 1 year, and only few of them had neuropsychological assessment during their follow-up after ETV.
Hemorrhagic complications resulting from neuroendoscopy for hydrocephalus have seldom been reported. Gaab and Schroeder [21] have previously discussed the methodology that most neurosurgeons perform using neuroendoscopy to control intraoperative bleeding through the endoscope. As the vast majority of hemorrhages encountered during the procedure resolve spontaneously with continued irrigation and occasionally with the bipolar diathermy [22]. In our series, fatal uncontrollable bleeding happened in one patient (2%).
There are recent reports on neuroendoscopy for hydrocephalus in infants showing variable success rates (Table 2). These variations in the results may be related to differences in the patient populations, and the follow-up period, before which ETV will be considered failure. We believe this needs multicenter, prospective, long-term follow-up studies. A prospective randomized, controlled trial of ETV vs shunting in children presenting under the age of 2 years with pure aqueduct stenosis is already running (the International Infant Hydrocephalus Study), hoping to provide answers to unsettled debates on the value of neuroendoscopy for infants [23].
The success rates have been found in the range of 37.5% to 83.7%. However, the overall success rate of the recently published series was found to be 57.3% for 696 infants.
The success rate in our study was not influenced by the age of patients at the time of ETV, the mean age was 4.59 and 4.57 months for both successful and failed cases, respectively, (P > 0.05). On the other hand the success rate was influenced by the underlying pathology and the gestational age of the patients, rather than the age at the time of presentation. One out of seven (14%) premature infants with low birth weight had improved compared with 85.7% improvement in full-term infants with normal birth weight, (P = 0.003).
Koch and Wagner [24] also reported that factors indicating potential failure of ETV were very young age and etiology other than idiopathic aqueduct stenosis, and the probability of success in their opinion seemed to increase during the first 2 or 3 months of life.
Conclusion
Neuroendoscopy can be considered as initial treatment of hydrocephalus, particularly occlusive type, in infants less than 1 year of age. ETV was effective in full-term infants, and carries low morbidity, while the results in low birth weight and preterm infants were poor. However, Success of ETV in this group was affected by gestational age and etiology of the hydrocephalus.
ETV should be considered a valuable alternative to shunt revision in infants affected by obstructive hydrocephalus presenting with shunt malfunction.
References
Beems T, Grotenhuis JA (2002) Is the success rate of endoscopic third ventriculostomy age dependent: an analysis of the results of endoscopic third ventriculostomy in young children. Childs Nerv Syst 18:605–608
Buxton N, Macarthur D, Mallucci C, Punt J, Vloeberghs M (1998) Neuroendoscopic third ventriculostomy in patients less than 1 year old. Pediatr Neurosurg 29:73–76
Cinalli G, Sainte-Rose C, Chumas P, Zerah M, Brunelle F, Lot G, Pierre-Khan A, Renier D (1999) Failure of third ventriculostomy in the treatment of aqueductal stenosis in children. J Neurosurg 90:448–454
Fukuhara T, Vorster SJ, Luciano MG (2000) Risk factors for failure of endoscopic third ventriculostomy for obstructive hydrocephalus. Neurosurgery 46:1100–1111
Hopf N, Grunert P, Fries G, Klaus RK, Perneczky A (1999) Endoscopic third ventriculostomy: outcome analysis of 100 consecutive procedures. Neurosurgery 44:795–804
Mobbs RJ, Vonau M, Davies M (2003) Death after late failure of endoscopic third ventriculostomy: a potential solution. Neurosurgery 53:384–386
Warf BC (2005) Comparison of endoscopic third ventriculostomy alone and combined with choroid plexus cauterization in infants younger than 1 year of age: a prospective study in 550 African children. J Neurosurg 103(6 Suppl):475–481
Baldauf J, Oertel JG, Schroeder MR, Henry WS (2007) Endoscopic third ventriculostomy in children younger than 2 years of age. Childs Nerv Syst 23(6):623–626
Brockmeyer D, Abtin K, Carey L, Walker ML (1998) Endoscopic third ventriculostomy: an outcome analysis. Pediatr Neurosurg 28:236–240
Elbabaa S, Steinmetz M, Ross J, Moon D, Luciano M (2001) Endoscopic third ventriculostomy for obstructive hydrocephalus in the pediatric population: evaluation of outcome. Eur J Pediatr Surg 11(Supp 1):S52–S54
Balthasar AJ, Kort H, Cornips EM, Beuls EA, Weber JW, Vles JS (2007) Analysis of the success and failure of endoscopic third ventriculostomy in infants less than 1 year of age. Childs Nerv Syst 23(2):151–155
Schwartz TH, Ho B, Prestigiacomo CJ, Bruce JN, Feldstein NA, Goodman RR (1999) Ventricular volume following third ventriculostomy. J Neurosurg 91(1):20–25
Jones RF, Kwok BC, Stening WA, Vonau M (1996) Third ventriculostomy for patients with spinal dysraphism: indications and contraindications. Eur J Pediatr Surg 6(Suppl 1):5–6
Siomin V, Cinalli G, Grotenhuis A, Golash A, Oi S, Kothbauer K, Weiner H, Roth J, Beni-Adani L, Pierre-Kahn A, Takahashi Y, Mallucci C, Abbott R, Wisoff J, Constantini S (2002) Endoscopic third ventriculostomy in patients with cerebrospinal fluid infection and/or hemorrhage. J Neurosurg 97:519–524
Teo C, Jones R (1996) Management of hydrocephalus by endoscopic third ventriculostomy in patients with myelomeningocele. Pediatr Neurosurg 25:57–63
Mohanty A (2005) Endoscopic options in the management of isolated fourth ventricles. Case report. J Neurosurg 103(1 Suppl):73–78
Jones RFC, Kwok BCT, Stening WA, Vonau M (1994) The current status of endoscopic third ventriculostomy in the management of non-communicating hydrocephalus. Minim Invasive Neurosurg 37:28–36
Mohanty A, Biswas A, Satish S, Praharaj SS, Sastry KV (2006) Treatment options for Dandy-Walker malformation. J Neurosurg 105(5 Suppl):348–356
Boschert J, Hellwig D, Krauss JK (2003) Endoscopic third ventriculostomy for shunt dysfunction in occlusive hydrocephalus: long-term follow up and review. J Neurosurg 98:1032–1039
Kehler U, Gliemroth J, Knopp U, Arnold H (1998) The role of third ventriculostomy in previously shunted hydrocephalus. In: Hellwig D, Bauer BL (eds) Minimally invasive techniques for neurosurgery. Springer Verlag, Berlin, pp 77–80
Gaab MR, Schroeder HW (1998) Neuroendoscopic approach to intraventricular lesions. J Neurosurg 88:496–505
Schroeder HW, Niendorf WR, Gaab MR (2002) Complications of endoscopic third ventriculostomy. J Neurosurg 96:1032–1040
Sgouros S, Kulkharni AV, Constantini S (2006) The international infant hydrocephalus study: concept and rational. Childs Nerv Syst 22:338–345
Koch D, Wagner W (2004) Endoscopic third ventriculostomy in infants of less than 1 year of age: which factors influence the outcome? Childs Nerv Syst 20(6):405–411
Koch-Wiewrodt D, Wagner W (2006) Success and failure of endoscopic third ventriculostomy in young infants: are there different age distributions? Childs Nerv Syst 22(12):1537–1541
Yadav YR, Sumeet J, Nelson A, Abhijeet B, Gaurav J (2006) Endoscopic third ventriculostomy in infants. Neurolog India 54:161–163
Fritsch MJ, Kienke S, Ankermann T, Padoin M, Mehdorn HM (2005) Endoscopic third ventriculostomy in infants. J Neurosurg 103:50–53
Wagner W, Koch D (2005) Mechanism of failure after endoscopic third ventriculostomy in young infants. J Neurosurg 103:43–49
Gorayeb RP, Cavalheiro S, Zymberg ST (2004) Endoscopic third ventriculostomy in children younger than 1 year of age. J Neurosurg 100:427–429
Fritsch MJ, Mehdorn M (2002) Endoscopic intraventricular surgery for treatment of hydrocephalus and loculated CSF space in children less than one year of age. Pediatr Neurosurg 36(4):183–188
Javadpour M, Mallucci C, Brodbelt A, Golash A, May P (2001) The impact of endoscopic third ventriculostomy on the management of newly diagnosed hydrocephalus in infants. Pediatr Neurosurg 35:131–135
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Elgamal, E.A., El-Dawlatly, AA., Murshid, W.R. et al. Endoscopic third ventriculostomy for hydrocephalus in children younger than 1 year of age. Childs Nerv Syst 27, 111–116 (2011). https://doi.org/10.1007/s00381-010-1254-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-010-1254-3