
Abstract
Introduction
Individuals with neurodevelopmental disorders have been observed to show accelerated cognitive aging or even dementia as early as 30 and 40 years of age. Memory deficits are an important component of age-related cognitive loss.
Methods
In this study, we investigated prospective memory, which is often impaired in aging, in a group of 32 adults with spina bifida meningomyelocele (SBM), including members of the oldest living cohort successfully treated with shunts to divert excess cerebrospinal fluid, ventriculomegaly, and hydrocephalus, who are now around 50 years of age. Seventeen typically developing adults provided a comparison group.
Results
The SBM and comparison groups differed in the prospective memory total score as well as in both time-based and event-based subscores. Prospective memory was impaired in both older and younger individuals with SBM. However, the percentage of individuals with impaired or poor prospective memory was three times higher in the older SBM group than in the younger SBM group. The results are considered in relation to specific features of the complex brain reorganization in SBM.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Spina bifida meningomyelocele (SBM), a neural tube birth defect that is the product of a complex pattern of gene–environment interactions, is associated with distinctive physical, neural, and cognitive phenotypes. Medical and surgical techniques (in particular, management of hydrocephalus with shunt technologies developed in the 1960s [1]) have produced a cohort of individuals with SBM who now range in age from young adulthood to middle age and whose cognitive function is only now being studied (e.g., [2]). Recently, long-term outcome has been explored in studies of young adult spina bifida cohorts, showing that these individuals continue to have difficulties in motor [3, 4], cognitive [5], and academic [6, 7] domains. In this paper, we investigate memory in relation to aging in adults with SBM.
Memory is a key cognitive resource, both for the acquisition of cognitive and academic skills in childhood and for the maintenance of adult cognitive and academic competencies. Reviewing earlier studies (e.g., [8]), Wills [9] concluded that memory was not a characteristic deficit of children with SBM, although later studies suggested specific rather than global memory deficits (e.g., [10, 11]).
The risk of memory problems increases with both normal and pathological aging [12]. Individuals with some neurodevelopmental disorders exhibit early pathological aging and have been observed to show accelerated cognitive aging or even dementia as early as 30 and 40 years of age (e.g., [13]). Adult survivors of SBM with hydrocephalus have poorer memory than adults with occult spina bifida [14]. Dennis et al. [5] investigated different forms of memory in 29 young adults with SBM. While some implicit memory functions were intact, deficits were apparent in working memory (the process of activating and manipulating information in the short term) and episodic memory (the recall and recognition of context specific events). Retrospective memory problems were negatively correlated with communication and community living independence, important components of quality of life.
Individuals with SBM have hydrocephalus, which is treated with shunt diversion. The number of lifetime shunt revisions is a marker for the stability of hydrocephalus. Cognitive outcome is generally unrelated to number of childhood shunt revisions [15–18]; but see [19]. In adults, the number of shunt revisions is negatively related to functional numeracy, independent living, and employment [2, 6, 20]. Less stable hydrocephalus, indexed by a larger number of shunt revisions, is associated with poorer function in some memory domains [5]. Even when apparently controlled, hydrocephalus contributes to poor memory. Although individuals with more shunt revisions had poorer prospective and immediate episodic memory, the young adults with SBM and fewer revisions in Dennis et al. [5] still showed poor memory. Young adults with SBM who have nonfunctioning shunts or non-shunted ventriculomegaly show improved memory after shunt treatment ([21]; although [22] found no relation between memory and magnetic resonance imaging ventricular dilatation, a measure of concurrent hydrocephalus, in a small sample of average-intelligence young adults with hydrocephalus). Thus, some memory deficits may be exacerbated by an increased number of lifetime shunt revisions, a marker for unstable hydrocephalus [5].
Another potential correlate of motor and cognitive deficits is the level of spinal lesion. Individuals with SBM are born with lesions at various levels of the spinal cord, and a higher spinal lesion level is associated with more brain compromise and greater cognitive morbidity in children [23]. In adults with SBM, spinal lesion level affects motor skills such as speech production [4] and motor independence [2], although not cognitive–academic function [2, 6].
Most studies of memory in SBM have concerned retrospective memory, the recall of past events or information. Prospective memory is an important component of everyday adult life because it involves the recall of intentions to be activated in the future. Prospective memory may be event-based (e.g., remembering to deliver a message when you see a particular person), time-based (e.g., remembering to keep an appointment at a specific hour), or activity-based (e.g., remembering to take a pill after dinner) [24]. Prospective memory deteriorates with age [25], but it is not known whether it does so more sharply in individuals with SBM than in typically developing individuals. Dennis et al. [5] found that adults with SBM have poor memory for intentions to be executed in the future. However, these tasks likely involve both prospective and retrospective memory, so the status of prospective memory in SBM remains to be understood.
In this paper, we report on the status of event-based and time-based prospective memory in an adult spina bifida cohort. We hypothesize that adults with SBM will have more prospective memory problems than age-based controls. Prospective memory deteriorates with age [25], but it is not known whether it does so more sharply in individuals with SBM than in typically developing adults. Not all prospective memory tasks deteriorate with aging, however, and older participants perform better than young individuals in naturalistic rather than laboratory tasks of prospective memory [26]. We hypothesize that older adults with SBM will have more prospective memory problems than either age-based controls or younger adults with SBM.
In retrospective memory, the cues for recall or recognition are external; in prospective memory, they are internal. Relative to retrospective memory, prospective memory places demands on internal control mechanisms (“remembering to remember”), and it has been argued that this makes it especially difficult for aging adults [27, 28]. Two entailments of this viewpoint are that the relations between retrospective and prospective memory in the same individuals should be relatively weak (although this issue is complex; [29]) and that external mnemonic support (e.g., taking written notes) should improve prospective memory performance. We hypothesize that a composite measure of retrospective recognition memory will be weakly related to prospective memory performance and also that note taking during the prospective memory task should facilitate performance.
Some data from typically aging individuals suggest that event-based prospective memory is more resilient to aging than time-based prospective memory because time-based prospective memory tasks place increased demands on self-monitoring [30], and time-based prospective memory tasks show the most consistent age-related differences [31]. We hypothesize that individuals with SBM will perform more poorly on time-based Prospective memory tasks than on event-based prospective memory tasks.
Method
Participants
Participants were 32 adults with SBM, including members of the oldest living cohort successfully treated with shunts to divert excess cerebrospinal fluid and control ventriculomegaly and hydrocephalus. The study was approved by the ethics board, and the data were obtained in compliance with institutional regulations for human research at The Hospital for Sick Children in Toronto. Medical information on the SBM participants was obtained from hospital charts or by parent or self report and included age, sex, type and level of spinal lesion, and number of shunt revisions. Table 1 presents IQ and demographic data for each group.
Five participants had an upper spinal lesion (T12 and higher), and 27 had a lower spinal lesion (L1 and lower), according to current taxonomies [23, 32]. Of the 23 shunted participants, five had no shunt revisions, seven had one revision, six had two to four revisions, two had five to nine revisions, and three had ten or more shunt revisions. Two participants had a shunt that was subsequently removed. Seventeen typically developing adults provided a comparison group. Participants ranged in age from 18.33 to 62.67 years old. Each had a Verbal or Performance IQ greater than 70 on the Stanford–Binet Intelligence Scale, fourth edition [33], and no comparison participant had a Verbal IQ greater than 120.
Tests
Prospective memory
The Cambridge Prospective Memory Test (CAMPROMPT) is the first age-normed test of prospective memory [34]. Participants are asked to work on a number of background pencil and paper tasks for a 20-min period. While they are doing these tasks, they are asked to remember to perform other tasks such as reminding the tester of something, either during the 20-min session or shortly thereafter. Participants may use any self-generated strategy as an aid in remembering the tasks.
The CAMPROMPT includes six prospective memory tasks for the participant to carry out in a 25-min period. Three of the tasks are cued by time, and three are cued by events. The time intervals between being asked to do the task and responding appropriately at the right moment are balanced across the two cuing conditions (time and event). Two of the three time-based tasks are cued by a countdown kitchen timer, and the third is cued by a clock. Both the clock and the timer are on the table in front of the participant.
One time-based task is to remind the examiner to make a phone call; the time between the instruction and the required action is 20 min, and the task has to be carried out at a specific time (e.g., 10 past 5, cued by the clock), which is 5 min after the end of the 20-min background task period. Another time-based task is to remind the examiner not to forget his/her keys. Here, the time interval is 13 min, and the response should be made “when there are 7 min left” on the timer. The third time-based task is to change the background task; here, the time interval is 7 min, and the response should be made “in seven minute’s time.”
One of the event-based tasks is cued by a verbal prompt from the examiner, one by the beeper going off followed by a prompt from the examiner, and one by a specific quiz question. One event-based task is to remind the examiner about five objects hidden at the start of the test. The time interval between being asked to carry out the task and the time when the response should be made is 20 min, and the cue is the beep of the timer followed by the examiner saying the test is finished. Another event-based task is to give the examiner a book when there is a quiz question about a specific television program. The time interval between being asked to carry out the task and the time when the response should be made is approximately 8 min, and the cue is the 14th question on a quiz sheet that is handed to the participant 7 min into the test. The third event-based task is to give the examiner a message envelope. The time interval is 13 min, and the cue is the tester saying, “There are 5 min left.”
There is a set pattern of responses to participants’ actions or lack of actions with each task receiving a maximum score of 6. Scores for the three time-based and for the three event-based tasks range from 0–18, yielding a maximum score out of 36 for total prospective memory score.
Retrospective memory
The Rivermead Behavioural Memory Test—Extended Version (RBMT-E; [35]) provides analogs of everyday memory situations (remembering to carry out an everyday task or retaining newly learned information). We used a composite of raw scores from the following subtests.
Picture recognition
Twenty line drawings are shown to participants with instructions to memorize as many as they can in 15 s. Forty pictures are then presented one at a time following a filled delay, and participants have to recognize the 20 original pictures.
Face recognition
Pictures of 15 faces are shown to participants for 3 s each. Thirty faces are then presented one at a time following a filled delay, and participants have to recognize the 15 original faces.
Functional independence
Independent functioning was assessed using the Scales of Independent Behavior—Revised (SIB-R), a structured interview that is normed by age and measures functional independence in four domains: motor, social/communication, personal living, and community living [36]. Parents of participants completed this interview.
Motor skills
This subscale assesses gross-motor and fine-motor skills. Participants or their parents rate how well tasks such as picking up small objects, assembling objects from small parts, and strength and endurance activities are completed without assistance.
Social interaction and communication skills
This subscale assesses social interaction, language comprehension, and language expression skills. Participants or their parents rate how well tasks such as making plans with friends, taking telephone messages, and filling out application forms are completed without assistance.
Personal living skills
This subscale assesses eating and meal preparation, toileting, dressing, personal self-care, and domestic skills. Participants or their parents rate how well tasks such as using bathroom facilities, selecting and maintaining clothing, and home repairs are completed without assistance.
Community living skills
This subscale assesses time and punctuality, knowledge of money and its value, work skills, and home/community orientation. Participants or their parents rate how well tasks such as writing down appointments, paying bills, responding to criticism, and using public transportation are completed without assistance.
Results
Sample characteristics
As expected, the SBM and comparison groups differed on Verbal, t(45) = 2.84, p < 0.01, and Performance IQ, t(47) = 6.65, p < 0.0001 (see Table 1). Note that the Verbal IQ of the group with SBM is within the average range and that the sample with SBM continues to show the lower Performance than Verbal IQ characteristic of this generation when studied as children [37]. Age at testing, socioeconomic status, gender, and ethnicity did not differ significantly between the groups, p > 0.05.
Prospective memory
The SBM and comparison groups differed in total score, t(47) = 4.84, p < 0.0001; time-based subscore, t(47) = 4.28, p < 0.0001; and event-based subscore, t(47) = 3.57, p < 0.001 (see Table 2). The percentage of individuals with impaired or poor prospective memory (based on an individual age-adjusted classification) was 25.00% in the SBM group and 0.00% in the comparison group, and this distribution difference was significant, x 2(1) = 5.08, p < 0.05.
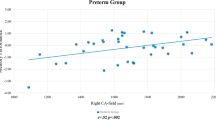
The percentage of individuals with impaired or poor prospective memory was three times higher in the older SBM group (over 32 years; 37.50%) than in the younger SBM group (12.50%) despite being the same in the older and younger comparisons (0.00%). This distribution difference was significant, X 2(3) = 8.74, p < 0.05.
Shunt revision history was available for the 23 shunted participants but was not correlated with total prospective memory score, r(21) = 0.20, p > 0.05.
Within-group t test comparisons were made to establish whether either group showed an advantage for either time-based or event-based memory. Both the SBM and comparison groups demonstrated comparable performance on these subtests, p > 0.05.
Note taking, an option given to all participants, was examined to see if participants using this strategy had a better total prospective score. In the combined sample, notes were found to be beneficial, t(47) = 3.12, p < 0.005, but this result was likely driven largely by the fact that significantly more comparison participants opted to take notes than SBM participants (82.35% versus 50%), X 2(1) = 4.89, p < 0.05. When each group was analyzed separately, note-takers did not demonstrate better prospective memory in either group, p > 0.05.
Relation between prospective and retrospective memory
Correlational analyses were used to determine whether total prospective memory score was related to a retrospective memory composite of face recognition and picture recognition performance from the RBMT-E [35]. These two types of memory were not significantly correlated in either the SBM or comparison groups, p > 0.05.
Relation between prospective memory and functional independence
Correlational analyses were used to determine whether total prospective memory score in the SBM participants was related to any of the four measures of functional independence from the SIB-R [36]. SIB-R scores were available for 43 participants for the social/communication, personal living, and community living domains and for 35 participants for the motor domains (listed in Table 3). The SBM and comparison groups differed significantly on the motor, t(31.3) = 8.17, p < 0.0001; social/communication, t(38.5) = 5.29, p < 0.0001, personal living; t(34.9) = 6.00, p < 0.0001; and community living, t(38.6) = 4.90, p < 0.0001, domains. However, no significant correlations were obtained between prospective memory and any of the functional independence domains for the SBM group, p > 0.05. Similarly, no significant correlations were obtained between prospective memory and any of the functional independence domains in just the older SBM participants, p > 0.05.
Discussion
Young adults with SBM show more prospective memory problems than their age peers. Unlike older typical adults, older adults with SBM have more prospective memory problems than their younger peers. The data support the first two hypotheses and show that level of prospective memory is poorer in individuals with SBM than would be expected on the basis of their chronological age and that their prospective memory declines more sharply with age than that of the comparison group. As individuals with SBM move from young adulthood into middle age, even those with a generally good cognitive outcome are more likely than typically developing age peers to experience prospective memory difficulties and thereby may require social services and social support much earlier in their lives than has been assumed. The social needs of young adults with SBM may include the provision of memory therapies, retraining, or support at an earlier point in life than the age at which independence-limiting disorders of memory would typically emerge.
In adults with SBM, retrospective and prospective memory measures were uncorrelated. This means that functional evaluations of these individuals must include both forms of measures. Theoretically, the data add to the information that retrospective and prospective memories are partially distinct neurocognitive functions: They are factorially separate (e.g., [38]); there is some unique, statistical independent age-related influences on prospective memory not shared by other cognitive abilities [39]; they are differentially affected by age [40]; and they involve partially separate neural processes [41].
Note-taking was overall of benefit to individuals performing prospective memory tasks, as hypothesized, but individuals with SBM were less likely than their age peers to avail themselves of the opportunity to provide themselves with written reminders to carry out tasks in the future. Part of the functional support required by adults with SBM is the provision of external supports for future recall of events and tasks. The fact that adults with SBM used written memory prompts less than the comparison group might suggest that they have a problem in internal control, which is considered to be an origin of problems in time-based prospective memory. However, children with SBM do not have significant problems in internal control [42]. In addition, although we had predicted that time-based prospective memory would be more difficult than event-based prospective memory, neither the SBM nor the comparison group had selective difficulty with time-based prospective tasks, which are assumed to require greater internal control.
Unlike aspects of retrospective memory and the preliminary measures of prospective memory in an earlier study [5], prospective memory in the present study was not related to shunt history. It is possible that this relates to the neuroanatomical stigmata of SBM.
How the neuroanatomical stigmata of SBM are related to memory function is not well understood. The brain in SBM undergoes a complex reorganization (e.g., [43, 44]). Some of this reorganization involves the hippocampi (which are rotated outward and laterally dislocated in a coronal plane, with an elevation of the medial parahippocampal gyri), the mesiotemporal cortex (which has abnormal sulcation), and the key white matter tracts (diffusion tensor imaging tractography shows reduction in white matter tracts such as the uncinate fasciculus that connects inferior frontal and anterior temporal lobes). Animal models of hydrocephalus show macroscopic structural integrity of the hippocampus, but dendritic, axonal, and synaptic alterations suggest deafferentation of dark pyramidal neurons [45]. Furthermore, impairment of spatial memory in kaolin-induced hydrocephalic rats is associated with dysfunction of the hippocampal cholinergic and noradrenergic systems [46]. Prospective memory involving time involves frontal lobe systems (e.g., [29]). The role of the temporal lobes is either secondary [29] or one that involves long delay intervals [47]. Individuals with SBM have atypical development of the frontal lobes involving larger-than-normal volume [48] and thinning of key white matter tracts such as the uncinate fasciculus that connects inferior frontal and anterior temporal lobes [43].
In SBM, it is likely that memory problems, including prospective memory deficits, emerge for a variety of factors related to the key dysmorphologies of SBM as well as to the effects of hydrocephalus on the connectivity of the neural systems supporting memory, an understanding of which is beginning to emerge. An additional research task is to delineate how the brain in individuals with SBM responds to the challenges of normal and abnormal aging.
References
Blum RW, Resnick MD, Nelson R, St. Germaine A (1991) Family and peer issues among adolescents with spina bifida and cerebral palsy. Pediatrics 88:280–285
Hetherington R, Dennis M, Barnes M, Drake J, Gentili F (2006) Functional outcome in young adults with spina bifida and hydrocephalus. Childs Nerv Syst 22:117–124
Dennis M, Salman MS, Jewell D, Hetherington R, Spiegler BJ, MacGregor DL, Drake JM, Humphreys RP, Gentili F (2009) Upper limb motor function in young adults with spina bifida. Childs Nerv Syst 25(11):1147–1153
Huber-Okrainec J, Dennis M, Brettschneider J, Spiegler BJ (2002) Neuromotor speech deficits in children and adults with spina bifida and hydrocephalus. Brain Lang 80:592–602
Dennis M, Jewell D, Drake J, Misakyan T, Spiegler B, Hetherington R, Gentili F, Barnes M (2007) Prospective, declarative, and non-declarative memory in young adults with spina bifida. J Int Neuropsychol Soc 13:312–323
Dennis M, Barnes M (2002) Math and numeracy in young adults with spina bifida and hydrocephalus. Dev Neuropsychol 21:141–155
Barnes MA, Dennis M (2004) Reading and writing skills in young adults with spina bifida and hydrocephalus. J Int Neuropsychol Soc 10:655–663
Parsons JG (1969) Short-term verbal memory in hydrocephalic children. Dev Med Child Neurol Suppl 20:75–77
Wills KE (1993) Neuropsychological functioning in children with spina bifida and/or hydrocephalus. J Clin Child Psychol 22:247–265
Scott MA, Fletcher JM, Brookshire BL, Davidson KC, Landry SH, Bohan TC, Kramer LA, Brandt ME, Francis DJ (1998) Memory functions in children with early hydrocephalus. Neuropsychology 12:578–589
Yeates KO, Enrile BG, Loss N, Blumenstein E, Delis DC (1995) Verbal learning and memory in children with myelomeningocele. J Pediatr Psychol 20:801–815
Cabeza R, Nyberg L, Park D (2005) Cognitive neuroscience of aging: linking cognitive and cerebral aging. Oxford University Press, Oxford
Devenny DA, Krinsky-McHale SJ, Sersen G, Silverman WP (2000) Sequence of cognitive decline in dementia in adults with Down syndrome. J Intellect Disabil Res 44:654–665
Barf HA, Verhoef M, Jennekens-Schinkel A, Post MWM, Gooskens RHJM, Prevo AJH (2003) Cognitive status of young adults with spina bifida. Dev Med Child Neurol 45:813–820
Jensen PB (1987) Psychological aspects of myelomeningocele: a longitudinal study. Scand J Psychol 28:313–321
Raimondi AJ, Soare P (1974) Intellectual development in shunted hydrocephalic children. Am J Dis Child 127:664–671
Ralph K, Moylan P, Canady A, Simmons S (2000) The effects of multiple shunt revisions on neuropsychological functioning and memory. Neurol Res 22:131–136
Tromp CN, van den Burg W, Jansen A, de Vries SJ (1979) Nature and severity of hydrocephalus and its relation to later intellectual function. Z Kinderchir 28:354–360
Halliwell MD, Carr JG, Pearson AM (1980) The intellectual and educational functioning of children with neural tube defects. Z Kinderchir 31:375–381
Hunt GM, Oakeshott P, Kerry S (1999) Link between the CSF shunt and achievement in adults with spina bifida. J Neurol Neurosurg Psychiatry 67:591–595
Mataro M, Poca MA, Sahuquillo J, Cuxart A, Iborra J, de la Calzada MD, Junque C (2000) Cognitive changes after cerebrospinal fluid shunting in young adults with spina bifida and assumed arrested hydrocephalus. J Neurol Neurosurg Psychiatry 68:615–621
Hommet C, Cottier JP, Billard C, Perrier D, Gillet P, De Toffol B, Sirinelli D, Bertrand P, Autret A (2002) MRI morphometric study and correlation with cognitive functions in young adults shunted for congenital hydrocephalus related to spina bifida. Eur Neurol 47:169–174
Fletcher JM, Copeland K, Frederick JA, Blaser SE, Kramer LA, Northrup H, Hannay HJ, Brandt ME, Francis DJ, Villarreal G, Drake JM, Laurent JP, Townsend I, Inwood S, Boudousquie A, Dennis M (2005) Spinal lesion level in spina bifida: a source of neural and cognitive heterogeneity. J Neurosurg 102:268–279
Kvavilashvili L, Ellis J (1996) Varieties of intention: some distinctions and classifications. In: Brandimonte M, Einstein GO, McDaniel MA (eds) Prospective memory: theory and applications. Erlbaum, Mahwah, pp 23–51
Craik FIM, Grady CL (2002) Aging, memory, and frontal lobe functioning. In: Stuss DT, Knight RT (eds) Principles of frontal lobe function. Oxford University Press, New York, pp 528–572
Henry JD, MacLeod MS, Phillips LH, Crawford JR (2004) A meta-analytic review of prospective memory and aging. Psychol Aging 19:27–39
Craik FIM (1986) A functional account of age differences in memory. In: Clix F, Hagendorf H (eds) Human memory and cognitive capabilities: mechanisms and performances. Elsevier, Amsterdam, pp 409–422
McDaniel MA, Einstein GO (2000) Strategic and automatic processes in prospective memory retrieval: a multiprocess framework. Appl Cogn Psychol 14:S127–S144
McFarland CP, Glisky EL (2009) Frontal lobe involvement in a task of time-based prospective memory. Neuropsychologia 47:1660–1669
Harris JE, Wilkins AJ (1982) Remembering to do things: a theoretical framework and an illustrative experiment. Hum Learn 1:123–136
Jäger T, Klugel M (2008) Time-based and event-based prospective memory across adulthood: underlying mechanisms and differential costs on the ongoing task. J Gen Psychol 135:4–22
Park CH, Stewart W, Khoury MJ, Mulinare J (1992) Is there etiologic heterogeneity between upper and lower neural tube defects? Am J Epidemiol 136:1491–1493
Thorndike RL, Hagen EP, Sattler JM (1986) The Stanford–Binet intelligence scale, 4th edn. Riverside, Itasca
Wilson BA, Emslie H, Foley J, Shiel A, Watson P, Hawkins K, Groot Y, Evans JJ (2005) The Cambridge Prospective Memory Test, CAMPROMPT. Harcourt Assessment/The Psychological Corporation, London
Wilson BA, Clare L, Cockburn JM, Baddeley AD, Tate R, Watson P (1999) The Rivermead behavioural memory test (extended version). Thames Valley Test Company Limited, Bury St Edmunds
Bruininks RH, Woodcock RW, Weatherman RF, Hill BK (1996) Scales of independent behavior—revised. The Riverside Publishing Company, Chicago
Dennis M, Fitz CR, Netley CT, Harwood-Nash DCF, Sugar J, Hendrick EG, Hoffman HJ, Humphreys RP (1981) The intelligence of hydrocephalic children. Arch Neurol 38:607–615
Maylor EA, Smith G, Sala SD, Logie RH (2002) Prospective and retrospective memory in normal aging and dementia: An experimental study. Mem Cognit 30:871–884
Salthouse TA, Berish DE, Siedlecki KL (2004) Construct validity and age sensitivity of prospective memory. Mem Cognit 32:1133–1148
Kvavilashvili L, Kornbrot DE, Mash V, Cockburn J, Milne A (2009) Differential effects of age on prospective and retrospective memory tasks in young, young-old, and old-old adults. Memory 17:180–196
West R, Krompinger J (2005) Neural correlates of prospective and retrospective memory. Neuropsychologia 43:418–433
Dennis M, Sinopoli KJ, Fletcher JM, Schacher R (2008) Puppets, robots, critics, and actors within a taxonomy of attention for developmental disorders. J Int Neuropsychol Soc 14:673–690
Hasan KM, Eluvathingal TJ, Kramer LA, Ewing-Cobbs L, Dennis M, Fletcher JM (2008) White matter microstructural abnormalities in children with spina bifida myelomeningocele and hydrocephalus: a diffusion tractography study of the association pathways. J Magn Reson Imaging 27:700–709
Miller E, Widjaja E, Blaser S, Dennis M, Raybaud C (2008) The old and the new: supratentorial MR findings in Chiari II malformation. Childs Nerv Syst 24:563–575
Kriebel RM, McAllister JP Jr (2000) Pathology of the hippocampus in experimental feline infantile hydrocephalus. Neurol Res 22:29–36
Egawa T, Mishima K, Egashira N, Fukuzawa M, Abe K, Yae T, Iwasaki K, Fujiwara M (2002) Impairment of spatial memory in kaolin-induced hydrocephalic rats is associated with changes in the hippocampal cholinergic and noradrenergic contents. Behav Brain Res 129:31–39
Adda CC, Castro LHM, Além-Mar e Silva LC, de Manreza MLG, Kashiara R (2008) Prospective memory and mesial temporal epilepsy associated with hippocampal sclerosis. Neuropsychologia 46:1954–1964
Juranek J, Fletcher JM, Hasan KM, Breier JI, Cirino PT, Alvarez PP, Diaz JD, Ewing-Cobbs L, Dennis M, Papanicolaou AC (2008) Neocortical reorganization in spina bifida. Neuroimage 40:1516–1522
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by National Institute of Child Health and Neurological Development Program Project Grants 1998–2010 P01 HD35946 P01 HD35946-06 “Spina Bifida: Cognitive and Neurobiological Variability.”
Rights and permissions
About this article
Cite this article
Dennis, M., Nelson, R., Jewell, D. et al. Prospective memory in adults with spina bifida. Childs Nerv Syst 26, 1749–1755 (2010). https://doi.org/10.1007/s00381-010-1140-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-010-1140-z