
Abstract
Objective
The objective of the study was to measure upper limb motor function in young adults with spina bifida meningomyelocele (SBM) and typically developing age peers.
Method
Participants were 26 young adults with SBM, with a Verbal or Performance IQ score of at least 70 on the Wechsler scales, and 27 age- and gender-matched controls. Four upper limb motor function tasks were performed under four different visual and cognitive challenge conditions. Motor independence was assessed by questionnaire.
Results
Fewer SBM than control participants obtained perfect posture and rebound scores. The SBM group performed less accurately and was more disrupted by cognitive challenge than controls on limb dysmetria tasks. The SBM group was slower than controls on the diadochokinesis task. Adaptive motor independence was related to one upper limb motor task, arm posture, and upper rather than lower spinal lesions were associated with less motor independence.
Conclusions
Young adults with SBM have significant limitations in upper limb function and are more disrupted by some challenges while performing upper limb motor tasks. Within the group of young adults with SBM, upper spinal lesions compromise motor independence more than lower spinal lesions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Spina bifida is a neural tube defect, one of a group of congenital disorders, that results from failure of the neural tube to close at the expected time, around 3–4 weeks of gestation. Its birth prevalence is about one per 1,000 live births in the USA and one per 750 live births in Canada [10]. Spina bifida meningomyelocele (SBM), the most common and most severe form of spina bifida, is associated with disruption of the upper and/or lower motor and sensory pathways [3, 5]. In addition, brain dysmorphologies are common, and the cerebellum, the midbrain and brainstem, the posterior cortex, and the corpus callosum are dysmorphic or dysplastic in individuals with SBM [3, 8, 10]. Some 90% of affected individuals with spina bifida develop hydrocephalus, often in association with the Chiari type II malformation, in which the cerebellar tonsils herniate down the vertebral column through the foramen magnum.
Neurodevelopmental disorders such as SBM are typically studied in infancy or childhood, although the natural history of SBM has changed over the last three decades [18]. With advances in neurosurgical treatments for the primary spinal lesion and for shunt management of the associated hydrocephalus, increasing numbers of individuals with SBM are reaching adulthood. These new young adults represent the first generation of individuals with SBM and modern-era shunt treatment to reach adulthood. Little is known about their physical or neuropsychological function.
Impaired motor function has long been identified in children with SBM, including those with hydrocephalus. Upper limb neurological abnormalities include spasticity and/or cerebellar signs present either uni- or bilaterally [24, 33]. The physical impairments in SBM include motor and sensory deficits of the lower limbs leading to difficulties with stance and locomotion, as well as urinary and bowel dysfunction causing wheelchair dependence [37]. A variety of cognitive impairments in perception and cognitive development have also been documented (reviewed in [10]).
Upper limb function, as well as lower limb function, is impaired in some two thirds of children with SBM. Upper limb motor deficits in SBM include motor weakness, hand and finger dexterity, motor speed, motor planning, and bimanual coordination [1, 11–14, 16, 17, 22, 27, 30, 32, 34, 39]. Children with SBM have an increased prevalence of left handedness [19, 38]. Upper limb motor deficits are demonstrable on neuropsychological tests of motor function and eye–hand coordination, as well as on everyday tasks involving drawing and handwriting.
Poor upper limb function has been related to a variety of primary or secondary effects of spina bifida (SB) or its treatment, which may act separately or conjointly. These include cortical, brainstem, cerebellar, and corpus callosum dysmorphologies; seizures; active hydrocephalus; shunt history, including revisions and infections; lowered intelligence; visual impairments; lack of experience-dependent motor and visuo-motor development; primary spinal cord malformations causing weakness, spasticity, or incoordination of the upper limbs; level of spinal cord lesion; lack of trunk control; and scoliosis [2, 11, 12, 15, 17, 20, 22, 23, 25, 27–30, 32, 33, 37, 39].
This paper is concerned with upper limb function in a cohort of young adults with SBM compared to typically developing age peers. The reasons for studying upper limb function in SBM adults are: (1) There is almost no information about upper limb status in SBM adults; (2) there is no information about ecological motor function in SBM, that is, the ability to perform upper limb tasks under conditions of routine challenge; (3) within SBM cohorts, there is no information about whether medical history variables (e.g., number of shunt revisions) and/or physical phenotypes that correspond to genetic differences (e.g., spinal cord lesion level) moderate the level of upper limb function; and (4) there is no information about whether upper limb motor function is related to adult quality of life and physical independence.
Knowledge about upper limb motor function in individuals with SBM has been largely based on studies of children [13], although some studies on upper limb motor function in subjects with SBM have included a few young adults [16, 24]. There are no quantitative studies of upper limb motor function in SBM adults. The first specific aim was to compare performance on three upper limb tasks (posture and rebound of outstretched arms, limb dysmetria/dystaxia or finger–nose–finger coordination, and rapidly alternating hand movement or diadochokinesis) in young adults with SB and age-matched controls.
Studies of motor function in SBM children have not addressed ecological capacity, the ability to instantiate motor skills under conditions of routine challenge (e.g., to carry out a motor task while simultaneously performing an unrelated cognitive task or with environmental distraction). There is no information about how individuals with SB perform upper limb motor task under conditions of physical or cognitive challenge. The second specific aim was to compare performance on upper limb tasks under different challenge conditions concerned with visual guidance (eyes open vs. eyes closed) or cognitive load (silence vs. counting backward) in the SBM and control groups.
Medical history variables such as those related to medical complications or shunt function may moderate the effects of motor function in young adults with SBM, although this has not been studied. The embryological and genetic basis of two physical phenotypes in SBM, upper vs. lower spinal cord lesions, has recently been reported [35, 36], but whether motor function varies with physical phenotype in adults with SBM is unknown. The third specific aim was to consider variability within the SBM group as a function of medical complications, shunt revisions (which we consider to be a marker for severity of hydrocephalus), and spinal lesion level.
Young adults with SBM have documented problems with physical and social independence (e.g., [26]). The fourth specific aim was to relate upper limb motor function to perceived motor independence within the SBM group.
Methods
Participants
In this retrospective case–control study, the participants were 26 young adults with SBM, each having a Verbal or Performance IQ score of at least 70 on the Wechsler scales. All SB participants had been treated for hydrocephalus by diversionary shunts. Modern neuroimaging studies were not available. Almost all cases of myelomeningocele with hydrocephalus are associated with the Chiari type II malformation; the fact that our SBM participants required early shunt treatment for hydrocephalus indicates that they had the brain stigmata of the Chiari type II malformation. In terms of mobility status, 17 SBM participants were non-ambulatory, four required assistive devices such as crutches, and five walked independently. The controls were 27 young healthy adults of normal intelligence, matched for age and gender to the SB group. Table 1 presents IQ and demographic data for each group.
Medical information on SBM participants was obtained by reviewing hospital charts or by direct inquiry. Information gathered included age, sex, handedness, type and level of spinal lesion, age at shunt insertion, shunt history, and shunt infections.
Medical histories coded over a 30-year period are of necessity incomplete; nevertheless, the total number of medical complications (including episodes of coma, seizures, visual problems such as strabismus, refractive errors and abducens nerve palsy, and orthopedic conditions such as scoliosis) provides a marker for the overall complexity of medical problems from birth to the time of testing in adulthood. Medical complications were present in 16 SBM participants: Nine had previous seizures, and four had not had seizures (seizure status was not reported in the other 13). Visual abnormalities (including sixth nerve palsy, refractive errors, and strabismus) were present in 12 participants, absent in three, and unknown in 11. Other medical complications included scoliosis in four patients, kyphosis in one, arthritis in one, coma after shunt revision in one, and chronic subdural haematoma in one.
The number of shunt revisions was established by direct questioning of participants or parents. For analysis, two shunt revision groups were created (on the basis of an empirical group division, not on an a priori basis): 14 participants who had zero to three revisions and 12 participants with four or more revisions. Of 17 SB participants who could answer the question about shunt infections, 14 reported no infection, and three participants reported more than one infection.
From birth records and medical charts, two spinal lesion level groups were created, one (N = 6) with upper lesions (T12 and above) and one (N = 20) with lower lesions (L1 and below). One participant’s record noted only an upper lumbar spinal lesion, on the basis of which she was assigned to the lower spinal lesion group.
Tests
Upper limb motor performance was analyzed from videotapes of a motor examination. Each motor test was conducted under four different visual and cognitive challenge conditions. The four conditions were eyes open without counting, eyes closed without counting, eyes open and counting backward from 50, and eyes closed and counting backward from 50. Motor tasks were scored from the videotaped examination. Time to perform tasks was recorded by the examiner at the time of the tests and checked from the videotape.
Posture test
Participants were asked to stand or sit next to a wall mapped with 15-cm grids while holding their arms outstretched and parallel, with the palms of the hand facing down for 30 s (full score) or until the hands dropped more than one grid. The score was graded as a function of the time taken to perform the task correctly, and the total posture score was the sum over the four challenge conditions.
Rebound test
Participants were given a tap just above the wrist, at 30° angle to their outstretched, still, and parallel arms, so that the tap just displaced the arm. The task was performed twice under each of the four challenge conditions mentioned above. The score was graded according to the quality of arm return, tone, presence of rebound, and overshooting. The total rebound score was the sum of the four challenge conditions.
Limb dysmetria/dystaxia test
This is a standardized finger–nose–finger test [21]. Participants held one arm straight out with the index finger at right angle to the arm. Using the index finger of the other hand, they touched the tip of the nose and then touched the tip of the other extended finger. The sequence was repeated ten times with each hand. The dysmetria/dystaxia task was timed and scored separately under the four challenge conditions. Accuracy and time to complete the iterations were the response measures.
Diadochokinesis
In this rapidly alternating hand movements test, participants placed one hand palm open and down, on a table and turned it over fully. Ten iterations were performed, smoothly and evenly for each hand. The task was timed and scored separately under the four challenge conditions. Accuracy and time to complete the iterations were the response measures.
Adaptive motor function
Adaptive motor function was measured using the motor subtest of the Scales of Independent Behavior, a structured interview format assessment for measuring functional independence in motor development, social development, language, self-help, and community adaptation [4]. The tests are individually administered through a structured interview, and norms are provided according to age. The motor subtest surveys independence in tasks that require gross and fine motor skills. The score was age-based for the motor scale.
Relations among medical and demographic variables and outcome variables were examined initially as correlations. Group differences were examined in two ways: Cross-tabulation analysis was used with the chi-square test of significance where restricted ranges of scores did not permit parametric analysis. For the other outcome measures, repeated-measures analysis of variance was employed to test for interactions and main effects of test condition.
Results
Intelligence
The groups differed on Full Scale IQ (F(1,51) = 27.77, p < 0.0001), Verbal IQ (F(1,51) = 5.56, p < 0.05), and Performance IQ (F(1,51) = 56.72, p < 0.0001). The control group IQ scores clustered around the population mean of 100 (see Table 1). For the SBM group, there was no association between IQ scores and medical complications or adaptive motor independence score. There also was no difference in IQ as a function of lesion level group; however, participants with more shunt revisions had a lower Performance IQ (F(1,24) = 4.60, p < 0.05).
Arm posture and rebound
Nearly all control subjects obtained perfect scores on these tests so scores were collapsed over the challenge conditions. Nineteen SBM participants were unable to perform one or both of these tasks, either because of deficits in motor skill or poor truncal control; the remaining participants approached or were at the test ceiling except for one participant who scored in the midrange for rebound. Overall, there was a significant group difference, such that fewer SBM than control participants obtained perfect scores (posture: χ 2(1) = 28.31, p < 0.0001, rebound: χ 2(1) = 20.54, p < 0.0001). Posture and rebound scores in the SBM group were unrelated to age at test and medical complications and did not differ by shunt revision or spinal lesion level group.
Finger–nose–finger test
The SBM group performed less accurately than the control group (F(1,50) = 14.46, p < 0.0005, Table 2).
The challenge of closing the eyes caused a decrement in accuracy for both groups (F(1,50) = 64.85, p < 0.0001). Counting backward affected accuracy more in the SBM than in the control group (F(1,50) = 4.81, p < 0.05). The two groups took equivalent time to perform the finger–nose–finger test. Closing the eyes increased the time taken in both groups (F(1,50) = 27.12, p < 0.0001). Counting backward did not affect time to perform the task, either with eyes open or eyes closed. Within the SBM group, performance accuracy and time scores were unrelated to age at test and medical complications and did not differ by shunt revision or spinal lesion level group.
Diadochokinesis test
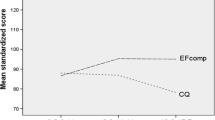
On the diadochokinesis test, the SBM group scored more poorly than controls (F(1,51) = 28.44, p < 0.0001, Table 2). Closing the eyes had no effect on performance. Counting backward caused a decrement in performance for both groups (F(1,51) = 6.35, p < 0.05), although counting backward with eyes closed did not result in a further performance decrement. Time scores differed in the two groups (F(1,51) = 19.59, p < 0.0001). Closing the eyes did not affect time scores. However, time to perform the task increased in both groups with counting backward (F(1,51) = 25.70, p < 0.0001). Counting backward with eyes closed increased time to perform the task for both groups (F(1,51) = 5.02, p < 0.05). Within the SBM group, accuracy and time scores for diadochokinesis were unrelated to age at test and medical complications and did not differ by shunt revision or spinal lesion level group.
Scales of independent behavior
Scores were available on 21 participants with SBM. The motor score was more than two standard deviations below the mean for age in 15 subjects (71%). The only association between perceived motor independence and upper limb motor function tasks (whether accuracy or time scores were considered) was a positive correlation between arm posture and motor independence (r(19) = 0.76, p < 0.0001). Motor independence scores were unrelated to age at test and medical complications and did not differ by shunt revision group. However, the difference between lesion level groups was significant, F(1,19) = 11.94, p < 0.005. Participants with higher spinal lesions had lower levels of motor independence.
Discussion
Young adults with SBM and hydrocephalus have impaired upper limb function relative to age- and gender-matched peers on tasks of arm posture and rebound, finger–nose–finger, and rapidly alternating hand movements. The presence of upper limb motor deficits in young SBM adults (albeit in a cross-sectional rather than longitudinal study) shows that the upper limb function deficits observed in SBM children persist into adulthood and do not resolve with increasing age.
For some tasks, young SBM adults and their age peers responded similarly to motor challenge. For example, both showed a decrement in accuracy and/or speed of response on the finger–nose–finger and diadochokinesis tasks when required to complete a concurrent physical or cognitive task. For the finger–nose–finger task, performance was influenced in both groups by the physical demands of closing the eyes.
For one upper limb task, motor challenge was more disruptive for the young SBM adults than for their age peers. The finger–nose–finger task during backward counting was especially difficult for the SBM group. For young adults with SB, certain motor functions can be performed when there are no distractions or dual task requirements, but deteriorate under the conditions of multitasking that mimic the real world instantiation of these skills.
Motor function was not obviously related to medical history variables. Shunt revisions in childhood are generally unrelated to intellectual outcome [9] or to a range of more specific neuropsychological tasks. In adulthood, by contrast, a greater number of lifetime shunt revisions is associated with compromised non-verbal intelligence but not motor task performance. The impact on cognitive development of repetitive shunt revisions may be underestimated if measured in childhood, so that cognitive outcome measures administered in adulthood may be more valid measures of the effects of shunt revisions, although upper limb motor function does not appear related to shunt history.
Spinal cord lesion level was unrelated to upper limb motor tasks in young adults with SBM; however, upper rather than lower lesions were associated with more limited motor independence, and arm posture was related to motor independence. In childhood, spinal lesion level is related to cognitive tasks [9], whereas in adulthood, spinal lesion level may be related to quality of life measures, such as perceived motor independence. Spinal lesion level is a phenotypic marker of two distinct SBM genotypes [36]; we show here that this genotype–phenotype distinction may have consequences for adult quality of life.
Young adulthood in individuals with SBM brings increased psychosocial demands [26], as well as increased need for psychosocial and occupational services [6, 31]. Part of providing these services is identifying those individuals with greater or lesser need. More research is required to assess the functional impact of these deficits on handwriting, fine motor skills, motor learning [7], and activities of daily living, so that habilitation programs may be developed to enhance the quality of life of this first cohort of adults with SBM and the cohorts to follow.
References
Anderson E, Plewis I (1977) Impairment of a motor skill in children with spina bifida cystica and hydrocephalus: an exploratory study. Br J Psychol 68:61–70
Aronin PA, Kerrick R (1995) Value of dynamometry in assessing upper extremity function in children with myelomeningocele. Pediatr Neurosurg 23:7–13
Barkovich AJ (1995) Pediatric neuroimaging, 2nd edn. Raven, New York
Bruininks RH, Woodcock RW, Weatherman RF, Hill BK (1997) Scales of independent behavior—revised. Riverside, Itasca
Brunt D (1980) Characteristics of upper limb movements in a sample of meningomyelocele children. Percept Mot Skills 51:431–437
Castree BJ, Walker JH (1981) The young adult with spina bifida. Br Med J 283:1040–1042
Cordo PJ, Bell CC, Horral S (1977) Motor learning and synaptic plasticity in the cerebellum. Cambridge University Press, Cambridge
Dennis M, Barnes MA, Hetherington CR (1999) Congenital hydrocephalus as a model of neurodevelopmental disorder. In: Tager-Flusberg H (ed) Neurodevelopmental disorders. MIT, Cambridge, pp 505–532
Dennis M, Fitz CR, Netley CT, Sugar J, Harwood-Nash DCF, Hendrick BE, Hoffman HJ, Humphreys RP (1981) The intelligence of hydrocephalic children. Arch Neurol 38:607–615
Fletcher JM, Dennis M, Northrup H (2000) Hydrocephalus. In: Yeates KO, Ris MD, Taylor HG (eds) Pediatric neuropsychology: research, theory, and practice. Guilford, New York, pp 25–46
Grimm RA (1976) Hand function and tactile perception in a sample of children with myelomeningocele. Am J Occup Ther 30(4):234–240
Hamilton AM, Shah SK (1984) Physical hand function of the child with spina bifida myelomeningocele. Br J Occup Ther, May issue, pp 147–150
Hetherington R, Dennis M (1999) Motor function profile in children with early onset hydrocephalus. Dev Neuropsychol 15(1):25–51
Holler KA, Fennell EB, Crosson B, Boggs SR, Mickle JP (1995) Neuropsychological and adaptive functioning in younger versus older children shunted for early hydrocephalus. Child Neuropsychology 1(1):63–73
Hurley AD, Laatsch LK, Dorman C (1983) Comparison of spina bifida, hydrocephalic patients and matched controls on neuropsychological tests. Z Kinderchir 38(Supp II):116–118
Jacobs RA, Wolfe G, Rasmuson M (1988) Upper extremity dysfunction in children with myelomeningocele. Z Kinderchir 43(Supp II):19–21
Jansen J, Taudorf K, Pedersen H, Jensen K, Seitzberg A, Smith T (1991) Upper extremity function in spina bifida. Childs Nerv Syst 7:67–71
Laurence KM, Tew BJ (1971) Natural history of spina bifida cystica and cranium bifidum cysticum. Arch Dis Child 46:127–138
Lonton AP (1976) Hand preference in children with myelomeningocele and hydrocephalus. Dev Med Child Neurol 18(Supp 37):143–149
Lonton AP (1977) Location of the myelomeningocele and its relationship to subsequent physical and intellectual abilities in children with myelomeningocele associated with hydrocephalus. Z Kinderchir 22(4):510–519
McCarron LT (1976) Mand McCarron assessment of neuromuscular development: fine and gross motor abilities. Common Market, Dallas
Mazur JM, Aylward GP, Colliver J, Stacey J, Menelaus M (1988) Impaired mental capabilities and hand function in myelomeningocele patients. Z Kinderchir 43(Supp II):24–27
Mazur JM, Menelaus MBM, Hudson I, Stillwell A (1986) Hand function in patients with spina bifida cystica. J Pediatr Orthop 6:442–447
Mazur JM, Stillwell A, Menelaus M (1986) The significance of spasticity in the upper and lower limbs in myelomeningocele. J Bone Joint Surg 68-B(2):213–217
Minns RA, Sobkowiak CA, Skardoutsou A, Dick K, Elton RA, Brown JK, Forfar JO (1977) Upper limb function in spina bifida. Z Kinderchir 22(4):493–506
Morgan DJR, Blackburn MC, Bax MCO (1993) A new clinic for young adults with spina bifida and/or hydrocephalus age 16–25 years. Eur J Pediatr Surg 3:23–24
Muen WJ, Bannister CM (1997) Hand function in subjects with spina bifida. Eur J Pediatr Surg 7(Supp I):18–22
Parsons J (1972) Assessments of aptitudes in young people of school-leaving age handicapped by hydrocephalus or spina bifida cystica. Dev Med Child Neurol 14(Supp 27):101–108
Pearson AM, Carr J, Hallwell MD (1988) The handwriting of children with spina bifida. Z Kinderchir 43(Supp II):40–42
Sand PL, Taylor N, Hill M, Kosky N, Rawlings M (1974) Hand function in children with myelomeningocele. Am J Occup Ther 28(2):87–90
Stellman-Ward G, Bannister CM, Lewis M (1993) Assessing the needs of the adults with spina bifida. Eur J Pediatr Surg 3:14–16
Turner A (1985) Hand function in children with myelomeningocele. J Bone Joint Surg 67-B(2):268–272
Turner A (1986) Upper-limb function of children with myelomeningocele. Dev Med Child Neurol 28:790–798
Tew BJ (1988) Spina bifida children in ordinary schools: handicap, attainment and behaviour. Z Kinderchir 43(Supp II):46–48
Van Allen MI, Kalousek DK, Chernoff GF, Juriloff D, Harris M, McGillivray BC, Yong S-L, Langlois S, MacLeod PM, Chitayat D, Friedman JM, Wilson RD, McFadden D, Pantzar J, Ritchie S, Hall JG (1993) Evidence for multi-site closure of the neural tube in humans. Am J Med Genet 47:723–743
Volcik KA, Blanton SH, Tyerman GH, Jong ST, Rott EJ, Page TZ, Romaine NK, Northrup H (2000) Methylenetetrahydrofolate reductase and spina bifida: evaluation of level of defect and maternal genotypic risk in Hispanics. Am J Med Genet 95:21–27
Wallace SJ (1973) The effect of upper-limb function on mobility of children with myelomeningocele. Dev Med Child Neurol 15(Supp 29):84–91
Wassing HE, Siebelink BM, Luyendijk W (1993) Handedness and progressive hydrocephalus in spina bifida patients. Dev Med Child Neurol 35:788–797
Wasson CMA, Bannister CM, Ward Stellman G (1992) Factors affecting the school placement of children with spina bifida. Eur J Pediatr Surg 2(Supp I):29–34
Acknowledgment
Supported by a project grant from the Ontario Mental Health Foundation and by National Institute of Child Health and Human Development Grant P01 HD35946 “Spina Bifida: Cognitive and Neurobiological Variability”. We thank Joanne Robitaille, Caitlin Mahy, Talar Hopyan, Bravina Bala, Joanne D’ Mello, Tali Bogler, and Rebekah Nelson for assistance with data collection and scoring.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dennis, M., Salman, M.S., Jewell, D. et al. Upper limb motor function in young adults with spina bifida and hydrocephalus. Childs Nerv Syst 25, 1447–1453 (2009). https://doi.org/10.1007/s00381-009-0948-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-009-0948-x