
Abstract
Purpose
To compare the practical difficulties of external and internal craniofacial distraction devices used in craniofacial advancement in terms of technical surgical limitations and patients’ discomfort.
Materials and methods
This study involved analysis of the pertinent literature and personal experience on the treatment of patients affected with syndromic craniosynostoses treated with craniofacial distraction advancement.
Results
One hundred patients who underwent internal craniofacial distraction were analyzed. This kind of distraction device was found to be adequately tolerated by the patients with regards to physical and psychological aspects. They had relatively little impact on day-life activities. However, a significant drawback of this type of device is represented by the difficulty in controlling the vectors of distraction. Thirty-eight patients were analyzed after having received the implantation of an external craniofacial distraction device. This type of instrumentation was found to have a significant psychological impact and important limitation on recreational activities. External devices, however, offered important advantages in the control of the vectors of distraction, which could be modified according to the patient’s needs during the perioperative and early postoperative clinical course. There were no significant differences among the two types of devices with regard to osteogenesis and degree of facial advancement.
Conclusion
Both internal and external devices are effective in distraction craniofacial advancement. However, significant differences do exist concerning the surgical aspects and the practical difficulties experienced by the patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The first demonstration of the possibility of advancing the frontal cranial area and the orbital district simultaneously without functional complications was provided by Tessier et al. [18] in 1967. Several authors have since contributed to the development of craniofacial surgery including Marchac et al. [10], Converse et al. [7], McCarthy et al. [11], and Ortiz-Monasterio et al. [15]. Nevertheless, standard craniofacial advancement had technical limitations, mainly the need of donor sites to obtain bone grafts to stabilize the advancement obtained, as well as a very high risk of cerebrospinal fluid (CSF) fistulas with subsequent liquorrhea and in some cases lepto-meningitis. Early in the 1990s, attempts were made to resolve these problems by applying distraction osteogenesis to the craniofacial district after its surgical mobilization. Distraction osteogenesis was actually described for the first time by Codivilla in 1905, subsequently revisited and popularized in the Western world by Bianchi-Maiocchi in the 1980s [2]. Distraction osteogenesis was then applied for the first time in the maxillofacial district in 1992 by McCarthy et al. [12], who reported the elongation of the mandible of patients affected by hemifacial microsomia and Nager syndrome.
The first report in the literature regarding the clinical use of an internal craniofacial distraction device was published by Chin and Toth [5] in 1996. In 1997, the use of an external distraction device was reported by Polley and Figueroa [16].
In the last 10 years, distraction osteogenesis has been utilized in almost all craniofacial centers because of its advantages compared with previous osteotomic techniques. These advantages include shorter time of surgical procedures, minor intraoperative bleeding and lower rate of complications, the absence of postsurgical bone gaps and the lack of needing bone grafts, the gradual expansion of the frontal lobes in the absence of an empty space, higher compliance of soft tissues, and the ability to achieve a better surgical correction.
With regards to bone distractors for craniofacial advancement, opinions in literature differ with authors who find internal devices to be superior, whereas others do rely on rigid external devices, exclusively.
The aim of this paper is to compare the two systems in terms of surgical implantation and results as well as of the quality of the patient’s life during the distraction period.
Materials and methods
A survey of the literature from 2000 to 2006 on the application of distraction osteogenesis in craniofacial advancement, provided by a PUBMED search (National Library of Medicine, NCBI, New Pubmed System; revised April 3, 2000), was performed by applying the following key words: craniofacial distraction, frontorbital, fronto-orbital, fronto orbital, and monobloc.
The initial search revealed the following:
-
236 works for the term craniofacial distraction
-
40 for frontorbital
-
281 for fronto-orbital
-
410 for fronto orbital
-
160 for monobloc
For the analysis of this sample of papers, excluding those that appeared more than once based on the terms of search, the following selection criteria were used: (1) description of the surgical cases; (2) use of a surgical technique, which required access to the anterior cranial fossa and detachment of the dura; (3) inclusion in each study of at least four patients; and (4) description of the kind of distractors utilized and any complications encountered.
With these criteria, the authors selected 11 papers [1, 2, 4, 6, 8, 9, 13, 14, 17, 19, 20], which responded to the selection criteria. In particular, considered for the study were patients treated with a distraction protocol consisting of internal craniofacial distraction devices (ICDD) or external craniofacial distraction devices (ECDD). For each surgical experience, the kind and the number of distractor used, age of patients, pathological substratum, and the extent of craniofacial advancement were analyzed.
Moreover, to fulfill the aim of this study, surgical management, the number and types of complications, the surgical difficulties in installing and removing the distractor, and the ability to control the distraction vector were also taken into consideration.
To assess the impact of the surgical protocol on the quality of the patients’ life, the criteria reported by Primrose in 2005 were applied:
-
Pain
-
Speech problems
-
Feeding problems
-
Difficulty to achieve adequate oral hygiene
-
Alterations in sensitivity
-
Sleeping problems
-
Disturbance of recreational activities
-
Psychological impact
We compared data in the literature with our own experience based on eight patients selected from a personal series of 242 cases of craniofacial surgical procedures. The selection criteria for these eight patients were the same as the ones used for the literature review (Tables 1 and 2).
Results
ICDD group
Concerning the ICDD group, 100 patients were selected (96 patients from the literature review and 4 cases of our series). Of the 96 patients selected from the literature, 20 were affected by Crouzon syndrome, 12 by Apert syndrome, 7 by Pfeiffer syndrome, and 57 by other nonsyndromic craniofacial pathological conditions [1, 2, 6, 13, 14, 19, 20].
The age ranged between 4 months and 15 years with a mean of 5.3 years.
The craniofacial advancement varied from 7 to 27.5 mm with a mean of 17.2 mm.
Three of the four patients in our series were affected by Crouzon syndrome (Fig. 1) and one was affected by Pfeiffer II syndrome. Ages in this subgroup ranged between 4 and 8 years with a mean of 5.4 years. The craniofacial advancement varied from 12 to 20 mm with a mean of 15.1 mm (Table 1).

ICDD group. Four-year-old female. Crouzon syndrome. Lateral view before (a) and after (b) the craniofacial distraction advancement
ECDD group
Concerning the ECDD group, we selected 38 patients (34 from the literature and 4 from our own series). Of the 34 patients of the literature, 15 were affected by Crouzon syndrome, 8 by Apert syndrome, 7 by Pfeiffer syndrome, and 4 by other craniofacial pathological conditions [1, 4, 8, 9].
Patients’ age ranged from 2 to 43 years with a mean of 8.2 years.
The craniofacial advancement varied from 13 to 26 mm with a mean of 16.2 mm.
Two of our four patients in our series were affected by Crouzon syndrome (Fig. 2) and two by Pfeiffer II syndrome. The ages ranged between 8 and 16 years with a mean of 14.1 years.

ECDD group. Sixteen-year-old female. Crouzon syndrome. Lateral view before (a) and after (b) the craniofacial distraction advancement
The craniofacial advancement varied from 12 to 35 mm with a mean of 26.2 mm (Table 2).
The following factors were considered in the comparative analysis of the results for the two types of procedures:
-
1.
Time needed for the implantation of the distraction device
-
2.
The possibility of adjusting the distraction vector during the distraction protocol
-
3.
Surgical times needed for the removal of the implanted devices
-
4.
Complications
Time needed for the implantation of the distraction device
Most of the studies in the literature do not report the surgical time needed for the distraction devices’ placement specifically; only the description of the relative time needed for this part of the procedure as related to the whole surgery time is usually found. What appears from the analysis of the available data is that surgical time for placement of ICDD is longer than for ECDD ones, although the difference does not reach statistical significance. Our experience confirms these findings, the mean time for ICDD placement being 74 min, compared with 42.5 min for the placement of an ECDD.
The possibility of adjusting the distraction vector during the distraction protocol
There is a general agreement on the very limited possibility of adjusting the distraction vector using ICDD, whereas this kind of management procedure is quite easily performed with ECDD [1, 4, 8, 9].
Surgical times needed for the removal of the implanted devices
As for the implantation, the surgical times needed for the removal of the distraction devices are not reported in literature. In most papers, indeed the time required for the entire surgical procedure is indicated. Nevertheless, it should be pointed out that a second surgical procedure under general anesthesia is always required for the removal of an ICDD, whereas ECDD can be removed in most cases under local anesthesia. The time required for the removal of an ICDD is significantly longer than that necessary for the removal of an ECDD [1–4, 6, 8, 9, 13, 14, 20].
In our cases, the mean surgical time necessary for the removal of an ICDD was 75 min and that for the removal of an ECDD was 24.5 min.
Complications
In the patients included in the ICDD group, the following complications were reported: 14 local infections, 5 mechanical problems due to rupture of a component of the device, 1 transient CSF loss, 1 deviation of the nasal septum, 1 orbital abscess, 4 trisma, 2 strabismus, 1 facial asymmetry at the end of protocol, 1 median palatal fracture, 4 zygomatic-maxillary fractures, and 1 death [1, 2, 6, 8, 14, 19, 20].
No data were reported which relate to Primrose’s criteria for evaluation of the quality of the patients’ life. In our experience, pain was mild in all the four patients. In these patients, no speech problems, no feeding problems, no difficulty in obtaining an adequate level of oral hygiene, and no alteration in local sensitivity were recorded. In all cases, however, mild sleeping problems, moderate disturbances in recreational activities, and a mild psychological impact were observed.
In the patients included in the ECDD group, the following complications were reported: nine local infections and one mechanical problem due to loss of pins [4, 8, 9].
Regarding assessment of the quality of the patients’ life in accordance with Primrose’s criteria, in both the literature and in our experience, pain was mild. Mild speech problems, feeding problems, and difficulty in obtaining an adequate level of oral hygiene were observed. The most severe side effects were sleeping problems, disturbances in recreational activities, and a significant psychological impact [4, 9]. On the other hand, no local sensorial disturbances were described.
Discussion
The data from the literature point to a definite advantage of distraction osteogenesis in terms of advancement, fewer complications, and better functional and aesthetic results compared with traditional osteotomic methods. Consequently, distraction osteogenesis is currently considered as the optimum technique for the treatment of craniofacial malformations in nearly all craniofacial centers throughout the world [1, 4, 8, 9].
Our experience, which is similar to that reported in the literature, further demonstrates that the use of both ICDD and ECDD can significantly improve visual, respiratory, and aesthetic functions in subjects with craniofacial synostosis.
Age is an important factor in the choice of the instrumentation as ECDD is clearly to be preferred for the more collaborative patients [8, 9]. Furthermore, ECDD appear to provide more extended bone osteogenesis advancement than ICDD [1, 8, 9]. On the other hand, there are no differences between the two systems in terms of pathological substratum. A reliable comparative analysis of the impact of the use of the two instrumentations on the surgical procedure is not available for all the papers considered here. However, there is a significantly large amount of data from the literature demonstrating that the surgical time required for the placement of a distraction device is always much longer for ICDD with respect to ECDD. This is because of the need of a perfect insertion for ICDD, which cannot be adjusted in the perioperative period, differently from what occurs for ECDD [4, 8].
Chin and Toth [5] report that the force applied on the bone during the distraction protocol may be as high as 9.5 kg. It is necessary that this force rely on a sufficient resistance of the bone itself, to ensure stability. The orientation of the ICDD is directly related to the direction of the distraction vector as placed during the operation. Thus, during surgical time, the orientation must be carefully evaluated to avoid torsion of the facial axis during the distraction period, or mechanical obstacles, which can lead to fractures or rupture of the device [2, 4, 5, 8]. ICDD applies the force vector on the zygomatic–maxillary junction, a rather weak point of the facial skeleton, especially in the younger patients [8, 9] and constantly applies on it a degree of deformation, which can result to fractures. The plates can be applied on the strongest points of the facial skeleton and the base of the traction is much larger, reducing the chance that the vectorial force applied on it could cause bone deformity rather than effective advancement [5, 8].
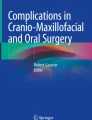
Although positioning and management of the devices are more complicated, the protocol proposed by Arnaud et al. [2] in 2001, with the use of four ICDD, has significantly simplified the surgical procedure. It provides a minimum of control on the distraction vector and decreases force on the individual distraction axis [4]. Other complications are specifically related to ICDD. During removal, several fractures have been reported due to an excessive osteointegration of the device. Even in the authors’ experience, surgical time for the removal of ICDD took longer than 1 h in all four patients as the bone had absorbed the device (Fig. 3). Nevertheless, we did not observe any case of bone fracture [8, 14].

ICDD group. Five-year-old female. Crouzon syndrome. a Intraoperative view at the time of ICDD removal documenting that the device has been partially included in the bone at the level of the temporal fossa. b Intraoperative view after the ICDD removal
The placement of ECDD is very simple and fast, without the need for particular attention to be paid for the choice of the traction site, and the plates can be placed in zones of greater resistance as compared to ICDD [9].
In general, patients in the ECDD group were older and consequently the bone on which the traction force was applied was stronger, thus allowing the application of greater forces to achieve a more extended advancement. The lower bone thickness of the youngest patients might actually make it difficult to evenly apply the plates. However, the utilization of ECDD on patients younger than 12 months has been described [4, 8, 19].
In terms of the management of the distraction vector, strong advantages of ECDD have been noted. This instrumentation allows one to easily modify the direction of the vectors to ensure optimization of advancement with relation to facial harmony [4, 8].
With regards to surgical complications such as the risk of dural lesions, CSF fistulae, meningitis, and necrosis of the mobilized bone, there are no significant differences among the two systems.
Although they are frequently reported, local infections and skin erosion can hardly be avoided, whichever system is utilized. Nevertheless, it is unlikely that these factors can jeopardize the final result, if managed properly.
The most frequent complication in the use of ICDD is the risk of rupture of the device, which results in a new surgical procedure. Furthermore, ICDDs are at risk of fracture of the distracted bone during removal [3, 4].
The possible penetration of the pins of an ECDD in the brain, in case of even mild accidental trauma, is a rare but not exceptional complication which should be taken into consideration, especially when dealing with noncollaborative subjects [8].
The scarce attention paid to the quality of life is quite surprising, as demonstrated by the current analysis. We have attempted to organize the scarce available data according to the criteria suggested by Primrose in 2005.
The use of ICDD does not seem to generate particular discomfort for any of the Primrose’s criteria, whereas speech, feeding, and oral hygiene problems may be significantly affected in patients with ECDD [8, 9, 14]. These difficulties seem to be directly related to the bulky construction of the halo frame. The halo frame also causes sleeping problems such as frequent waking. Finally, often most important for children and adolescents, to note is the psychological impact caused by the ECDD on the relational life [4, 8, 9].
Conclusion
By analyzing the data reported in the literature and from personal experience, ICDD and ECDD differ in terms of surgical management and the quality of the patients’ life. Internal devices are harder to manage from the surgical point of view but are better tolerated by patients. External devices are friendlier for surgical management, but they have a negative impact on the quality of patients’ daily life.
Internal devices have a specific indication in patients under school age. Younger children are indeed less cooperative and find it difficult to bear the mechanical and the psychological stress caused by the bulkiness of the halo frame. On the other hand, external devices should probably be preferred in adolescents and adult patients, because they offer easier implantation and better control of the vectors of distraction and assure more predictable and effective final results.
References
Akizuki T, Komuro Y, Ohmori K (2000) Distraction osteogenesis for craniosynostosis. Neurosurg Focus 9(3):e1
Arnaud E, Marchac D, Renier D (2004) Quadruple internal distraction with early frontal-facial avancement for faciocraniodysostosis. Rev Stomatol Chir Maxillofac 105(1):13–18
Bertele G, Mercanti M, Stella F, Albanese M, De Santis D (2005) Osteodistraction in the craniofacial region. Minerva Stomatol 54(4):179–198
Bradley JP, Gabbay JS, Taub PJ, Heller JB, O’Hara CM, Benhaim P, Kawamoto HK Jr (2006) Monobloc advancement by distraction osteogenesis decreases morbidity and relapse. Plast Reconstr Surg 118(7):1585–1597
Chin M, Toth BA (1996) Distraction osteogenesis in maxillofacial surgery using internal device: review of five cases. J Oral Maxillofac Surg 54(1):45–53
Cho BC, Hwang SK, Uhm KI (2004) Distraction osteogenesis of the cranial vault for the treatment of craniofacial synostosis. J Craniofac Surg 15(1):135–144
Converse JM, Wood-Smith D, McCarthy JG, Coccaro PJ (1974) Craniofacial surgery. Clin Plast Surg 1(3):499–557
Gosain AK, Santoro TD, Havlik RJ, Cohen SR, Holmes RE (2002) Midface distraction following Le Fort III and monobloc osteotomies: problems and solutions. Plast Reconstr Surg 109(6):1797–1808
Kubler AC, Speder B, Zoller JE (2004) Fronto-orbital advancement with simultaneous LeFort III-distraction. J Craniomaxillofac Surg 32(5):291–295
Marchac D, Cophignon J, Neulen JV, Bouchta M (1974) Osteotomy for advancement of the face and skull. Ann Chir Plast 197419(4):311–323
McCarthy JG, Coccaro PJ, Eptstein F, Converse JM (1978) Early skeletal release in the infant with craniofacial dysostosis: the role of the sphenozygomatic suture. Plast Reconstr Surg 62(3):335–346
McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH (1992) Lengthening the human mandible by gradual distraction. Plast Reconstr Surg 89(1):1–8
Meling TR, Due-Tonnessen BJ, Hogevold HE, Skjelbred P, Arctander K (2004) Monobloc distraction osteogenesis in pediatric patients with severe syndromal craniosynostosis. J Craniofac Surg 15(6):990–1000, discussion 1001
Nonaka Y, Oi S, Miyawaki T, Shinoda A, Kurihara K (2004) Indication for and surgical outcomes of the distraction method in various types of craniosynostosis. Advantages, disadvantages, and current concepts for surgical strategy in the treatment of craniosynostosis. Childs Nerv Syst 20(10):702–709
Ortiz-Monasterio F, del Campo AF, Carrillo A (1978) Advancement of the orbits and the midface in one piece, combined with frontal repositioning, for the correction of Crouzon’s deformities. Plast Reconstr Surg 61(4):507–516
Polley JW, Figueroa AA (1997) Management of severe maxillary deficiency in childhood and adolescence through distraction osteogenesis with an external, adjustable, rigid distraction device. J Craniofac Surg 8:181–185
Primrose AC, Broadfoot E, Diner PA, Molina F, Moos KF, Ayoub AF (2005) Patients’ responses to distraction osteogenesis: a multi-centre study. Int J Oral Maxillofac Surg 34(3):238–242
Tessier P, Guiot G, Rougerie J, Delbet JP, Pastoriza J (1967) Cranio-naso-orbito-facial osteotomies. Ann Chir Plast 12(2):103–118
Yano H, Tanaka K, Sueyoshi O, Takahashi K, Hirata R, Hirano A (2006) Cranial vault distraction: its illusionary effect and limitation. Plast Reconstr Surg 117(1):193–200, discussion 201
Yonehara Y, Hirabayashi S, Sugawara Y, Sakurai A, Harii K (2003) Complications associated with gradual cranial vault distraction osteogenesis for the treatment of craniofacial synostosis. J Craniofac Surg 14(4):526–528
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Pelo, S., Gasparini, G., Di Petrillo, A. et al. Distraction osteogenesis in the surgical treatment of craniostenosis: a comparison of internal and external craniofacial distractor devices. Childs Nerv Syst 23, 1447–1453 (2007). https://doi.org/10.1007/s00381-007-0475-6
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-007-0475-6