
Abstract
Objectives
In 1996 we published our results for treatment of childhood craniopharyngioma. That study did not only reveal that there was a significant morbidity associated with our then policy of attempted radical removal followed by post-operative radiotherapy in those cases with residual disease, but also that risk factors for poor outcome could be identified based on the clinical and radiological findings at presentation. As result of that study, we redefined the role of radical surgery in the treatment of craniopharyngioma and developed a new treatment strategy in an attempt to improve the quality of outcome without compromising tumour control. Our aims in this paper were to compare the results of our current treatment strategy with that reported in the 1996 paper to assess whether we have achieved this goal.
Methods
A detailed assessment of the treatment pathway and outcome was undertaken for children treated for craniopharyngioma in our unit from 1996 to 2004. This included a morbidity score based on visual, motor, cognitive, hypothalamic and endocrinological data obtained from our neuro-oncology database and review of clinical records. Where possible we have attempted to record data in the same manner as for our previous study allowing for meaningful comparison.
Results
Forty-eight children with craniopharyngioma presented in the study period. On the basis of clinical presentation and radiological findings, 25 were deemed suitable for attempted radical surgery and 23 were treated with various subtotal surgical procedures. Radiotherapy was used in patients over the age of 5 years where residual tumour was present or progressed after the initial surgical intervention(s). Morbidity scores, particularly in relation to visual and cognitive outcome, are improved and there was no surgical mortality in the current series.
Conclusions
A treatment paradigm for childhood craniopharyngioma is presented which improves the quality of outcome without compromising tumour control.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Radical surgery has been the perceived treatment of choice for craniopharyngioma for many years. A survey published in 1994 revealed that this was the favoured primary treatment modality for the overwhelming majority of American paediatric neurosurgeons [7]. There are therefore large numbers of published clinical series reporting variable numbers of cases from individual institutions which collectively give us some idea about the outcome of the results of radical surgery for this tumour. Ten-year survival is achieved in 69% of these cases. Diabetes insipidus is an almost inevitable consequence of radical surgery, and impairment of anterior pituitary function necessitating replacement of two or more anterior pituitary hormones is seen in approximately 80% of cases [4, 9]. The non-endocrine morbidity (approximately 15%) must also be considered including the often devastating consequences of hypothalamic damage resulting in obesity, severe appetite disturbance, loss of diurnal rhythm and cognitive impairment [1]. The impact of such morbidity on daily living, sociability, academic attainment and employment prospects has been hitherto under recognised. If, in addition to this, it is remembered that the published mortality following radical resection is in the order of 10% even in contemporary series [5, 8], then it is indeed fitting that the neurosurgical community should re-examine its role in the management of this pernicious tumour.
Prior to 1996 our default treatment policy had been to attempt a surgical cure by carrying out as radical a procedure as possible—and to reserve radiotherapy (RT) for those patients who had had an incomplete removal or whose tumours had recurred despite an apparently complete removal. In 1996 we published an extensive review of our experience of the management of childhood craniopharyngioma [2]. The impact of this treatment policy in terms of operative morbidity, long-term endocrine and neurocognitive outcome was a major emphasis of that review.
The results of that review can be summarised as follows:
-
1.
The ill effects of radical surgery (particularly upon hypothalamic function) can largely be predicted.
-
2.
Factors predictive of a poor prognosis following radical surgery were
-
(a)
At presentation
-
(i)
Degree of hydrocephalus
-
(ii)
Size of tumour (as judged by the number of intracranial compartments involved)
-
(iii)
Age less than 5 years
-
(iv)
Presence of signs of hypothalamic disturbance (most commonly obesity)
-
(i)
-
(b)
At surgery
-
(i)
An intra-operative complication (most commonly vascular)
-
(ii)
Removal of tumour observed to be adherent to the hypothalamus
-
(i)
-
(a)
In addition to our ability to predict morbidity following radical surgery, we also found the following factors to be significant for the prediction of cure.
-
1.
Small tumour size
-
2.
Age more than 5 years at presentation
-
3.
Complete surgical resection
-
4.
No or mild hydrocephalus at presentation
-
5.
Radiotherapy—radiotherapy was confirmed as an effective curative treatment for craniopharyngioma [“The actuarial 10-year recurrence-free survival after radiotherapy (including treatment given for recurrent disease) was 72% at a median follow-up assessment of 7.6 years”.]
As a result of our (published) experience, we changed our management of childhood craniopharyngioma to a model whose emphasis is flexibility. There is now no automatic “default” management policy, but instead an algorithm that takes into account the various factors we have found to be important if the cure rate is to be kept as high as possible while restraining morbidity (particularly with regard to hypothalamic function) within acceptable limits (Figs. 1, 2).

Algorithm for craniopharyngioma with good risk factors

Algorithm for craniopharyngioma with poor risk factors
In 2004 we joined with our radiotherapy colleague at the Royal Marsden Hospital, Dr. Micheal Brada [3], to present a joint surgical/radiotherapy/paediatric review of the management of childhood craniopharyngioma.
The purpose of this article is to compare our current approach with our previous management policy. It should be emphasised that we cannot present here our results in exactly the same format as in our 1996 paper, although we have attempted to do so as far as possible. The following is a brief account of the status of the treated children in each cohort (past and present) both in terms of the treatment paradigm followed (tumour outcome) and the morbidity associated with this treatment (clinical outcome).
Treatment of craniopharyngioma at our hospital prior to 1996
Tumour control
Of the 75 children aged 16 years and under whose results we reported in 1996, the initial aim of the neurosurgeon was to attempt a total excision in 59 and a subtotal excision in 16 (many of whom were operated in the years close to 1994 when the ill effects of radical surgery were becoming all too apparent). However, surgery resulted in an apparently total excision in only 39 (of whom 29 were shown to have residual tumour on post-operative imaging).
Elective (“early”) external fractionated radiotherapy (RT), 55 Gy over 30 fractions, was given to 16 children following their primary surgical procedure and to 19 children following recurrence.
The overall 10-year actuarial survival was 88% at a median follow-up review of 5.2 years.
Clinical outcome
To assess morbidity we devised a scoring system that incorporated data on each child’s vision, endocrine status, neurology, education and hypothalamic functions (Table 1). The worst score on this scale was 15. When 66 surviving children were assessed, 13 (20%) were found to be severely affected with scores between 10 and 14 (those children who had not survived had morbidity scores of 12 or more following their initial surgery).
Current treatment of craniopharyngioma at our hospital
Since 1994 we have treated 48 children (age range, 7 months–15 years) newly presenting with craniopharyngioma (plus a further six who received treatment for recurrences of tumours that had presented prior to 1994). In this more recent cohort, children were stratified at presentation into (1) those in whom—given the clinical presentation and radiological appearances—it was deemed appropriate to attempt a radical resection, and (2) those where a subtotal resection or simple cyst aspiration was undertaken as part of a staged approach to treatment integral to which was treatment with RT either immediately or anticipated but deferred usually by virtue of the child’s young age. The follow-up for this current cohort is 1–132 months (median 67 months).
Tumour control
The initial surgical management of these recent cases exemplifies the element of flexibility (Table 2). A variety of surgical approaches, including the trans-sphenoidal approach and image guided cyst aspiration, have been utilised according to the age of the child and the anatomical configuration of the tumour.
Radical surgery was chosen as the primary curative treatment in 25 of the 48, in six of whom it was preceded by an emergency cyst aspiration (usually because of rapidly deteriorating vision). In 16 out of theses 25 cases, a complete resection was achieved as judged by post-operative MR imaging. During the course of follow-up, eight children have remained tumour-free and eight have recurred at a median time of 33 months (range 23–53 months). These recurrences have been treated with a combination of further surgery (craniotomy, trans-sphenoidal surgery or cyst aspiration) or RT. In the nine patients where residual disease was present on post-operative imaging, a policy of surveillance was pursued: four developed progressive disease (median time to progression, 24 months; range 9–48 months) and have gone on to receive RT, whilst in the other five the residual tumour has remained static during the course of surveillance (four have follow-up of more than 9 years, one has 12 months of follow-up).
For the remaining 23 patients a treatment strategy was formulated incorporating the wish to avoid radical surgery. Seventeen had elective subtotal surgical procedures followed by RT. Fourteen of these children have shown no evidence of tumour recurrence/progression, and three have required a total of seven procedures for drainage of re-accumulating tumour cysts during the first year following treatment. Of the six who had subtotal surgery alone followed by a period of surveillance (usually because of the wish to avoid RT in the very young), five are known to have recurred and one has been lost to follow-up. One child received single-dose radiotherapy (Gamma knife or Linnac) for treatment of localised foci of recurrence away from the visual apparatus and hypothalamus.
The treatment pathways followed by this group of children are summarised in Fig. 3. There was no post-operative mortality in this current series.

Treatment pathway for current series
Of the 48 children in our current study, 24 have had regular clinical and radiological (MR scan) follow-up for 5 years or more following their last “attempted curative” treatment. Of these, nine have no radiological evidence of residual tumour and 15 have abnormal residual tissue on their scan but no evidence of tumour progression over this period. We submit that these 24 children should be considered cured.
Clinical outcome
Applying the scoring system used in our previous study to our surviving children (using the hospital’s neuro-oncology database and clinical records for this purpose rather than recalling all the children for a 48-h in-patient assessment period as we did for that study), we find that two children (4%) scored between 10 and 14 as opposed to 13/66 (20%) in our previous study.
The scoring system used is essentially the same for both groups (Table 1). The only difference is with respect to educational/cognitive status. IQ scores were available for some, but not all in the more recent group. Where this information was not available the score was applied according to educational requirements. More details of the 1996 definitions can be found in the original paper [2]. A comparison of the results for each of the parameters scored is shown in Tables 3, 4, 5, 6, 7.
Two patients in our present study have died. One child whose post-operative morbidity score was 1 (related to endocrine requirements) died suddenly of unknown causes in his country of origin 2 years following his treatment. The second child (early post-primary treatment morbidity score 3) died of tumour recurrence 105 months after his initial presentation.
Illustrative case histories
Case 1
An 8-year-old boy presented with a history of headache, lethargy and visual impairment. MRI scan revealed a large solid and cystic tumour extending into the posterior and middle cranial fossae on the left, and a solid tumour could be seen in the region of the hypothalamus. There was associated hydrocephalus. The tumour was approached via a left pterional craniotomy, and a subtotal resection was performed; the optic nerves and chiasm were decompressed. The solid tumour in the region of the hypothalamus was left undisturbed. Post-operatively, the child made an uneventful recovery, and the hydrocephalus resolved without recourse to a shunting procedure. The presenting symptoms and signs including visual impairment resolved completely. The child went on to receive focal radiotherapy. At 4 years follow-up, evidence of tumour residuum in the suprasellar region was seen; this has remained unchanged over the course of serial scans. The child is in full-time education, on single hormone replacement therapy (growth hormone), and has no diabetes insipidus (Fig. 4a,b).

a, b Case 1: sagittal MRI scans at presentation and at 4 years follow-up
Case 2
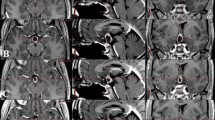
This 9-year-old boy presented with a history of lethargy, polydipsia and polyuria. He had bilateral papilloedema but normal visual acuity. MRI revealed a solid/cystic suprasellar mass producing obstructive hydrocephalus. Surgical treatment comprised cyst aspiration and sterotactic placement of a catheter and reservoir. The aspirated fluid confirmed the diagnosis of craniopharyngioma. The presenting symptoms and hydrocephalus resolved following this procedure. The child went on to receive radiotherapy. During radiotherapy he required aspiration because of re-accumulation of cyst fluid on two occasions. At 6 years follow-up, residual solid tumour was observed in the sellar region; however, this has remained stable since completion of radiotherapy. Visual function is normal, and the patient remains on thyroxine, growth hormone and testosterone. There is no diabetes insipidus. He continues in full-time normal education (Fig. 5a,b).

a, b Case 2: coronal MRI scans at presentation and at 5 years follow-up
Discussion
Craniopharyngiomas remain rare tumours of childhood. Approximately five children per year were admitted to our unit as new cases in the 10-year period that began in 1994—a similar rate to that described in the earlier study from our unit published in 1996.
In our 1996 study we discussed our results in terms of tumour control and mortality and morbidity. We shall do the same here and then make some “general comments”.
Mortality and morbidity
In our previous study we reported nine tumour-related deaths in 75 children (12%) who were treated between 1973 and 1994. In the 10 years following 1994, we have had two deaths (4%)—one definitely tumour-related, the other in a child who suddenly died 2 years after returning to his own country, having apparently been well until then and requiring only hormonal replacement therapy.
Before discussing changes in morbidity between the two studies, it should be noted that exact comparisons cannot be made and what we present here are inferences based upon information that has been gathered in different ways. For our 1996 study, a “dedicated” neurologist-in-training (Dr. Catherine DeVile) recalled all surviving craniopharyngioma patients for an intensive neurological, psychological, ophthalmological, radiological and endocrinological review. For our present study, we have drawn on information entered contemporaneously with each child’s medical attendance into a neuro-oncology database, as well as examination of the hospital records. The details from which our morbidity scores have been drawn have therefore been gathered in different ways and vary slightly in themselves. We would contend, however, that the similarities outweigh the dissimilarities sufficiently to allow meaningful comparisons to be made.
It should also be noted that regarding the status at presentation of the children in the 1996 study, we only have figures for the presence of hypothalamic disability.
Comparison of the cumulative morbidity scores from the two studies confirms our prediction that a more flexible approach to treatment would reduce mortality—a reduction from 20 to 4% of children scoring 10–14 according to our grading system. However, within the total scores there are significant variations showing that there is still considerable room for improvement. For example, with regard to vision, the overall outcome has improved (60% as opposed to 32% being graded as “normal”), and for the contemporary cohort tumour treatment is successful in improving vision (41% “normal” at presentation, 60% “normal” at their most recent assessment).
The effect upon endocrine status largely remains as before. Although 27% of children have evidence of endocrinopathy at presentation, this number rises to 92% following treatment (99% in the previous study). However, there are important improvements in the “severity” of the endocrinopathy. For example, in the original series 80% of patients had permanent DI, in 16% of whom this was further complicated by reduced or absent thirst (adipsic DI). In the current series, as a whole 73% of patients have required ongoing treatment for DI, two of whom (6%) are adipsic. If the 23 patients who had subtotal surgery and radiotherapy are considered separately, only 52% have DI.
It is also interesting to see that there has been little change in the effect on hypothalamic function—one of the main stimuli for us to re-assess our management policies for children with craniopharyngioma. Whilst this may be a real finding, it is difficult to reconcile with the improvement in educational/cognitive status (see below). The sequelae of hypothalamic disturbance are manifest in a number of ways and are often difficult to quantify (Keating, this edition). The earlier cohort was specifically assessed for hypothalamic disturbance, whereas in the recent series it has been inferred on the basis of a retrospective review of clinical records. Our current assessment may thus be insufficiently sensitive to demonstrate a real difference.
The effect of treatment on the children’s educational/cognitive status has undoubtedly improved (62% attending a normal school and with no educational concerns as opposed to 37% graded in 1996 as normal IQ>90). But at presentation 45 (94%) of our present cohort were reported as receiving normal education, so treatment is still responsible for significant educational/cognitive morbidity.
Contemporary treatment is also responsible for a small deterioration in neurological status (down from 94% normal pre-operatively to 80% post-operatively) but this is still an improvement compared to the 33% assessed as neurologically normal post-treatment in the 1996 study.
General comments
In 1996 we predicted that a more flexible approach to the management of childhood craniopharyngioma would reduce treatment-related morbidity, particularly that following attempted (curative) radical surgery. Although numbers are of necessity small, it is our opinion that we have been successful in this aim. However, our study also shows that despite a drop in tumour-related mortality, morbidity as demonstrated by, for example, the post-treatment drop in cognitive/educational status remains a major issue. Final visual outcome is shown to be related to acuity at presentation and despite the increasing use of elective radiotherapy as the primary “curative” treatment, the endocrine morbidity remains much as before.
There are therefore improvements to be made. What might they be?
The role of radical surgery
Although not analysed with this question in mind, these figures do raise the issue of whether there remain any indications for radical (attempted surgically curative) surgery in the management of childhood craniopharyngioma, particularly given the efficacy of RT. In our opinion, the answer is yes—but those indications are limited. Conventional fractionated RT, however delivered, has a cure rate of 70–80% but it carries a significant morbidity of its own, a morbidity that increases the younger the child. There will therefore always be pressure to postpone its use for as long as is practical. While this may involve elective sub-total tumour removal and/or cyst aspirations, a minority of tumours (as identified in the protocols described in Figs. 1 and 2) will remain amenable to attempted curative surgery as their primary method of treatment. It is also important to distinguish between two categories of subtotal removal—that which is “elective” (from which the morbidity should be low) and that which represents a failed attempt at radical removal (from which the morbidity is likely to be higher).
There are also those tumours that have recurred despite radiotherapy. Some of these will have been deemed unsuitable for radical surgery at presentation. The surgeon will then be faced with the difficult decision as to whether an attempt should now be made at a surgical cure despite the previously predicted morbidity that such a procedure is likely to produce.
Nevertheless, it is difficult to escape the conclusion that the avoidance of radical surgery as a primary curative treatment option is associated (at least in our hands) with a gratifying reduction in post-operative morbidity without a subsequent fall in rates of cure.
Intra-cyst therapy
Our experience of yttrium is too limited to report here and we have not as yet used intra-cyst bleomycin. How successful these treatments are remains a matter of controversy with some units reporting enthusiastically upon them [6], while others describe (usually by word of mouth) problems that have led to their being abandoned. What can be said, however, is that their efficacy is likely to be greatest in those tumours that are predominantly cystic.
Increasing the range of the surgical “armamentarium”
Of particular note in our contemporary series is the range of modalities currently employed in the treatment of childhood craniopharyngioma. For example, an increasing number require image guidance not only for the accurate placement of cyst catheters and for cyst aspiration but also for craniotomies aimed at bulk tumour removal. We would not be able to offer the service we do unless it was possible to draw upon expertise in trans-sphenoidal surgery—a skill that may not always be available in dedicated paediatric units where pituitary surgery is uncommon. This has implications not only for the surgical skills required, but also for the equipment available.
Radiotherapy requires not only access to experience in the use of stereotactic methods of focussed treatment (conformal fields) for the delivery of external fractionated treatment but also to “radio-surgery” for those tumours (primary or recurrent) considered sufficiently far from the visual apparatus, hypothalamus, etc. to make them a safe alternative.
Concentration of cases
The management of these rare tumours raises complex issues for a broad range of specialists involved in their care—not only paediatric oncologists (medical, surgical and radiotherapy) and endocrinologists for their initial management, but endocrinologists, neurologists, psychologists and ophthalmologists for their after-care and surveillance. Few single paediatric units can publish results of treating more than 50 cases, and these may have been accrued over a period of time that makes it difficult to derive any useful guidance from them. There is no excuse therefore for the primary care of these children to be undertaken outside a paediatric unit that sees at least five patients a year and can field the necessary expertise for their aftercare.
Conclusions
The mortality and morbidity of radical surgery for childhood craniopharyngioma has been well documented by us and others. Radical surgery is an effective treatment in terms of tumour control and will continue to have a role in treatment of selected cases. Our current philosophy recognises the efficacy of radiotherapy in the treatment of this tumour, the importance of flexibility in surgical approach, and the role multi-disciplinary input at all stages of management.
Based upon this comparison between our earlier results and our contemporary experience, we believe that our current philosophy of management of childhood craniopharyngioma has gone some way towards achieving our goal of improving the quality of survival without compromising tumour control.
References
De Vile CJ, Grant DB, Hayward RD, Kendall BE, Neville BG, Stanhope R (1996) Obesity in childhood craniopharyngioma: relation to post-operative hypothalamic damage shown by magnetic resonance imaging. J Clin Endocrinol Metab 81:2734–2737
De Vile CJ, Grant DB, Kendall BE, Neville BG, Stanhope R, Watkins KE, Hayward RD (1996) Management of childhood craniopharyngioma: can the morbidity of radical surgery be predicted? J Neurosurg 85:73–81
Hayward R, De Vile CJ, Brada M (2004) Craniopharyngioma. In: Walker D, Perilongo G, Punt J, Taylor R (eds) Brain and spinal tumours of childhood. Arnold, London, pp 370–386
Hoffman HJ, De Silva M, Humphreys RP, Drake JM, Smith ML, Blaser SI (1992) Aggressive surgical management of craniopharyngiomas in children. J Neurosurg 76:47–52
Kang JK, Lee KS, Hong YK, Jeun SS, Kim MC (2005) Endocrine management following craniopharyngioma surgery in children. Childs Nerv Syst 19:625
Mottolese C, Stan H, Hermier M, Berlier P, Convert J, Frappaz D, Lapras C (2001) Intracystic chemotherapy with bleomycin in the treatment of craniopharyngiomas. Childs Nerv Syst 17:724–730
Sanford RA (1994) Craniopharyngioma: results of survey of the American Society of Pediatric Neurosurgery. Pediatr Neurosurg 21(Suppl 1):39–43
Wisoff JH, Sands S, Moliterno J, Milner J (2005) Functional outcome following radical resection of primary and recurrent craniopharyngioma. Childs Nerv Syst 19:624
Yasargil MG, Curcic M, Kis M, Siegenthaler G, Teddy PJ, Roth P (1990) Total removal of craniopharyngiomas. Approaches and long-term results in 144 patients. J Neurosurg 73:3–11
Acknowledgements
The authors would like to acknowledge Mr. M. Powell, Consultant Neurosurgeon (National Hospital for Neurology and Neurosurgery, Queen Square) for providing his expertise in trans-sphenoidal surgery in the management of our patients.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Thompson, D., Phipps, K. & Hayward, R. Craniopharyngioma in childhood: our evidence-based approach to management. Childs Nerv Syst 21, 660–668 (2005). https://doi.org/10.1007/s00381-005-1210-9
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-005-1210-9