
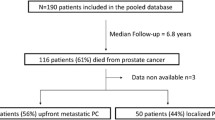
Abstract
Purpose
Time to metastasis is often used as a surrogate parameter of treatment success in clinical trials for prostate cancer. However, it has not been shown that there is a clear correlation between time to metastasis and overall survival. Our objective was to evaluate the impact of time to metastasis on OS in patients with prostate cancer.
Methods
Between 2008 and 2015, 269 patients with mPCa were included in this retrospective study with a median follow-up of 7.1 years. Patients were divided into three groups: (1) Presentation with metastasis within three months of initial diagnosis (de-novo-M); (2) patients free of metastasis initially but developed metastasis more than 6 months prior to castration resistance (CSPC-M); (3) patients who developed metastasis within 6 months of becoming castration resistant or after (CRPC-M).
Results
There was a significant decrease in OS when metastases were present at diagnosis (median 6.39 years) compared to CRPC-M (19.07) and CSPC-M (18.19 years). De-novo-M and CSPC-M showed a longer OS from occurrence of metastasis to death when compared to CRPC-M, although reaching CRPC earlier. There was no difference in OS between the groups once castration resistance was reached. Time from initial diagnosis to metastasis and to CRPC was correlated with OS and remained important prognosticators in multivariate Cox-regression (p < 0.01 for both).
Conclusions
Time from diagnosis to CRPC (all patients) and time to metastasis (for CRPC-M and CSPC-M patients) are significant prognosticators of overall survival and are therefore valid surrogates in a study setting. Therefore, time to CRPC should be prolonged as long as possible.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Prostate cancer (PCa) represents the most common cancer among North American males with 180,890 estimated new cases in 2016 [1]. Although the overall survival (OS) increased over the last two decades [2], patients with PCa diagnosed with de-novo metastatic or metastasis after initial local therapy still have poor outcomes. This stage of PCa remains a lethal disease accounting for over 26,020 estimated deaths in 2016 in the US [1]. Several groups have evaluated the impact of clinical features on the outcome of non-castration-resistant metastatic [3, 4] and castration-resistant metastatic [5,6,7] PCa. However, despite little is known about the impact of the time of occurrence of metastasis on the survival of patients with PCa, several studies are looking at time to metastasis as a surrogate parameter for survival [8, 9].
In addition to patients with metastasis at original presentation, some patients with localized disease develop metastases after primary therapy of their PCa. The most common clinical scenario of metastasis consists of patients relapsing after initial treatment with curative intent diagnosed through radiological or clinical evaluation. In addition, patients with locally advanced disease with no clinical evidence of metastatic disease may be treated with androgen deprivation therapy after a rise in PSA without radiological or clinical evidence of distant metastasis, leading to a subset of patients that develop metastases after becoming castration resistant. The aim of this study is to evaluate the impact of the time of occurrence of metastasis on overall survival with prostate cancer.
Materials and methods
Study design
In this retrospective study, we identified 269 prostate cancer patients treated at the Vancouver Prostate Centre and the British Columbia Cancer Agency from 2008 to 2015 that developed metastasis in the course of their disease and had progressed to CRPC. Patients were classified into three groups according to the time of occurrence of metastases: (1) patients that presented with clinical evidence of metastasis within 3 months of initial diagnosis (de-novo-M); (2) patients who were initially free of metastasis but developed metastasis more than 6 months prior to castration resistance (castration-sensitive prostate cancer with metastasis-CSPC-M); (3) patients who developed metastasis within 6 months of becoming castration resistant or after, (castration-resistant prostate cancer with metastasis-CRPC-M) (Supplementary Fig. 1). We chose this 6 months time schedule to account for the fact that our surveillance strategy usually involves evaluating the patients every 3–6 months depending on their clinical performance and PSA kinetics once experiencing a biochemical failure. Biochemical failure was defined according to the EAU guidelines, for patients treated with radical prostatectomy, two consecutive PSA values of > 0.2 ng/ml and rising and for patients after radiotherapy, any PSA increase > 2 ng/ml higher than the nadir [10].
Castration resistance was defined according to the EAU guidelines as either biochemical progression consisting of three consecutive rises in PSA 1 week apart, resulting in two 50% increases over the nadir, with PSA > 2 ng/mL or radiological progression with the appearance of two or more new bone lesions on bone scan or enlargement of one soft tissue lesion using RECIST—(Response Evaluation Criteria in Solid Tumours) criteria [10]. Testosterone levels were not available in all patients and therefore not included in the definition of castration resistance. All patients were followed-up on a regular basis as per standard of care at our institution. This included at least annually performed Technetium-99 m bone scan and CT scan at least annually in CPSC patients and with any PSA rise or development of symptoms. Imaging frequency was increased to at least 6 months once castration-resistant disease was developed.
Study population
Of the total cohort of 269 patients, we identified 123 patients with de-novo-M, 60 with CSPC-M and 86 with CRPC-M. All patients reached CRPC in the time of follow-up. 68 patients received primary radical prostatectomy (RP), 75 received primary radiotherapy (RT), and 126 patients were initially not treated with a local therapy due to significant metastatic disease, patients’ preferences or contraindications against local intervention (patients age, comorbidities e.g.). Salvage RP was performed in eight cases and salvage RT in 21 cases. Patients in the de-novo-M group received less local treatment than patients in the other groups (Table 1). This is also represented in a higher clinical stage and higher PSA values at diagnosis for patients with de-novo-M compared to all other groups. None of the patients received stereotactic body radiation therapy to their metastases. Age at diagnosis was evenly distributed throughout patient groups with a mean age of 66.89 years (range 45–92.3).
Data analysis
Kaplan–Meier estimates of overall survival time, defined as death of the patient, were calculated, and subgroups were compared by the log-rank test. Continuous variables were reported as mean values and range for parametric distributions or as median values and interquartile ranges (IQR) for non-parametric distributions. Chi-square or Fisher’s exact tests were conducted to assess differences in covariate distributions. Correlations of continuous and normal distributed variables were calculated as Pearson correlation. Univariate and multivariate Cox-regression were performed to verify the influence of various prognosticators of OS. SPSS 20.0 (IBM, Armonk, NY, USA) was used for statistical assessment. In all tests, a two-sided p < 0.05 was considered to indicate significance.
Results
The median follow-up was 3.79, 10.1, and 13.15 years for de-novo-M, CSPC-M and CRPC-M, respectively. Patients in the CRPC-M and de-novo-M group had more advanced clinical stage at diagnosis than CSPC-M patients (p < 0.001). The PSA value at diagnosis was significantly higher in the de-novo-M group, whereas CRPC and CSPC showed similar PSA values. CRPC-M and de-novo-M patients showed higher Gleason scores than CSPC-M at diagnosis. Patient characteristics are shown in Table 1.
During the time of follow-up 142 patients died. 49.2% (30/60) patients with CSPC-M, 45% (45/86) patients with CRPC, and 67% (67/123) patients with de-novo-M were deceased. Kaplan–Meier and log-rank analysis revealed a significantly shorter overall survival from initial diagnosis for patients with de-novo-M compared to patients in the CRPC-M or CSPC-M group (p < 0.001) (Fig. 1a). In contrast, patients with CRPC-M patients had the shortest median overall survival from the date of diagnosis of their metastases (2.94 years) compared to CSPC-M (7.01 years and de-novo-M patients (6.41 years) (p = 0.001). (Supplementary Fig. 2).

a Survival from time of diagnosis. Kaplan–Meier analysis of the overall survival of patients from time of diagnosis. b Time from diagnosis to CRPC. Kaplan–Meier analysis of the time to becoming castration resistant from diagnosis
De-novo-M patients progressed to CRPC significantly earlier from diagnosis (median 1.85 years (SE 0.24 years) than CSPC-M [7.27 years (SE 1.29 years)] and CRPC-M [9.15 years (SE 1.87 years)] patients (Fig. 1b). There was no significant difference between the time from metastasis to CRPC between the CSPC-M and the de-novo-M group. Once castration-resistant stage was reached, there was no difference in the survival between all groups (Supplementary Fig. 5). Treatments after CRPC (abiraterone, enzalutamide, docetaxel) were similar within groups with variable sequences and combinations. There was no use of docetaxel in a castration-sensitive setting.
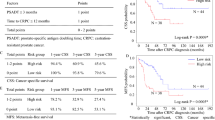
There was no difference in survival from diagnosis between CSPC-M and CRPC-M patients (Fig. 1a) CSPC-M patients metastasized significantly earlier (median time 6.77 years (SE 0.75 years) from diagnosis than CRPC-M patients 10.85 years (SE 0.70 years) (Supplementary Fig. 3). Time from metastasis to death was significantly shorter in patients with CRPC-M compared to CSPC-M (Supplementary Fig. 2). Pearson correlation revealed that within patients that did not have metastases at diagnosis, time to metastasis is correlated positively with overall survival (r = 0.897, p < 0.001, Supplementary Fig. 4a) as well as time to CRPC in all patients (r = 0.962, p < 0.001, Supplementary Fig. 4b). Table 2 gives an overview of times between different events. A subset of these patients, who developed metastases within 5 years of diagnosis, showed a similar short overall survival time to patients with de-novo metastasis (Supplementary Fig. 6).
Univariate and multivariate Cox-regression revealed time to metastasis (for CSPC-M and CRPC-M patients) and time to CRPC (for the entire cohort) as well as patient age at diagnosis to be independent prognosticators of OS. (Supplementary Table 1).
Discussion
In this retrospective study, we describe the impact of the time occurrence of metastasis on survival outcomes in prostate cancer. To our knowledge, this is the first data to show that time to metastasis and time to CRPC correlate with overall survival in patients with metastatic prostate cancer. These data show that time to metastasis and time to development of CRPC is a useful surrogate for overall survival when evaluating the impact of new therapies in prostate cancer. Trials such as the SPARTAN trial [9] (evaluating apalutamide (ARN-509) in men with Non-Metastatic Castration-Resistant Prostate Cancer) or the PROSPER trial [8] (a phase 3 study of enzalutamide in non-metastatic (M0) castration-resistant prostate cancer (CRPC) patients) are already using time to metastasis as clinical endpoints.
Our data show that the results of the primary endpoints of these trials may result in a translation into overall survival as well. Selecting time to metastasis rather than overall survival results in a shorter time for events to occur and a shorter time for patients to be followed up.
In addition, we show that patients with metastasis at presentation have a significantly different natural history than patients that develop metastasis while being castration sensitive or after becoming castration resistant. Similar results have been published by Patrikidou et al. in their manuscript evaluating the factors increasing the likelihood of dying from prostate cancer in 113 men with mPCa [11]. They showed that of these patients 56% had metastasis at diagnosis with a similar median overall survival as the de-novo patients in our cohort of about 5.2 years. Interestingly, these patients progressed to CRPC earlier than the patients in our cohort. This might be due to the fact that 26 out of 123 of our de-novo patients received some sort of local treatment despite metastasis at diagnosis [11]. This group also showed that there was a non-significant trend for longer OS and longer time to CRPC in favor of patients with mPCa undergoing loco-regional treatment at diagnosis compared to those that were only treated systemically [12]. We show that patients with de-novo metastasis have the shortest overall survival and reach castration resistance faster than patients developing metastasis after initial diagnosis. A subset of these patients that develop metastasis within the first 5 years after diagnosis seem to have a more aggressive cancer and show a similar overall survival even compared to de-novo metastatic patients. For patients with CRPC-M and CSPC-M, the time to metastasis correlates with the overall survival. For the entire cohort, time to CRPC is also an independent prognosticator. Interestingly, once reaching castration resistance, there is no difference in the survival between the groups, and no differences were seen in the frequency of treatments between the three groups when CRPC is diagnosed.
In addition, these data show that there is a need for aggressive management of de-novo metastatic patients and patients that develop metastasis within 5 years of diagnosis to prolong the time to CRPC as much as possible. The majority of our patients were treated with sequential therapy, receiving androgen deprivation therapy (ADT) after biochemical failure or at the diagnosis of metastases. Recently, two large studies have contributed to a change in the approach of metastatic prostate cancer. The CHAARTED trial [13] showed that six cycles of docetaxel administered at the time of diagnosis of de-novo metastatic hormone-naïve PCa resulted in an increase in median overall survival of 13.6 months compared to those treated with androgen deprivation alone. Interestingly, about 65% of their cohort had “high volume” disease and 73% never underwent curative treatment. Time to CRPC in both arms was shorter than in our cohort (20.2 months in the docetaxel treated group and 11.7 months in the ADT only group), which may be due the difference in tumor burden in our cohort compared to those in CHARRTED. Similar results were seen in STAMPEDE [14] trial that showed an increase in survival of 77 months in patients with metastatic castration-sensitive PCa treated with upfront chemo-hormonal therapy compared to those treated with androgen deprivation alone.
In addition, there were two trials evaluating the effect of abiraterone plus ADT versus ADT alone in a castration-sensitive setting. The LATITUDE trial showed a significantly longer overall survival for patients treated with abiraterone and ADT compared to ADT plus placebo for metastastic high-risk castration-sensitive prostate cancer (not reached vs. 34.7 months) [15]. The STAMPEDE group reported on a second trial arm, evaluating the effect of abiraterone plus ADT and ADT plus placebo in patients with metastatic or high-risk locally advanced prostate cancer. The addition of abiraterone to ADT showed strong evidence of a survival benefit after 3 years compared to ADT alone (83% vs. 76%) [16]. Both studies emphasized the efficacy of a combination therapy and a more aggressive treatment of de-novo as well as high-risk prostate cancer.
It is difficult to compare our data to the subset of patients in the control arm of these studies. Survival and progression data from the trials do not include time to CRPC as a single analysis. In the control arm of the STAMPEDE trial (ADT alone treatment), failure-free survival (FFS) was defined as time from randomization to evidence of at least one of the following: biochemical failure; progression either locally, in lymph nodes, or in distant metastases; or death from PCa [17]. The median FFS survival in this cohort was only 11.2 months with an overall survival similar to our cohort (42 months), taking to account that they included death from PCa as one of their outcomes for FFS and therefore making it not comparable to our definition of CRPC. Hence, our dataset describes the impact of timing of metastatic disease on overall survival that is not described in any of the above-mentioned trials.
In a recent systematic review, the authors could not find a significant difference in the overall survival between men treated with abiraterone and ADT or docetaxel and ADT for castration-sensitive metastatic prostate cancer. These conclusions have to be regarded with caution, since there is currently no meta-analysis or head-to-head comparison of the two drugs in this setting [18].
Our data suggest that a higher tumor burden may correlate with earlier development of CRPC as seen in the de-novo-M group. These results are similar to others that have shown a positive effect of radical surgery or radiation in high-burden metastatic prostate cancer [19,20,21]. As most patients in our CRPC and CSPC-M groups were initially treated with curative intent, the hypothesis could be raised that a reduction in tumor burden may be beneficial for survival and prolong development of castration resistance. This would be justifiable if one would assume that all patients that developed metastases had micro-metastases at the time of surgery.
Several studies are evaluating the characteristics of patients that could benefit from a local treatment of newly diagnosed metastatic prostate cancer [22]. Our data also confirm the findings from Patrikidou et al. that a higher Gleason score and T-stage in patients with localized disease lead to a higher risk of not only dying of prostate cancer but also a higher risk for a shorter survival [11].
Due to the retrospective nature of our study there are certain limitations. Patients were not uniformly followed up after initial treatment of prostate cancer, which could impact the time to metastasis because metastasis may have been missed at an earlier stage. In addition, androgen deprivation therapy varied, including some patients receiving continuous ADT and some intermittent ADT. Specific treatments for CRPC were not available in our database; however, provincial guidelines were followed resulting in nearly all patients starting with either abiraterone or enzalutamide followed by docetaxel if they were able to tolerate it. Also imaging is not accurate in all patients with metastatic prostate cancer. Our definition of metastasis included mostly radiological evidence of metastasis, which does exclude micro-metastasis and carries the risk of missing metastasis depending on the imaging modality used. Although a vast majority of the defined metastases were bone metastases, the precise site of disease is not available either. Thus, we are unable to clearly classify patients into M-subcategory. We are aware that due to the long follow-up not all patients had the modern secondary androgen deprivation therapy available and guidelines regarding treatment of metastatic prostate cancer changed over time.
Conclusion
Our study shows that time from diagnosis to metastasis (for CRPC-M and CSPC-M patients) and time to CRPC (all patients) are significant prognosticators of overall survival. Therefore, using time to metastasis as a surrogate for current and future studies seems warranted. In addition, our data show that patients with metastasis at presentation have the worst overall survival due to the shortest time from diagnosis to CRPC. Once CRPC is reached, there is no difference in survival time between the three groups. Prolonging the development of CRPC in patients with prostate cancer seems to be the key to a longer overall survival.
References
Society AC (2016) Cancer facts & figures 2016. American Cancer Society, Atlanta
Stephenson R (2005) Prostate cancer overdiagnosis and overtreatment: analysis of US mortality and SEER incidence. Trends in the PSA and pre-PSA eras. In: Klein EA (ed) Management of prostate cancer. Humana Press, Totowa (NJ), pp 3–13
Glass TR, Tangen CM, Crawford ED, Thompson I (2003) Metastatic carcinoma of the prostate: identifying prognostic groups using recursive partitioning. J Urol 169(1):164–169. https://doi.org/10.1097/01.ju.0000042482.18153.30
Gravis G, Boher JM, Fizazi K, Joly F, Priou F, Marino P, Latorzeff I, Delva R, Krakowski I, Laguerre B, Walz J, Rolland F, Theodore C, Deplanque G, Ferrero JM, Pouessel D, Mourey L, Beuzeboc P, Zanetta S, Habibian M, Berdah JF, Dauba J, Baciuchka M, Platini C, Linassier C, Labourey JL, Machiels JP, El Kouri C, Ravaud A, Suc E, Eymard JC, Hasbini A, Bousquet G, Soulie M, Oudard S (2015) Prognostic factors for survival in noncastrate metastatic prostate cancer: validation of the glass model and development of a novel simplified prognostic model. Eur Urol 68(2):196–204. https://doi.org/10.1016/j.eururo.2014.09.022
Halabi S, Small EJ, Kantoff PW, Kattan MW, Kaplan EB, Dawson NA, Levine EG, Blumenstein BA, Vogelzang NJ (2003) Prognostic model for predicting survival in men with hormone-refractory metastatic prostate cancer. J Clin Oncol 21(7):1232–1237
Smaletz O, Scher HI, Small EJ, Verbel DA, McMillan A, Regan K, Kelly WK, Kattan MW (2002) Nomogram for overall survival of patients with progressive metastatic prostate cancer after castration. J Clin Oncol 20(19):3972–3982
Armstrong AJ, Garrett-Mayer ES, Yang YC, de Wit R, Tannock IF, Eisenberger M (2007) A contemporary prognostic nomogram for men with hormone-refractory metastatic prostate cancer: a TAX327 study analysis. Clin Cancer Res 13(21):6396–6403. https://doi.org/10.1158/1078-0432.CCR-07-1036
Safety and Efficacy Study of Enzalutamide in Patients With Nonmetastatic Castration-Resistant Prostate Cancer (PROSPER)
A Study of Apalutamide (ARN-509) in Men With Non-Metastatic Castration-Resistant Prostate Cancer (SPARTAN)
Mottet N, Bellmunt J, Briers, E, van den Bergh RCN, Bolla M, van Casteren NJ, Cornford P, Culine S, Joniau S, Lam T, Mason MD, Matveev V, van der Poel THvdK H, Rouvière O, Wiegel T (2015) Guidelines on Prostate Cancer. https://uroweb.org/guideline/prostate-cancer/. Mar 2015
Patrikidou A, Loriot Y, Eymard JC, Albiges L, Massard C, Ileana E, Di Palma M, Escudier B, Fizazi K (2014) Who dies from prostate cancer? Prostate Cancer Prostatic Dis 17(4):348–352. https://doi.org/10.1038/pcan.2014.35
Patrikidou A, Brureau L, Casenave J, Albiges L, Di Palma M, Patard JJ, Baumert H, Blanchard P, Bossi A, Kitikidou K, Massard C, Fizazi K, Blanchet P, Loriot Y (2015) Locoregional symptoms in patients with de novo metastatic prostate cancer: morbidity, management, and disease outcome. Urol Oncol 33(5):202–e209-217. https://doi.org/10.1016/j.urolonc.2015.01.022
Sweeney CJ, Chen YH, Carducci M, Liu G, Jarrard DF, Eisenberger M, Wong YN, Hahn N, Kohli M, Cooney MM, Dreicer R, Vogelzang NJ, Picus J, Shevrin D, Hussain M, Garcia JA, DiPaola RS (2015) Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med 373(8):737–746. https://doi.org/10.1056/NEJMoa1503747
James ND, Sydes MR, Clarke NW, Mason MD, Dearnaley DP, Spears MR, Ritchie AW, Parker CC, Russell JM, Attard G, de Bono J, Cross W, Jones RJ, Thalmann G, Amos C, Matheson D, Millman R, Alzouebi M, Beesley S, Birtle AJ, Brock S, Cathomas R, Chakraborti P, Chowdhury S, Cook A, Elliott T, Gale J, Gibbs S, Graham JD, Hetherington J, Hughes R, Laing R, McKinna F, McLaren DB, O’Sullivan JM, Parikh O, Peedell C, Protheroe A, Robinson AJ, Srihari N, Srinivasan R, Staffurth J, Sundar S, Tolan S, Tsang D, Wagstaff J, Parmar MK (2016) Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 387(10024):1163–1177. https://doi.org/10.1016/S0140-6736(15)01037-5
Fizazi K, Tran N, Fein L, Matsubara N, Rodriguez-Antolin A, Alekseev BY, Ozguroglu M, Ye D, Feyerabend S, Protheroe A, De Porre P, Kheoh T, Park YC, Todd MB, Chi KN, Investigators L (2017) Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med 377(4):352–360. https://doi.org/10.1056/NEJMoa1704174
James ND, de Bono JS, Spears MR, Clarke NW, Mason MD, Dearnaley DP, Ritchie AWS, Amos CL, Gilson C, Jones RJ, Matheson D, Millman R, Attard G, Chowdhury S, Cross WR, Gillessen S, Parker CC, Russell JM, Berthold DR, Brawley C, Adab F, Aung S, Birtle AJ, Bowen J, Brock S, Chakraborti P, Ferguson C, Gale J, Gray E, Hingorani M, Hoskin PJ, Lester JF, Malik ZI, McKinna F, McPhail N, Money-Kyrle J, O’Sullivan J, Parikh O, Protheroe A, Robinson A, Srihari NN, Thomas C, Wagstaff J, Wylie J, Zarkar A, Parmar MKB, Sydes MR, Investigators S (2017) Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med 377(4):338–351. https://doi.org/10.1056/NEJMoa1702900
James ND, Spears MR, Clarke NW, Dearnaley DP, De Bono JS, Gale J, Hetherington J, Hoskin PJ, Jones RJ, Laing R, Lester JF, McLaren D, Parker CC, Parmar MK, Ritchie AW, Russell JM, Strebel RT, Thalmann GN, Mason MD, Sydes MR (2015) Survival with newly diagnosed metastatic prostate cancer in the “docetaxel era”: data from 917 patients in the control arm of the STAMPEDE trial (MRC PR08, CRUK/06/019). Eur Urol 67(6):1028–1038. https://doi.org/10.1016/j.eururo.2014.09.032
Wallis CJD, Klaassen Z, Bhindi B, Goldberg H, Chandrasekar T, Farrell AM, Boorjian SA, Kulkarni GS, Karnes RJ, Satkunasivam R (2017) Comparison of abiraterone acetate and docetaxel with androgen deprivation therapy in high-risk and metastatic hormone-naive prostate cancer: a systematic review and network meta-analysis. Eur Urol. https://doi.org/10.1016/j.eururo.2017.10.002
Qin XJ, Ma CG, Ye DW, Yao XD, Zhang SL, Dai B, Zhang HL, Shen YJ, Zhu Y, Zhu YP, Shi GH, Xiao WJ, Lin GW, Swanson GP (2012) Tumor cytoreduction results in better response to androgen ablation–a preliminary report of palliative transurethral resection of the prostate in metastatic hormone sensitive prostate cancer. Urol Oncol 30(2):145–149. https://doi.org/10.1016/j.urolonc.2010.02.010
Swanson G, Thompson I, Basler J, Crawford ED (2006) Metastatic prostate cancer-does treatment of the primary tumor matter? J Urol 176(4 Pt 1):1292–1298. https://doi.org/10.1016/j.juro.2006.06.069
Culp SH, Schellhammer PF, Williams MB (2014) Might men diagnosed with metastatic prostate cancer benefit from definitive treatment of the primary tumor? A SEER-based study. Eur Urol 65(6):1058–1066. https://doi.org/10.1016/j.eururo.2013.11.012
Fossati N, Trinh QD, Sammon J, Sood A, Larcher A, Sun M, Karakiewicz P, Guazzoni G, Montorsi F, Briganti A, Menon M, Abdollah F (2015) Identifying optimal candidates for local treatment of the primary tumor among patients diagnosed with metastatic prostate cancer: a SEER-based study. Eur Urol 67(1):3–6. https://doi.org/10.1016/j.eururo.2014.08.056
Acknowledgements
Dr. Frees held a scholarship from the “Deutsche Forschungsgemeinschaft” (DFG).
Author information
Authors and Affiliations
Contributions
S. Frees Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing. S. Akamatsu Protocol/project development, Data collection or management, Manuscript writing/editing. S. Bidnur Manuscript writing/editing. D. Khalaf Data collection or management. C. Chavez-Munoz Data analysis, Manuscript writing/editing. W.Struss Data collection or management, Manuscript writing/editing. B. J Eigl Protocol/project development, Manuscript writing/editing. M. Gleave Protocol/project development, Manuscript writing/editing. K. N. Chi Protocol/project development, Manuscript writing/editing. A. I. So Protocol/project development, Data analysis, Manuscript writing/editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of human rights
For this type of study formal consent is not required.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Electronic supplementary material
Below is the link to the electronic supplementary material.
345_2018_2236_MOESM1_ESM.pdf
Supplementary material 1 (PDF 465 kb). Supplementary Fig. 2: Survival from time of metastasis. Kaplan–Meier analysis of the overall survival of patients from time of metastasis. Supplementary Fig. 3: Time from diagnosis to metastasis (CRPC-M vs CSPC-M). Kaplan–Meier analysis of the time from diagnosis to metastasis. Supplementary Fig. 4: a Pearson correlation of time from diagnosis to metastasis and time from diagnosis to death. b Pearson Correlation of time from diagnosis to CRPC and time from diagnosis to death
345_2018_2236_MOESM2_ESM.pdf
Supplementary material 2 (PDF 448 kb). Supplementary Fig. 5: Time from CRPC to death. Kaplan–Meier analysis of the overall survival of patients from time of becoming castration resistant. Supplementary Fig. 6:De- novo-M compared to all other patients divided into groups according to time to metastasis. Kaplan–Meier analysis of the overall survival of patients comparing de-novo-metastasis and groups of different time intervals of metastasis
345_2018_2236_MOESM3_ESM.pdf
Supplementary material 3 (PDF 331 kb). Supplementary Fig. 1: Schematic timeline of a typical course of patients with prostate cancer and the division used in this paper according to the time point of metastasis. Above: Initial non-metastatic prostate cancer, that is treated with an initial therapy, mostly in a curative intent, then biochemical failure which is typically treated with Androgen deprivation therapy (ADT). Patients become castration resistant followed by a secondary ADT or chemotherapy and finally ending in the death of the patient. Below: Patients with initially metastatic prostate cancer receive ADT and once becoming castration resistant chemotherapy or secondary ADT. De novo-M: Patients that presented with clinical evidence of metastasis within 3 months of initial diagnosis; CSPC-M (castration sensitive prostate cancer with metastasis): Patients who were free of metastasis initially but developed metastasis more than 6 months prior to castration resistance; CRPC-M (castration resistant prostate cancer with metastasis) patients who developed metastasis within 6 months of becoming castration resistant or after. Abbreviations: CRPC: castration resistant prostate cancer
345_2018_2236_MOESM4_ESM.docx
Supplementary material 4 (DOCX 142 kb). Supplementary Table 1: Multivariate Cox- regression: A: Prognosticators influencing OS for patients with CRPC-M and CSPC-M; B: Prognosticators influencing OS for all patients
Rights and permissions
About this article

Cite this article
Frees, S., Akamatsu, S., Bidnur, S. et al. The impact of time to metastasis on overall survival in patients with prostate cancer. World J Urol 36, 1039–1046 (2018). https://doi.org/10.1007/s00345-018-2236-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-018-2236-4