
Abstract
Objectives
Evaluation of clamp-off laser-assisted laparoscopic partial nephrectomy technique (LLPN) compared to the clamp-off laparoscopic (LPN) and open (OPN) techniques.
Patients and methods
Between September 2008 and July 2011, 36 patients suffering from small peripheral renal tumours (RT) underwent LLPN (n = 12), LPN (n = 12) and OPN (n = 12) in a prospective single-centre study. RT were excised with laser, Sonosurg or monopolar scissors during LLPN, LPN and OPN, respectively. Blood vessels are identified and sutured before opening them; alternatively, laser energy was used to coagulate them (LLPN). Early and late postoperative complications were assessed. Follow-up was done according to EAU-guidelines.
Results
Mean age was 64.9 years. Mean operative time was 135.8 min (100–180) versus 144.2 (85–255) versus 113.6 (50–170) for LLPN versus LPN versus OPN, respectively. Median estimated blood loss (EBL) was 170.8 ml (50–600) versus 245.2 (50–700) versus 425.8 (100–900) for LLPN versus LPN versus OPN, respectively. Tumours (19 right and 17 left) were located in upper (11), midparenchyma (13) and lower pole (12). Mean tumour size was 2.7 cm (1.2–5.5). There were no reported perioperative complications/conversions. There were no positive margins. Histological evaluations were not compromised in any LLPN-case. Compared to LPN, LLPN offered significant lower EBL, shorter operative time, otherwise, comparable results. Follow-up was uneventful without tumour recurrences.
Conclusion
Current prospective comparative study shows that LLPN is a reproducible efficient alternative to LPN/OPN. Besides the absence of renal ischaemia, LLPN offered lower EBL, good haemostasis and minimal parenchyma damage. Surgical and oncological outcomes are comparable to LPN and OPN.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Lasers play an active role in the current urology armamentarium in lithotripsy (Holmium) [1] and competitive role in benign prostate diseases (BPH) surgery (KTP and Holmium) [2], while further studies with enough follow-up is still missing as regard oncological indications like tumours excision and laparoscopic surgery.
Currently, there is no better way to treat small renal tumours (RT) than surgical excision. Thus, recent guidelines have urged the consideration of nephron sparing surgery (NSS) for RT up to 7 cm [3]. However, NSS should be considered whenever technically feasible and safe from the oncological point of view. While laparoscopic partial nephrectomy (LPN) has the advantage of superior postoperative recovery, it is associated with many disadvantages that have been improving over the last decade through many modifications. There are many reports documenting that this sophisticated procedures, laparoscopic and robotic-assisted, offer perioperative, functional and long-term oncological outcomes comparable to OPN [4–7]. Furthermore, a multivariate analysis showed that the surgical approach was not an independent prognosticator of survival (P = 0.06) [8]. The 5-year oncological outcomes are equivalent to those of open partial nephrectomy (OPN) [9].
Despite the mentioned advantages and the improvement in long-term outcomes, NSS remains a technically challenging procedure associated with a complication rate of 9–33% [10]. This opened a demand for laparoscopic surgical tools in order to simplify the procedure and lower this complication rates.
Haemostasis represents an important challenge during LPN. It obliged the surgeon to clamp the renal vasculature to allow for precise tumour removal in a bloodless field. The consequent warm ischaemia (WI) places a significant time constraints on the surgeon during tumour excision and parenchyma reconstruction that adds more technical challenges to the procedure [8].
Various energy sources, haemostatic devices and haemostatic agents have also gained popularity in urological laparoscopy [11]. Laser energy can offer a good cutting and coagulation tool during LPN. This was found to affect neither the feasibility of the procedure nor all its outcomes. Achieving haemostasis and collecting system closure after tumour excision, even without ischaemia, were also warranted by the procedure [12].
The aim of present study was to further simplify the procedure to decrease its complication rate. Laser was used in an attempt to precise incision and excision of RT, minimize tissue damage, ease the manipulations and add no further side effects and good haemostasis for the preservation of laparoscopic vision. This laser-assisted technique was compared prospectively to clamp-off open and laparoscopic techniques in an effort to establish a safe comparable and reproducible laser supported technique.
Patients and methods
Patients and tumour characteristics
Between September 2008 and July 2011, 36 consecutive patients (25 males and 11 females) underwent clamp-off open, laparoscopic and laser-assisted partial nephrectomy for small peripheral renal tumours in our department. Twelve patients were included in a single-centre prospective study comparing LLPN with LPN and OPN. A cross-matched group of LPN and OPN was included as control groups. All those patients underwent partial nephrectomy procedures by the same experienced surgeon (in the three approaches), and the specimens were examined by same histopathologist. All patients underwent preoperative computer tomography (CT) and/or magnetic resonance (MRI).
All tumour parameters were prospectively entered into a database by the treating surgeon. The decision not to clamp the hilum and surgical approach (i.e. transperitoneal [LPN] or retroperitoneal [RPN]) is made prospectively and is based on tumour location and proximity to the renal sinus or collecting system [13]. All patients have the same tumour parenchymal infiltration depth.
Approach
The kidney was approached through three trocars that were inserted after establishment of the retroperitoneal space at the tip of last rib, in anterior axillary line (2–3 cm above and medial to anterior superior iliac spine), and at middle point of a line connecting both ports for RPN while at 3 cm above and cranial to the umbilicus, in the midclavicular line (2 and 12 cm from thorax cage) for LPN. OPN was done through 10 cm supra-costal incision in flank lateral patient position.
Laser equipments
Diode laser apparatus (1,318 nm; Eraser, Rolle&Rolle, Salzburg, Austria) was assembled at the tableside. The sterile flat cut-ended laser fibre (core-diameter 600 μm) was fixed at the sister table and prepared through the fibre guidance instrument. This is commercially available as laser guidance instrument for Endonasal surgery (Karl Storz, Tuttlingen, Germany) during LLPN [14]. Laser adjustment between 45 and 70 W in a moderate cut velocity (1–3 mm/s) and continuous wave (CW) mode was sufficient for adequate manipulations (cutting as well as preparation).
Technique
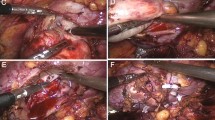
The laser-assisted technique without ischaemia and its intraoperative challenges were reported [14]. After incision of geroata’s fascia and preparation of renal hilum, the perirenal fat is removed from upper, lower or middle parts of the kidney for adequate tumour exposition. The fibre guidance system was introduced through 10 mm trocar positioned as near as possible to the kidney as a protection sheath. Laparoscopic suction device was hold simultaneously in left hand. Renal tumour was excised using the laser energy with an adequate free resection edges (RR) and depicted in the laparoscopic entrapment sack. This sack is moved over the liver or spleen (LPN) or toward the pelvis (RPN), and its drawstick is fixed externally. The tumour extraction followed through the camera port incision. The renal cut surface was then biopsied and coagulated using the diode laser (without tissue contact). If needed, opened vessels were compressed until the tumour is resected wide enough to avoid laser effects on the sutures after reconstruction (done only once). Opened calyx or large vessels were sutured with 3–0 monocryl. The renal parenchyma was covered with cellulose mesh and closed using 0–0 Vicryl sutures maintaining adequate compression. After removal of the specimen, a drain was placed through the 5-mm port site with closure of the other sites.
Some intraoperative manoeuvres during OPN/LPN without clamping of the renal vessels are used. The tumour was slowly resected with Sonosurg during conventional LPN. During this resection, the vessels and calyx system were identified and controlled with 4–0 Vicryl needles before opening them. Accidentally opened blood vessels were compressed with small laparoscopic gauze, brought previously to the field, till they were sutured. After that the parenchyma cut surface is compressed with this gauze tell further bleeding vessels are sutured and the renal parenchyma is then covered with cellulose mesh and closed using 0–0 Vicryl continuous sutures. The same principles are applied during OPN. Resection was done by monopolar scalpel, and manual compression of the kidney was used if vessels were accidently opened. There was no need for additional haemostatic materials in all cases. No patient became clinically unstable.
The drainage tubes and urethral catheters were removed on second and third postoperative day, respectively.
All specimens were measured and fixed in formalin for histological examination to evaluate the depth and effects of laser on RR.
Postoperative managements and follow-up
Postoperative complications were assessed till discharge and included in the prospective database. At the time of analysis, a retrospective review of each patient’s electronic medical records was performed to assess for the late complications. Follow-up over 2–29 months was done according to the standard guidelines.
Statistics
For comparison of variables between different patient groups, the Mann–Whitney U test was used. P values below 0.05 were regarded as significant. All calculations were performed using software STATISTICA (release 8, StatSoft Inc., Tulsa, OK, USA).
Results
The described techniques were applied successfully to all patients. The median age of all treated patients was 63.0 years (39–88). Tumours (19 right and 17 left sides) were distributed as follows: 11 in the upper pole, 13 in midparenchyma part and 12 in lower pole. The median (range) tumour size was 2.6 cm (1.2–5.5). The median (range) operative time was 132.5 min (100–180) versus 123 (85–255) versus 100 (50–170) for LLPN versus LPN versus OPN, respectively. The median (range) estimated blood loss (EBL) was 170.8 ml (50–600) versus 254.2 (50–700) versus 425 (100–900) for LLPN versus LPN versus OPN, respectively. We have had no instances of severe intra-operative or delayed postoperative complications (e.g. severe bleeding), emergency clamping of renal vessels or conversions to open surgery. No patients received blood transfusions perioperatively. One LLPN patient received a delayed transfusion on 5th postoperative day (POD) because of serum haemoglobin of 8.9 mg/dl, but this was not due to bleeding from the procedure. This patient had an acquired immune deficiency syndrome (AIDS) with high virus load, neutropenia and was transfused as a precaution rather than a postoperative necessity. Notably, an abdominal-CT scan done in the 4th POD showed no evidence of para-renal haematoma or extravasations.
In this consecutive comparative series of 36 patients, the median (range) postoperative fall in the serum haemoglobin was 2.2 gm/dl (0.2–5.3) with a median (range) serum haemoglobin at discharge of 11.0 gm/dl (7.5–15.3). The median (range) preoperative creatinine was 1.7 mg/dl (0.6–3.6), and the median (range) postoperative creatinine at discharge was 1.6 mg/dl (0.7–3.8). There were no cases of urine leakage.
There were no positive margins at intraoperative frozen sections. However, it should be noted that the surgeon has re-resected the renal parenchyma at the tumour bed in two cases, at the beginning of the LLPN series, because of macroscopically unclear surgical margin. Specimens were found free of tumour microscopically by the pathologist. The evaluation of the surgical margin was not compromised in any case by the use of monopolar, laser or sonosurg devices. The histopathology included: 19 clear-cell cancers, six papillary renal cell cancers, one chromophobe renal cell cancer, four oncocytomas, four angiomyolipoma, one metastatic tumour (bronchial carcinoma) and one leiomyoma.
There was no difference in the postoperative hospital stay or the need of postoperative analgesics between the patients groups. Summery of the demographic, operative and perioperative parameters of the three groups is shown in Tables 1 and 2. There was a significant lower EBL (P = 0.016) and shorter operative time (insignificant, P = 0.644) for LLPN versus LPN, respectively. Otherwise, all other parameters were comparable with LPN. Further, there was no significant difference between LPN and RPN in all examined parameters. Both laparoscopic techniques (LLPN and LPN) have significant lower blood loss (P < 0.005), insignificant lower serum CRPs level as well as insignificantly longer operative time than OPN. One LLPN patient developed a para-nephric abscess necessitating puncture after one postoperative month. Tumour excision time was 9–17 min for LLPN versus 7–15 min for LPN versus 5–11 min for OPN, respectively, without any significance between groups. LLPN offered an advantage as regard the easy manipulations, good cutting and haemostatic laser characters.
On follow-up CT, no patients had evidence of local recurrence in the resection bed, para-renal haematoma or urine extravasations. The mean follow-up for these patients was 14.8 (2–29) months.
Discussion
While technical improvements in open surgery are hardly possible with its current high standards, minimal invasive surgeries remain continuously in progress. There is no widely accepted and established LPN method. Many aspects are contributing in making LPN technique challenging. Avoidance of severe blood loss, precise excision of RT and saving the collecting system together with minimal parenchymal damage in order to preserve the renal function are the main principles. However, the complication rate was reported to be 33%, from which 5.5% was stated to occur intraoperatively, 12% postoperatively, and 15.5% were delayed complications [15]. Therefore, a new modality of RT resection is still required.
The feasibility of the described LLPN technique was reported previously. The laser irrigation system for adequate laser manipulations, laser cutting and coagulation quality, microscopic depth of laser coagulation in tissue and management of intraoperative challenges were also reported [12, 14]. In current work, it was intended to prospectively compare the results of clamp-off LLPN with LPN and OPN in a single surgeon/centre series omitting the effect of surgeon experience or learning curve on the acquired results. Further the same pathologist had assessed all the specimens.
An important advantage of the described techniques is the avoidance of WI. The safe limit of WI during LPN remains controversial, but every attempt should be made to avoid or keep WI at a minimum to limit the permanent kidney damage. Further, increasing WI was reported as an independent predictor for postoperative complications after LPN [16]. Another advantage was the significantly lower EBL for LLPN versus the standard OPN and LPN.
As mentioned, some laser technologies have become established standard modalities available for urological clinical applications, while others are still under investigation. Recently, various laser systems have been used for NSS in animal models [1–19] and in vivo [20, 21]. However, none of these techniques has proved widespread use for this surgery. Thus, we evaluated the 1,318 nm diode laser through end-firing laser fibre for the resection of renal tissue.
Every laser has its efficacy in cutting/coagulation according to its tissue absorption characters. The diode laser has been introduced for the treatment of BPH. Its strong absorption by water at a wavelength of 1,470 nm allows tissue penetration of 2–3 mm [22]. Other diode laser systems working on a wavelength of 1,380 nm offer the highest simultaneous absorption in water and haemoglobin. Therefore, it is thought that this diode laser is able to combine high tissue ablation properties with the benefit of excellent haemostasis. The used laser with its wavelength was suitable for LPN as it combines good cutting and coagulation qualities [12]. This was found to affect neither the macroscopic nor microscopic view of the tumours which is important for the oncological outcomes of LLPN [14].
Louei et al. [11] reported a selected review of the worldwide literature from 2000 to 2009 (n = 1,286 patients). They found that haemorrhage was the most common complication (6.6%, mean EBL of 366 ml) followed by urinary extravasations (3.1%) as the second most common. Transfusion rate was 7.6%. Most of these procedures were done with laparoscopic scissors rather with an energy-based sealing device. These case series showed the results of the pioneer laparoscopic surgeons at the beginning of their LPN experience. The major aim of current series was to create a simple surgical technique to control intraoperative bleeding during tumour resection without ischaemia. LLPN seems to fulfil this primary goal without need for any further haemostatic materials or steps that is time saving and cost-effective. Further, the technique was also feasible with comparable outcomes through the retroperitoneoscopic approach.
Another goal was to create a reproducible technique to be accessible for urological surgeons at any point of their learning curve with LPN. The described simple manoeuvres including laser device provides a very simple way of tumour excision without ischaemia assuring adequate haemostasis and without affecting the oncological results or closure of collecting system. This makes the technique reproducible and more available to urologists. The current results are also comparable with literature [4–7]. Being comparable to the conventional techniques argues in favour of LLPN and laser energy which had proved efficacy in current series. LLPN offers further advantage over LPN that the laser fibre is easy to manipulate (than Sonosurg) under complete surgeon control.
Lastly, technical problems concerning laser adjustments, handling of laser fibre and optimal speed of cutting/coagulation are of outmost importance for the emerging technique. Based on our ex vivo and in vivo experience, these manoeuvres are easy to learn with a short learning curve. The safety of the technique should be warranted, so we advice the presence of laser physics specialist at the beginning of first experience with LLPN.
There are some limitations of this study. Small patient number but, to our knowledge, this is the largest series of LLPN to date. Additionally, the current experience was over a period of several years, without ischaemia and for tumours as large as 5.5 cm, and no bleeding, conversions or urine leakage has occurred. This argues, from our point of view, in favour of this technique. Further, the necessity of special training for laser makes the technique only available for clinics where this technology is available.
Lastly, the laser equipments need more adaptation to the laparoscopic techniques which we have already begun [23].
Conclusion
This prospective comparative study shows that LLPN is a reproducible and efficient technique for LPN. It offers the advantage of less blood loss, good haemostasis and minimal parenchymal damage. Its surgical and oncological outcomes are comparable to OPN and LPN.
References
Pierre S, Preminger GM (2007) Holmium laser for stone management. World J Urol 25:235–239
Descazeaud A, Robert G, Azzousi AR, Ballereau C, Lukacs B, Haillot O, Dumonceau O, Devonec M, Fourmarier M, Saussine C, de la Taille A (2009) Committee for lower urinary tract symptoms of the French Association of Urology. Laser treatment of benign prostatic hyperplasia in patients on oral anticoagulant therapy: a review. BJU Int 103:1162–1165
Campbell SC, Novick AC, Belldegrun A et al (2009) Guideline for management of the clinical T1 renal mass. J Urol 182:1271–1279
Lane BR, Gill IS (2007) 5-Year outcomes of laparoscopic partial nephrectomy. J Urol 177:70
Allaf ME, Bhayani SB, Rogers C et al (2004) Laparoscopic partial nephrectomy: evaluation of long-term oncological outcome. J Urol 172:871
Jeong W, Park SY, Lorenzo EI, Oh CK, Han WK, Rha KH (2009) Laparoscopic partial nephrectomy versus robot-assisted laparoscopic partial nephrectomy. J Endourol 23:1457–1460
Williams SB, Kacker R, Alemozaffar M, Francisco IS, Mechaber J, Wagner AA (2011) Robotic partial nephrectomy versus laparoscopic partial nephrectomy: a single laparoscopic trained surgeon’s experience in the development of a robotic partial nephrectomy program. World J Urol [Epub ahead of print]
Lane BR, Gill IS (2010) 7-year oncological outcomes after laparoscopic and open partial nephrectomy. J Urol 183:473–479
Porpiglia F, Volpe A, Billia M, Scarpa RM (2008) Laparoscopic versus open partial nephrectomy: analysis of current literature. Eur Urol 53:732–743
Wheat JC, Roberts WW, Hollenbeck BK, Wolf JS Jr, Weizer AZ (2011) Complications of laparoscopic partial nephrectomy. Urol Oncol 28 [Epub ahead of print]
Louie MK, Deane LA, Kaplan AG, Lee HJ, Box GN, Abraham JB, Borin JF, Khan F, McDougall EM, Clayman RV (2011) Laparoscopic partial nephrectomy: six degrees of haemostasis. BJU Int 107:1454–1459
Khoder WY, Sroka R, Hennig G, Seitz M, Siegert S, Zillinberg K, Gratzke C, Stief CG, Becker AJ (2011) The 1,318-nm diode laser supported partial nephrectomy in laparoscopic and open surgery: preliminary results of a prospective feasibility study. Lasers Med Sci 26:689–697
Weizer AZ, Gilbert SM, Roberts WW et al (2008) Tailoring technique of laparoscopic partial nephrectomy to tumor characteristics. J Urol 180:1273–1278
Khoder WY, Sroka R, Kellhammer N, Haseke N, Stief CG, Becker AJ (2011) Laser-assisted laparoscopic partial nephrectomy without ischemia: procedure and challenges. J Endourol Part B Videourol. doi:10.1089/vid.2010.0155
Ramani AP, Desai MM, Steinberg AP, Ng CS, Abreu SC, Kaouk JH, Finelli A, Novick AC, Gill IS (2005) Complications of laparoscopic partial nephrectomy in 200 cases. J Urol 173:43–47
Turna B, Frota R, Kamoi K et al (2008) Risk factor analysis of postoperative complications in laparoscopic partial nephrectomy. J Urol 179:1289–1295
Eret V, Hora M, Sykora R, Hes O, Urge T, Klecka J, Matejovic M (2009) GreenLight (532 nm) laser partial nephrectomy followed by suturing of collecting system without renal hilar clamping in porcine model. Urology 73:1115–1118
Bui MH, Breda A, Gui D, Said J, Schulam P (2007) Less and minimal tissue carbonization using a thulium laser for laparoscopic partial nephrectomy without hilar clamping in a porcine model. J Endourol 21:1107–1111
Anderson JK, Baker MR, Lindberg G, Cadeddu JA (2007) Large-volume laparoscopic partial nephrectomy using the potassium-titanyl-phosphate (KTP) laser in a survival porcine model. Eur Urol 51:749–754
Gruschwitz T, Stein R, Schubert J, Wunderlich H (2008) Laser-supported partial nephrectomy for renal cell carcinoma. Urology 71:334–336
Mattioli S, Muñoz R, Recasens R, Berbegal C, Teichmann H (2008) What does Revolix laser contribute to partial nephrectomy. Arch Esp Urol 61:1126–1129
Seitz M, Sroka R, Gratzke C, Schlenker B, Steinbrecher V, Khoder W, Tilki D, Bachmann A, Stief C, Reich O (2007) The diode laser: a novel side-firing approach for laser vaporisation of the human prostate—immediate efficacy and 1-year follow-up. Eur Urol 52:1717–1722
Khoder WY, Seroka R (2011) Concept of a fiber guidance instrument for laser-assisted laparascopic partial nephrectomy. Med Laser Appl 26:176–182
Acknowledgments
The authors would like to thank the Rolle&Rolle Company, Austria for their support during this study.
Conflict of interest
I disclose any commercial association that might pose a conflict in connection with my submitted article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Khoder, W.Y., Sroka, R., Siegert, S. et al. Outcome of laser-assisted laparoscopic partial nephrectomy without ischaemia for peripheral renal tumours. World J Urol 30, 633–638 (2012). https://doi.org/10.1007/s00345-011-0807-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-011-0807-8