
Abstract
Objectives
To examine radiation dose levels of CT-guided interventional procedures of chest, abdomen, spine and extremities on different CT-scanner generations at a large multicentre institute.
Materials and methods
1,219 CT-guided interventional biopsies of different organ regions ((A) abdomen (n=516), (B) chest (n=528), (C) spine (n=134) and (D) extremities (n=41)) on different CT-scanners ((I) SOMATOM-Definition-AS+, (II) Volume-Zoom, (III) Emotion6) were included from 2013–2016. Important CT-parameters and standard dose-descriptors were retrospectively examined. Additionally, effective dose and organ doses were calculated using Monte-Carlo simulation, following ICRP103.
Results
Overall, radiation doses for CT interventions are highly dependent on CT-scanner generation: the newer the CT scanner, the lower the radiation dose imparted to patients. Mean effective doses for each of four procedures on available scanners are: (A) (I) 9.3mSv versus (II) 13.9mSv (B) (I) 7.3mSv versus (III) 11.4mSv (C) (I) 6.3mSv versus (II) 7.4mSv (D) (I) 4.3mSv versus (II) 10.8mSv. Standard dose descriptors [standard deviation (SD); CT dose indexvol (CTDIvol); dose-length product (DLPbody); size-specific dose estimate (SSDE)] were also compared.
Conclusion
Effective dose, organ doses and SSDE for various CT-guided interventional biopsies on different CT-scanner generations following recommendations of the ICRP103 are provided. New CT-scanner generations involve markedly lower radiation doses versus older devices.
Key Points
• Effective dose, organ dose and SSDE are provided for CT-guided interventional examinations.
• These data allow identifying organs at risk of higher radiation dose.
• Detailed knowledge of radiation dose may contribute to a better individual risk-stratification.
• New CT-scanner generations involve markedly lower radiation doses compared to older devices.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The definite diagnosis of cancer often requires a histological examination of a cell or tissue sample obtained by biopsy, operation, ultrasound or CT-guided interventional procedure. With the recent progress in targeted therapies, CT-guided interventional biopsies significantly gain relevance in the diagnostics for personalized medicine [1, 2]. Despite the advances in radiomics technology [3, 4], until now, only by obtaining tumour tissue is it possible to integrate the molecular profiling of somatic mutation into patient therapy and care. Due to the possible technical complexity, a CT-guided interventional procedure requires close team-work of radiologists and technologists and may involve high radiation doses. At the same time as the number of diagnostic imaging examinations is increasing, anxiety about radiation exposure raises [5, 6]. Several studies examined radiation dose levels of CT-guided interventions, comparing different CT-guided interventional procedures such as cryoablation, aspiration, biopsy, drain or injection [7, 8]. As a primary dose descriptor, the dose length product was regularly applied [8]. However, in contrast to this traditional dose descriptor, the size-specific dose estimate (SSDE) and effective dose became widely established as a recognized method to quantify patient dose giving a far more accurate picture of radiation exposure [9, 10]. Up to now, no study has been conducted that compared SSDE, effective dose and individual organ doses of CT-guided biopsies on different CT devices, although in the last decade new CT technologies have emerged. Hence, the purpose of this study was to examine radiation dose of CT-guided interventional biopsies on different CT-scanner generations calculated following the recommendations of the International Commission on Radiological Protection ICRP 103 [11]. In detail, the study aimed at the following objectives: (i) Assessment of SSDE and individual organ doses imparted to patients undergoing of CT-guided interventional procedures at a large multisite institute, (ii) differentiation of radiation doses according to CT-scanner device and to organ region, (iii) determination of age-, gender- and size-based effective doses for CT-guided interventions.
Methods
The Institutional Review Board gave ethical approval (17-7679-BO) and waived the requirement for informed consent. In a retrospective study design in total 1,219 consecutive CT-guided interventional biopsies were included in the time period from January 2013 to December 2016. Differentiation of procedures was made according to four different organ regions: (A) abdomen (n = 516), (B) chest (n = 528), (C) spine (n = 134) and (D) extremities (n = 41). CT-guided interventional procedures were performed on three different, single-source CT-scanner generations (I) SOMATOM Definition AS+, (II) Somatom Volume Zoom and (III) Emotion 6 (all Siemens Healthcare, Forchheim, Germany). The SOMATOM Volume Zoom is the oldest generation of CT-scanners, followed by the Emotion 6 and then by the more recent SOMATOM Definition AS+. SOMATOM Volume Zoom CT-scanner is a four-multislice CT-scanner and has both fore and aft collimators. Emotion 6 is a low power, six-slice CT-scanner. SOMATOM Definition AS+ is a 64-slice CT-scanner that employs the flying focal spot to mimic 128-slice operation with a 64-slice detector array. At our institute not all interventional procedures were examined on all CT scanners due to local and organization terms: on SOMATOM Definition AS+ all organ regions were examined, on Somatom Volume Zoom all but chest and on Emotion 6 chest only. Therefore, for interventional procedures of the (A) abdomen, (C) spine and (D) extremities radiation doses were compared between (I) SOMATOM Definition AS+ and (II) SOMATOM Volume Zoom and those of (B) chest between (I) SOMATOM Definition AS+ and (III) Emotion 6.
CT-guided interventional procedure
According to the clinical guidelines at our institute all examinations were conducted after determining strict clinical indication, exclusion of contraindications and interdisciplinary consent. Every CT-guided interventional procedure included an initial planning CT-scan in helical modus with the purpose of adjusting the optimal table and patient position for an interventional access. Depending on the complexity of the procedure, several sequential series were acquired during the whole intervention in order to achieve a secure, coaxial biopsy of a lesion. An additional enhanced or non-enhanced control CT-scan was conducted after completion to exclude possible complications such as pneumothorax or bleeding. Technical parameters of the CT-guided interventions are summarised in detail in Table 1.
Calculation of radiation exposure
Radiation exposure was determined by the dose-monitoring software Radimetrics Enterprise Platform [12,13,14]. The calculation of the effective dose relies on a Monte Carlo simulation engine following the recommendations of the ICRP 103 [11]. The software incorporates a library of various phantoms based on the Cristy phantom library. Several variables like gender, age or water-equivalent diameter (WED) are used to define which virtual phantom will apply for an individual patient. The dose-calculation algorithm takes z-overscanning by broader beam collimation into account.
In addition, the standard deviation (SD), size-specific dose estimates (SSDEs) and important CT-parameters (reference tube voltage (kV), reference tube current (mAs), slice thickness (mm), collimation, pitch, average number of series and average number of images per procedure as well as standard dose descriptors like computed tomography dose index (CTDIvol) and dose length product (DLP) were examined.
Statistical analysis
Statistical analysis was performed with SPSS Statistics® version 21.0 (SPSS, Chicago, IL, USA). Descriptive statistics, Pearson’s correlation and the Mann-Whitney U test were used to test the differences in radiation exposure of the different subgroups. The level of significance was set at a p-value less than 0.05.
Results
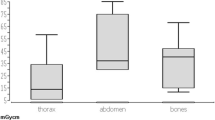
Altogether 516 interventional procedures of the abdomen (A), 528 interventional procedures of the chest (B), 134 interventions of the spine (C) and 41 interventions of the extremities (D) were included in the study. During abdomen interventions (A) average effective dose was 20 % higher compared to chest interventions (B), 30 % higher compared to spine interventions (C) and 50 % higher compared to procedures of the extremities (D). Statistical analysis of radiation doses with the Mann-Whitney U test revealed that there was a highly significant difference in radiation doses concerning CT-scanner generation at the p < 0.001 level. The mean effective dose and selected dose metrics [standard deviation; CTDIvol; DLP; SSDE] for each of the four procedures are summarised as follows: (A) (I) 9.3 mSv [3.8 mSv; 10.8 mGy; 655 mGy*cm; SSDE 12.2 mGy]; (II) 13.9 mSv [4.8 mSv; 13.3 mGy; 813 mGy*cm; SSDE 13.2 mGy] (dose distribution highlighted in Fig. 1); (B) (I) 7.3 mSv [3.5 mSv; 7.8 mGy; 440 mGy*cm; SSDE 8.8 mGy]; (III) 11.4 mSv [3.7 mSv; 9.5 mGy; 684 mGy*cm; SSDE 11.9 mGy]; (C) (I) 6.3 mSv [2.5 mSv; 13.3 mGy; 460 mGy*cm; SSDE 14.4 mGy]; (II) 7.4 mSv [2.5 mSv; 14.4 mGy; 620 mGy*cm; SSDE 13.2 mGy]; (D) (I) 4.3 mSv [3.1 mSv; 9.1 mGy; 257 mGy*cm; SSDE 10.1 mGy]; (II) 10.8 mSv [4.7 mSv; 14.7 mGy; 777 mGy*cm; SSDE 12.8 mGy]. Figure 2 demonstrates the mean effective dose according to CT-scanner device and organ region. The lowest radiation dose was achieved with the 128-multislice CT-scanner Somatom Definition AS+ (I). Tables 2, 3, 4 and 5 depict effective dose differentiated according to patient age, WED and gender. Figures 3a–b display effective dose and individual organ doses for chest and abdominal CT-guided interventional procedures on different CT-scanner generations. Statistical analysis showed a positive linear correlation between number of images and effective dose (p < 0.001; Pearson's correlation coefficient 0.28), and the number of series and effective dose (p < 0.001; Pearson's correlation coefficient 0.33). There was no significant correlation between procedure time and radiation exposure (p > 0.05).

Scatter plot delineating dose distribution (in terms of effective dose; ICRP 103) of CT-guided interventional procedures for the abdomen on (I) 128-mulitslice CT-scanner SOMATOM Definition AS+, and on (II) four-mulitslice CT-scanner SOMATOM Definition Volume Zoom (both Siemens Healthcare, Forchheim, Germany)

In this bar chart the mean effective dose (following recommendations of the ICRP 103; in mSv) is delineated on (I) SOMATOM Definition AS+ and (III) Emotion 6 for CT-guided interventions of the (B) chest (n = 528). For interventional procedures of the (A) abdomen (n = 516), (C) spine (n = 134) and (D) extremities (n = 41) radiation doses are delineated on (I) SOMATOM Definition AS+ and (II) SOMATOM Definition Volume Zoom (all Siemens Healthcare, Forchheim, Germany)

Highlighting effective dose and individual organ doses (in mSv) imparted to patients during CT-guided interventional procedures in (a) the abdominal area on SOMATOM Definition Volume Zoom (blue) and SOMATOM Definition AS+ (red), and (b) the thoracic area on Emotion 6 (blue) and SOMATOM Definition AS+ (red)
Discussion
The clinical question of concern was to determine radiation exposure, in particular the effective dose, individual organ doses and SSDE, imparted to patients undergoing CT-guided interventional biopsies on different CT-scanner generations at a large multisite institute. The present data contribute to the examination of age-, gender- and size-based dose reference levels. Previously reported dose reference levels give only a general, unisex dose reference such as DLPbody or CTDIvol and focus on standard diagnostic CT-procedures [7, 8, 15]. Furthermore, this study was intended to evaluate radiation exposure of three different CT-scanner generations and their impact on radiation dose of CT-guided interventions. At the very beginning of the decade of multislice CT-scanners there were great doubts whether effective doses were much higher, and about its geometric efficiency. Especially effects of overbeaming and overscanning in helical scanning posed a matter of concern [16], particularly for CT-scans with short scan lengths such as in CT-guided interventional biopsies. However, the present data show that new CT-scanner generations bear considerable capacity for radiation dose savings. In fact, the lowest radiation dose was achieved at the CT-scanner with the highest slice capabilities i.e. 128-multislice. During CT-scans on (I) SOMATOM Definition AS+ tube voltage adjustment (CARE kV), automatic tube current modulation (CARE Dose4D) and iterative reconstruction SAFIRE (Sinogram Affirmed Iterative Reconstruction) were applied. Automatic tube current modulation (CARE Dose) was the leading dose technology on (II) SOMATOM Volume Zoom. (III) Emotion 6 included automatic tube current modulation (CARE Dose4D) and iterative reconstruction IRIS (Iterative Reconstruction in Image Space). Automatic tube current modulation can be performed using one or more of three basic approaches, patient-size, z-axis and angular dose modulation. Contrary to CARE Dose, which is based on angular dose modulation only, CARE Dose4D involves a weight-based, angular and z-axis dose modulation.
The present results are in line with previous studies that showed a wide variation of examined local diagnostic reference levels in terms of the dose length product. The estimated organ doses for CT-guided interventional procedures are less or equal compared to previously published organ doses for standard diagnostic CT-protocols on a 320-multislice CT-scanner [17]. Radiation dose is influenced by many key factors of a technical, human-made or external nature. Nonetheless, the present data underline the continuous trend of lowering radiation doses compared to older CT-scanner devices. This may be due to enhanced capabilities and extended applications of newer CT-scanner generations (iterative reconstruction, automatic dose modulation, high pitch technique [18], etc.). Leng et al. found that the mean DLPbody of a collection of CT-guided interventional procedures (cryoablation, aspiration, biopsy, drain) ranged from 909 mGy*cm (for biopsy) to 7,946 mGy*cm (for cryoablation) at 16-, 40- and 64-multislice CT-scanners [7]. Kloeckner et al. discussed preliminary dose reference levels for various intervention types on a four-multislice CT-scanner. They showed that the mean DLPbody for a liver biopsy was 848 mGy*cm and for a retroperitoneal biopsy 889 mGy*cm [8], about 23–27 % higher compared to the present results, which indicate that the mean DLPbody for a standardised abdominal intervention is 655 mGy*cm at a 128-multislice CT-scanner.
Former studies focused predominantly on traditional dose descriptors (CTDIvol and DLPbody), which neglect patients’ characteristics and body composition [19]. Contrary to former studies, in the present study the estimate of patient dose was determined primarily in terms of effective dose, individual organ doses and size-specific dose estimate (SSDE). Overall, the effective dose distinguised according to patient age and gender showed notable variation. As expected, larger patients with higher water equivalent diameter (WED) were imparted to higher radiation doses. A major strength of the present study is the large data collection representing a wide clinical patient collective that avoids systematic bias. Data acquisition was performed with the help of a Monte Carlo simulation engine, which in preceding studies proved to be a valid tool for dose calculation [12,13,14].
The limitations of the study are those characteristics of methodical design that result from the total uncertainty of MC simulation results, estimated to be 5–10 % [14]. In future studies it will be necessary to consider data from other institutes and data with scanners from other venders.
Conclusion
The present study provides effective dose, individual organ doses and SSDE during various CT-guided interventional procedures at different CT-scanner generations following recommendations of the ICRP 103. Dose reduction potential of examined organ regions highly depends on the applied CT-scanner generation. New CT-scanner generations involved markedly lower radiation doses compared to older devices and thus, may considerable reduce overall radiation exposure.
Abbreviations
- CARE®:
-
Combined Applications to Reduce Exposure
- CT:
-
Computed tomography
- CTDIvol :
-
CT dose indexvol
- DLPbody :
-
Dose-length product
- ICRP:
-
International Commission on Radiological Protection
- kV:
-
Kilovolt (tube voltage)
- mAs:
-
Milliampere second (tube current–time product)
- Safire®:
-
Sinogram-affirmed iterative reconstruction
- SD:
-
Standard deviation
- SSDE:
-
Size-specific dose estimate
- WED:
-
Water equivalent diameter
References
Tsai IC, Tsai WL, Chen MC et al (2009) CT-guided core biopsy of lung lesions: a primer. Am J Roentgenol 193:1228–1235
Pao W, Kris MG, Iafrate AJ et al (2009) Integration of molecular profiling into the lung cancer clinic. Clin Cancer Res 15:5317–5322
Gevaert O, Xu J, Hoang CD et al (2012) Non-small cell lung cancer: identifying prognostic imaging biomarkers by leveraging public gene expression microarray data — methods and preliminary results. Radiology. 264:387–396
Aerts HJ, Velazquez ER, Leijenaar RT et al (2014) Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat Commun 5:4006
Pearce MS, Salotti JA, Little MP et al (2012) Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet 380:499–505
Brenner DJ, Hall EJ (2007) Computed tomography — an increasing source of radiation exposure. N Engl J Med. 357:2277–2284
Leng S, Christner JA, Carlson SK et al (2011) Radiation Dose Levels for Interventional CT Procedures. AJR Am J Roentgenol. 197:W97–W103
Kloeckner R, dos Santos DP, Schneider J, Kara L, Dueber C, Pitton MB (2013) Radiation exposure in CT-guided interventions. Eur J Radiol. 82:2253–2257
McCollough CH, Leng S, Lifeng Y, Cody DD, Boone JM, McNitt-Gray MF (2011) CT dose index and patient dose: they are not the same thing. Radiology 259:311–316
Brink JA, Morin RL (2012) Size-specific dose estimation for CT: how should it be used and what does it mean? Radiology 265:666–668
ICRP Publication 103 (2007) Recommendations of the International Commission on Radiological Protection. Annals of the ICRP Vol. 37 (2-4). Elsevier Science, Oxford
Guberina N, Forsting M, Suntharalingam S et al (2017) Radiation dose monitoring in the clinical routine. Rofo 189:356–360
Guberina N, Suntharalingam S, Naßenstein, Forsting M, Theysohn J, Wetter A K et al (2017) Verification of organ doses calculated by a dose monitoring software tool based on Monte Carlo Simulation in thoracic CT protocols. Acta Radiol. https://doi.org/10.1177/0284185117716199
Guberina N, Suntharalingam S, Naßenstein K et al (2016) Clinical evaluation of a dose monitoring software tool based on Monte Carlo Simulation in assessment of eye lens doses for cranial CT scans. Neuroradiology. 58:955-959.
Kanal KM, Butler PF, Sengupta D, Bhargavan-Chatfield M, Coombs LP, Morin RL (2017) U.S. diagnostic reference levels and achievable doses for 10 adult CT examinations. Radiology. https://doi.org/10.1148/radiol.2017161911
Tzedakis A, Damilakis J, Perisinakis K, Karantanas A, Karabekios S, Gourtsoyiannis N (2007) Influence of z overscanning on normalized effective doses calculated for pediatric patients undergoing multidetector CT examinations. Med Phys 34:1163–1175
Sinclair L, Griglock TM, Mench A (2015) Determining organ doses from ct with direct measurements in postmortem subjects: part 2--correlations with patient-specific parameters. Radiology. 277:471–476
Guberina N, Lechel U, Forsting M, Ringelstein A (2016) Efficacy of high-pitch CT protocols for radiation dose reduction. J Radiol Prot 36:N57–N66
Menke J (2005) Comparison of different body size parameters for individual dose adaptation in body CT of adults. Radiology 236:565–571
Funding
The authors state that this work has not received any funding.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Dr.med. Guberina.
Conflict of interest
The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article.
Statistics and biometry
One of the authors has significant statistical expertise.
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was waived by the Institutional Review Board.
Ethical approval
Institutional Review Board approval was obtained.
Methodology
• prospective / retrospective
• observational
• multicentre study
Rights and permissions
About this article

Cite this article
Guberina, N., Forsting, M., Ringelstein, A. et al. Radiation exposure during CT-guided biopsies: recent CT machines provide markedly lower doses. Eur Radiol 28, 3929–3935 (2018). https://doi.org/10.1007/s00330-018-5350-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-018-5350-1