
Abstract
Objectives
To investigate the changes of respiratory function in patients affected by chronic obstructive pulmonary disease (COPD) with single dorsal osteoporotic vertebral compression fractures (OVCFs) treated with vertebroplasty (VTP).
Methods
Forty-five patients affected by COPD and single dorsal OVCF underwent VTP (29 men, 16 women; mean age 71.4 years, range 65–77 years). Inclusion criteria were magnetic resonance findings of bone marrow oedema, without intracanal bone fragments and refractory pain to medical treatment for at least 3 months. Osteoporosis was assessed by bone densitometry. Spirometry was performed before and after treatment.
Results
A significant VAS-score decrease was observed 1 week after VTP, with a subsequent decrease over time; vital capacity (VC) and forced vital capacity (FVC) improved over time, reaching a plateau at 3 months. Forced expiratory volume at 1 s (FEV1) did not significantly differ between the pre-VTP values and follow-up values. A significant correlation was observed between VAS-score values and VC, and VAS-score values and FVC. No significant correlation was observed between VAS-score values and FEV1 values.
Conclusions
VTP improves restrictive ventilatory impairment in patients with moderate and severe COPD affected by single thoracic OVCFs. We recommend this treatment in the management of these patients.
Key Points
• Osteoporosis is a major comorbidity in chronic obstructive pulmonary disease (COPD) patients.
• Pain due to osteoporotic vertebral compression fractures worsens respiratory failure in COPD.
• Vertebroplasty improves ventilatory impairment in COPD patients with osteoporotic vertebral compression fractures.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoporosis represents a significant cause of morbidity and mortality, which is becoming increasingly prevalent with the ageing of the population [1, 2]. Vertebral compression fractures (VCFs) are the most common fractures associated to osteoporosis, although they often remain unidentified in about half of patients that do not experience pain symptoms. Due to the peculiar kinetic of the spine, 80 % of pathological vertebral fractures are located at the dorsal-lumbar passage; the most frequent sites of osteoporotic vertebral fractures are, in decreasing order, L1, D12 and L2 [3]. VCFs usually cause back pain, more or less intense depending on the site and number of the fractures and their severity, which may affect the patients’ quality of life. Other consequences of VCFs are represented by spinal misalignment and kyphosis. They may therefore reduce the activities of everyday life, cause respiration dysfunction and increase the prevalence of lung disease [4, 5].
Osteoporosis has been widely recognised as a major comorbidity in chronic obstructive pulmonary disease (COPD) patients, being present in 36–60 % of patients with COPD, a rate that is two to five fold higher than that detectable in age-matched healthy subjects [5, 6]. The underlying causes of osteoporosis in COPD remain unclear, but several factors are significantly related to reduced bone density in COPD, including older age, female sex, and body mass index (BMI). The relationship with other proposed factors, such as tobacco smoking, physical inactivity and corticosteroid therapy, is still controversial [6–8].
Percutaneous vertebroplasty (VTP) is a minimally invasive technique employing the injection of liquid polymethylmethacrylate (PMMA) cement into a fractured vertebral body [9, 10].
VTP was first reported in the literature in 1987 by Galibert and Deramond [11], for the treatment of a cervical vertebral haemangioma. In the following years, evolution of cement and expansions of indications have resulted in several useful vertebral augmentation procedures [12]. VTP is now considered a safe and effective procedure for the treatment of Osteoporotic VCFs (OVCFs) [13–17]. Pain relief and improvement of mobility and function after VTP is immediate, long lasting and is considered significantly better than conservative medical treatment [18–20].
The aim of our study was to investigate the effects of VTP and the changes of respiratory function in COPD patients with single dorsal VCFs due to osteoporosis.
Materials and methods
Patient population and preoperative management
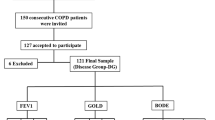
From September 2011 to August 2013, we observed in our department 123 patients with COPD affected by OVCFs. All patients reported that severe back pain, resistant to conservative treatment, occurred no later than 3 months before. Those reporting radicular pain and symptoms suggestive for neurological involvement were excluded.
The diagnosis and selection of patients was made by a pulmonologist and interventional radiologist in consensus, on the basis of clinical history and physical examination; treatment indications were made by an interventional radiologist based on imaging findings.
All patients presented a VCF at spine radiography. Diagnosis was confirmed by spine magnetic resonance (MR) examination. In some cases, computed tomography was also performed in order to exclude the interruption of vertebral posterior wall with the potential for intracanal bone fragment (Fig. 1).

A 72-year-old woman with osteoporosis and COPD. MR imaging shows an acute T8 compression fractures with deformity of the vertebral body. a Sagittal T1-weighted: low signal intensity in the collapsed T8 vertebral body compared with the normal bone marrow in other adjacent vertebral bodies. b Sagittal T2-STIR: bone marrow high signal intensity secondary to oedema
Inclusion criteria were a single dorsal vertebral involvement, with MR findings of bone marrow oedema, without intracanal bone fragments and refractory pain to conventional medical treatment from at least 3 months. The osteoporotic condition was assessed by bone densitometry, and spirometry was performed before and after treatment.
A total of 45 patients were enrolled (29 men, 16 women; mean age 71.4 years, range 65–77 years) and underwent VTP treatment. All patients continued their drug therapy for osteoporosis and COPD and were encouraged to terminate their analgesic or anti-inflammatory therapy the days after VTP procedure.
Our inner Ethical Committee approved the study protocol and written informed consent was obtained from all patients before VTP procedure.
Percutaneous procedure—operative technique and devices
All procedures were performed under fluoroscopic guidance in an angiographic suite (Allura Xper FD 20; Philips Healthcare, Best, The Netherlands) with patients in the prone position with the spine slightly hyperextended. All procedures were performed under local anaesthesia with close monitoring of the anaesthetist (buffered lidocaine/bupivacaine 1 %/0.25 % for skin incision; ropivacaine 10 mg/ml for periosteal anaesthesia). The access was through the left pedicle in all cases using a 13-G × 150 mm straight injection cannula (OptiMed, Ettlingen, Germany), according to the habit of the first operator. Our technique did not differ from the standard well-established technique widely used, described elsewhere [21]. The cement, polymethylmethacrylate (PMMA; OptiMed, Ettlingen, Germany), was injected inside the vertebral body as uniformly as possible under fluoroscopic control (Figs. 2 and 3).

A 79-year-old man with osteoporosis and COPD. Fluoroscopic biplanar post-procedure control in the lateral (a) and antero-posterior (b) view. Optimal and uniform distribution of PMMA within T6 vertebral body

Fluoroscopic end-procedure control lateral (a) and antero-posterior (b) view; notice cement filling of the basivertebral vein near posterior vertebral wall. Intraprocedure fluoroscopic lateral (c) and antero-posterior (d) view of another patient showing injection cannula still in place inside the vertebral body with the tip close to the anterior vertebral wall during the last phases of cement injection; notice cement spread throughout the middle third of vertebral body although the tip is so far anteriorly located
The duration of the whole procedure was approximately 25–30 min. After the procedure, the patient was placed in a supine position and asked to lie in bed motionless for at least 4 hours to allow complete consolidation of the PMMA prior to axial loading. In the absence of complications, patients were discharged 4–6 h after the procedure. Antibiotics (cefazolin) were administered the day of procedure. In eight patients with diabetes, antibiotic coverage was extended up to 3 days after the procedure.
Clinical assessment and follow-up
All patients underwent physical and neurological examination prior to and after the VTP procedure.
During the screening period, the use of analgesic and anti-inflammatory drugs, as well as osteoporosis and COPD therapy, was recorded. No deaths were observed in the 12-month follow-up period.
Pain intensity was evaluated by an 11-point visual analogue scale (VAS) score (0 = absence of pain, 10 = unbearable pain) administered before, 1 week, 3 months and 12 months after the procedure.
Spirometric examination was performed before (baseline) and 1 week, 3 months and 12 months after treatment. In accordance with the literature we considered as benchmarks percentage vital capacity (VC %), percentage forced vital capacity (FVC %), and percentage forced expiratory volume in 1 s (FEV1 %).
Statistical analysis
The correlations between VAS score and VC, VAS score and FVC, VAS score and FEV1 were evaluated by non-parametric Spearman test. The difference between the baseline, 1-week, 3-month and 12-month values in VAS score, VC, FVC and FEV1 were evaluated using the Wilcoxon matched-pairs signed rank test. A p value lower than 0.05 was considered significant. Data were expressed as mean value ± standard deviation (SD). Statistical analyses were performed using commercial software (Graph-pad Prism 5, San Diego, CA).
Results
Twelve months of follow-up were completed for all 45 patients. A significant variation (p < 0.001) between the VAS-score values, VC and FVC values obtained before the procedure and those obtained at 1 week, 3 months and 12 months after treatment was recorded without significant changes in FEV throughout the follow-up period (Fig. 4). A marked decrease in pain was observed 1 week after the procedure, with a subsequent slight but continuous decrease over time (Table 1); VC % and FVC % values slightly and continuously improved over time, reaching a plateau at 3 months (Tables 2 and 3). FEV1 values did not significantly differ between the pre-VTP ones and the ones obtained 1 week after the procedure (p = 0.6840), at 3 months’ (p = 0.5140) and at 12 months’ follow-up (p = 0.9496) (Table 4). A significant correlation was observed between VAS-score values and VC % (p = 0.0167), and VAS-score values and FVC % (p = 0.0028); the correlation between the VAS-score values and FEV1 values was not significant (p = 0.6583) (Fig. 5).

Graphical representation of the mean VAS score (a), VC % (b), FVC % (c) and FEV1 (d) values before VTP (baseline) and at 1 week, 3 months and 12 months of follow-up evaluation. The improvement was significant for VAS, VC and FVC. FEV1 values did not change significantly over the whole 1 year follow-up period

Graphical representation of the crossed-correlation results between the VAS score, VC%, FVC%, and FEV1 values using the Spearman test. A significant (p < 0.001) correlation between VAS score and VC% (r = −0.9429), as well as VAS score and FVC% (r = −1.0000) resulted (a, b). The correlation between VAS score and FEV1 was not significant (r = −0.2571) (c)
Discussion
OVCFs are known to result in impaired respiratory function through reduction of thoracic mobility and postural deformity, especially in patients with co-existent pulmonary disease, such as COPD patients [22]. Back pain due to acute and sub-acute thoracic OVCFs limits movements of the thorax and can represent a factor contributing to ventilatory disturbance in COPD patients, influencing the involvement of accessory muscles to improve the change of air volume and increasing muscular effort [23, 24].
In this study VTP was performed in patients with symptomatic thoracic OVCFs affected by moderate/severe COPD (according to the GOLD severity scale) with the aim of relieving thoracic back pain. The pain improvement was evaluated through an 11-point VAS score and the related pulmonary functional outcome was assessed through spirometric parameters: VC, FVC and FEV1.
Consistent with previous results reported in the literature, VAS score assessment demonstrates a significantly higher improvement of symptoms with significant pain reduction already 1 week after VTP, maintained during long-term follow-up without further significant modification [18, 25–27]. In accordance with these studies, we observed a progressive improvement of spirometric parameters such as VC and FVC 1 week after VTP, with further gradual improvement over the entire follow-up period. In another trial, Dong et al. [5] also reported an improvement of pulmonary function after both VTP and kyphoplasty (KPT). In this study, VC and FVC were already significantly increased 3 days after procedures, whereas maximum voluntary ventilation (MVV) started to improve 3 months later.
The improvement in pulmonary function was paralleled by decreased VAS values showing significant correlation between them [5]. MVV values reflect the respiratory muscle endurance and are reduced in osteoporotic patients due to their inactivity. Women with osteoporosis typically have impaired lung volumes, restricted rib mobility, reduced respiratory muscle endurance and reduced isometric muscle strength [28]. Since both VC and FVC directly correlate with restrictive respiratory impairment, which is in turn correlated with thoracic pain, we can assume that the analgesic effect of VTP can reduce restriction of thoracic movements, thus improving ventilation in COPD patients. However, if we consider the different timing of evolution between the VAS score and spirometric parameters, it is unlikely that pain reduction by itself is the only factor involved in such improvement. In this context, it is more likely that pain reduction may allow wider thoracic/costal movements over time, thus improving the strength of respiratory muscles and eventually leading to improvement of the restrictive syndrome.
Tanigawa et al. [23] evaluated the effects of VTP on respiratory function in patients with acute/subacute OVCFs occurring at single or multiple levels in the thoracic, thoracic-lumbar and lumbar segments. They reported significant pain reduction in all patients, independent of the number of levels involved and on their segmentary localisation. However, significant improvement of FVC was reported exclusively in the group with thoracic involvement, independent of single- or multiple-level involvement. They concluded that pain is the main determinant of such restrictive syndromes, owing to decreased thoracic motion. Alleviation of local kyphosis was also considered a contributing factor, but mainly in the cases of multiple level OVCFs.
Several previous studies underlined the role of reduction of kyphosis and restored vertebral height in the improvement of pulmonary function in OVCF patients [5, 29, 30]; in these studies the authors underline the dual role of KPT for both back pain relief and restoration of vertebral body height and kyphotic wedge angle. Dong et al. [5] stated that patients with thoracic OVCFs might obtain more benefit from KPT than VTP because of reduction of local kyphotic angle (LKA) and its related back pain relief. Other studies in contrast suggested that improvement of sagittal alignment and restoration of vertebral body height did not significantly influence respiratory air exchange and LKA did not show correlation with any parameter of pulmonary function. Yang et al. [24] reported that, despite the reduction of LKA in their patients being clinically significant, correlation with lung functional parameters was not significant: as for VTP, balloon KPT contribution acted only on pain relief, which was demonstrated to be the major cause of impairment of lung volumes and reduction of respiratory muscle endurance. A systematic review of osteoporosis-related kyphosis and respiratory function impairment demonstrates that declines in VC secondary to kyphosis seem modest and directly related to the number of vertebral fractures and degree of kyphosis [31]. Moreover, according to Chen et al. [32], VTP does not seem to significantly affect vertebral body height. Accordingly, many cases in which increased vertebral height was reported seem to be mostly secondary to dynamic mobility of the vertebral body itself.
In a recent study, Kelekis et al. [33] reported another interesting effect of VTP. They performed a prospective comparative electronic baropodometer registration analysis of weight projection areas in feet of patients with OVCFs treated with VTP and treated conservatively. Pain related to compression fractures not only affect respiratory dynamic but also produce wide and deep effects on overall body posture that ultimately influence load distribution between left and right feet and among different regions of the same sole. They reported a statistical variation and normalisation of load weight distribution before and after VTP that was not found in the group of patients treated conservatively. These results suggest that baropodemeter analysis could be potentially used as another objective index to evaluate the outcome.
According to these considerations and grounding on our experience we do not believe that vertebral body height restoration after VTP, when its happening is significant, could exercise significant influence on the outcome of these patients. Moreover, because we restricted the study to single-level OVCF, the local kyphotic angle improvement would be minimal, or at least not significant for the purpose of pulmonary function improvement. However, the position of the patients on the operating table is prone with the spine slightly hyperextended, which should widen the fracture lines, allowing more cement to diffuse easily into the vertebral body and thus improving stabilisation.
During the follow-up period we did not find new vertebral collapses, neither adjacent nor distant.
VAS values showed a steep decrease during the first week, whereas these remained almost stable during the following follow-up checks, showing only minimal further improvement, which in some cases was not statistically significant. These results are congruous with the generally and widely recognised effect of VTP. The further minimal VAS improvement after 1 month can be considered a result of the overall better physical condition of the patients rather than an intrinsic effect of the procedure itself, whose effects are usually almost immediately evident.
There were no other complications related to the procedure, such as significant cement leakages or infections in the treated region. Thoracic pain beyond the involved level showed a steep decrease since the first days after procedure, keeping quite stable and significantly reduced after 1 month and over the following follow-up period. Some patients who complained about lower back pain unrelated to the vertebral collapse before the procedure, continued to complain steadily after the procedure. We have not been able to detect any influence of such lower back pain on the outcome of these patients. Indeed, the improvement of VC and FVC of patients complaining of lower back pain did not show a significant difference, compared with the other patients.
As mentioned above, the choice to restrict the study to patients with only single vertebral collapse, with the purpose to ease the evaluation of the results and scavenge further bias, represents an evident limitation. Another limitation, apart from the small population of patients, is the absence of a control group. An optimal evaluation of the effect of VTP on respiratory function in COPD patients would require a randomised controlled study comparing VTP with a control group, such as a conservative treatment group, a sham-treated group or a group receiving respiratory rehabilitation. In addition, the choice to observe our patients over a 12-month period may have some disadvantages. Indeed, in such a short period of observation, the incidence of respiratory complications—such as acute COPD exacerbations—is lower and this could have influenced the results. Regarding the use of VTP compared with KPT, in addition to the considerations listed above, some advantages of VTP over KPT that should be considered are shorter operation time, smaller amount of PMMA required, reducing the incidence of complications, as well as the lower overall cost of VTP [11, 12, 34–38].
However VTP is a treatment of proven effectiveness in reducing pain secondary to acute OVCFs. Notwithstanding the above mentioned limitations, it also appears to be effective in improving VC and FVC of patients with COPD.
Conclusions
VTP treatment has led to improvement of both respiratory impairment and overall quality of life for patients affected by single thoracic OVCFs with moderate or severe COPD. We therefore recommend this treatment in the management of such patients.
Abbreviations
- COPD:
-
Chronic obstructive pulmonary disease
- OVCFs:
-
Osteoporotic vertebral compression fractures
- VTP:
-
Vertebroplasty
- PMMA:
-
Polymethylmethacrylate
References
Barth RW, Lane JM (1988) Osteoporosis. Orthop Clin North Am 19:845–858
Lane NE (2006) Epidemiology, etiology, and diagnosis of osteoporosis. Am J Obstet Gynecol 194:S3–S11
Wu SS, Lachmann E, Nagler W (2003) Current medical, rehabilitation, and surgical management of vertebral compression fractures. J Womens Health 12:17–26
Tanigawa N, Kariya S, Kojima H et al (2008) Improvement in respiratory function by percutaneous vertebroplasty. Acta Radiol 49:638–643
Dong R, Chen L, Gu Y et al (2009) Improvement in respiratory function after vertebroplasty and kyphoplasty. Int Orthop 33:1689–1694
Silva DR, Coelho AC, Dumke A et al (2011) Osteoporosis prevalence and associated factors in patients with COPD: a cross-sectional study. Respir Care 56:961–968
Graat-Verboom L, Smeenk FW, van den Borne BE et al (2012) Risk factors for osteoporosis in Caucasian patients with moderate chronic obstructive pulmonary disease: a case control study. Bone 50:1234–1239
Tantucci C (2012) COPD and osteoporosis: something more than a comorbidity. Endocrine 42:5–6
Eckel TS, Olan W (2009) Vertebroplasty and vertebral augmentation techniques. Tech Vasc Interv Radiol 12:44–50
Hurley MC, Kaakaji R, Dabus G et al (2009) Percutaneous vertebroplasty. Neurosurg Clin N Am 20:341–359
Galibert P, Deramond H, Rosat P, Le Gars D (1987) Preliminary note on the treatment of vertebral angioma percutaneous acrylic vertebroplasty. Neurochirugie 33:166–168, Article in French
Garfin SR, Yuan HA, Reiley MA (2001) New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine 26:1511–1515
Anselmetti GC, Marcia S, Saba L et al (2012) Percutaneous vertebroplasty: multi-centric results from EVEREST experience in large cohort of patients. Eur J Radiol 81:4083–4086
Wong CC, McGirt MJ (2013) Vertebral compression fractures: a review of current management and multimodal therapy. J Multidiscip Healthc 6:205–214
Hsieh MK, Chen LH, Chen WJ (2013) Current concepts of percutaneous balloon kyphoplasty for the treatment of osteoporotic vertebral compression fractures: evidence-based review. Biomed J 36:154–161
Chandra RV, Yoo AJ, Hirsch JA (2013) Vertebral augmentation: update on safety, efficacy, cost effectiveness and increased survival? Pain Physician 16:309–320
Chitale A, Prasad S (2013) An evidence-based analysis of vertebroplasty and kyphoplasty. J Neurosurg Sci 57:129–137
Voormolen MH, Mali WP, Lohle PN et al (2007) Percutaneous vertebroplasty compared with optimal pain medication treatment: short-term clinical outcome of patients with subacute or chronic painful osteoporotic vertebral compression fractures. The VERTOS study. AJNR Am J Neuroradiol 28:555–560
Klazen CA, Lohle PN, de Vries J et al (2010) Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (Vertos II): an open-label randomised trial. Lancet 376:1085–1092
Masala S, Calabria E, Nano G et al (2013) Traumatic burst fracture with spinal channel involvement augmentation with bioactive strontium-hydroxyapatite cement. Case Rep Orthop 2013:613149
Mathis JM (2003) Percutaneous vertebroplasty: complication avoidance and technique optimization. AJNR Am J Neuroradiol 24:1697–1706
Carlin BW (2012) COPD and associated comorbidities: a review of current diagnosis and treatment. Postgrad Med 124:225–240
Tanigawa N, Kariya S, Komemushi A, Nakatani M, Yagi R, Sawada S (2012) Added value of percutaneous vertebroplasty: effects on respiratory function. AJR Am J Roentgenol 198:W51–W54
Yang HL, Zhao L, Liu J et al (2007) Changes of pulmonary function for patients with osteoporotic vertebral compression fractures after kyphoplasty. J Spinal Disord Tech 20:221–225
Klazen CA, Verhaar HJ, Lampmann LE et al (2007) VERTOS II: percutaneous vertebroplasty versus conservative therapy in patients with painful osteoporotic vertebral compression fractures; rationale, objectives and design of a multicenter randomized controlled trial. Trials 8:33
Farrokhi MR, Alibai E, Maghami Z (2011) Randomized controlled trial of percutaneous vertebroplasty versus optimal medical management for the relief of pain and disability in acute osteoporotic vertebral compression fractures. J Neurosurg Spine 14:561–569
Rousing R, Hansen KL, Andersen MO, Jespersen SM, Thomsen K, Lauritsen JM (2010) Twelve-months follow-up in forty-nine patients with acute/semiacute osteoporotic vertebral fractures treated conservatively or with percutaneous vertebroplasty: a clinical randomized study. Spine (Phila Pa 1976) 35:478–482
Cimen OB, Ulubaş B, Sahin G, Calikoğlu M, Bağiş S, Erdoğan C (2003) Pulmonary function tests, respiratory muscle strength, and endurance of patients with osteoporosis. South Med J 96:423–426
Ettinger B, Black DM, Nevitt MC et al (1992) Contribution of vertebral deformities to chronic back pain and disability. J Bone Miner Res 7:449
Ryan PJ, Blake G, Herd R, Fogelman I (1994) A clinical profile of back pain and disability in patients with spinal osteoporosis. Bone 15:27
Harrison RA, Siminoski K, Vethanayagam D, Majumdar SR (2007) Osteoporosis-related kyphosis and impairments in pulmonary function: a systematic review. J Bone Miner Res 22:447–457
Chen YJ, Chen HY, Tsai PP, Lo DF, Chen HT, Hsu HC (2012) Significance of dynamic mobility in restoring vertebral body height in vertebroplasty. AJNR Am J Neuroradiol 33:57–60
Kelekis A, Filippiadis DK, Vergadis C et al (2014) Comparative prospective study of load distribution projection among patients with vertebral fractures treated with percutaneous vertebroplasty and a control group of healthy volunteers. Cardiovasc Intervent Radiol 37:186–192
Frankel BM, Monroe T, Wang C (2007) Percutaneous vertebral augmentation: an elevation in adjacent-level fracture risk in kyphoplasty as compared with vertebroplasty. Spine J 7:575–582
Lin WC, Lee YC, Lee CH et al (2008) Refractures in cemented vertebrae after percutaneous vertebroplasty: a retrospective analysis. Eur Spine J 17:592–599
Lieberman IH, Dudeney S, Reinhardt MK, Bell G (2001) Initial outcome and efficacy of “kyphoplasty” in the treatment of painful osteoporotic vertebral compression fractures. Spine (Phila Pa 1976) 26:1631–1638
Masala S, Ciarrapico AM, Konda D, Vinicola V, Mammucari M, Simonetti G (2008) Cost-effectiveness of percutaneous vertebroplasty in osteoporotic vertebral fractures. Eur Spine J 17:1242–1250
Svedbom A, Alvares L, Cooper C, Marsh D, Ström O (2013) Balloon kyphoplasty compared to vertebroplasty and non-surgical management in patients hospitalised with acute osteoporotic vertebral compression fracture—a UK cost-effectiveness analysis. Osteoporos Int 24:355–367
Acknowledgements
The scientific guarantor of this publication is Professor Salvatore Masala M.D. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. No complex statistical methods were necessary for this paper. Institutional Review Board approval was not required because this study did not require off-label use of materials, methods and procedures non-standardised. Written informed consent was obtained from all subjects (patients) in this study. Methodology: prospective, observational, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Masala, S., Magrini, A., Taglieri, A. et al. Chronic obstructive pulmonary disease (COPD) patients with osteoporotic vertebral compression fractures (OVCFs): improvement of pulmonary function after percutaneous vertebroplasty (VTP). Eur Radiol 24, 1577–1585 (2014). https://doi.org/10.1007/s00330-014-3165-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-014-3165-2