
Abstract
The purpose of this study was to compare sensitivity, specificity, and postprocessing time of a colon dissection approach to regular 3D-endoluminal workup of computed tomography (CT) colonography for the detection of polypoid lesions. Twenty-one patients who had received conventional colonoscopy after CT colonography were selected; 18 patients had either colon polyps or colon cancer and three had no findings. CT colonography was performed using a 4-channel multi-detector-row (MDR) CT in ten cases and a 16-channel MDR-CT in 11 cases. A blinded reader retrospectively evaluated all colonographies using both viewing methods in a randomized order. Thirty-seven polyps were identified by optical colonoscopy. An overall per-lesion sensitivity of 47.1% for lesions smaller than 5 mm, 56.3% for lesions between 5 mm and 10 mm, and 75.0% for lesion larger than 10 mm was calculated using the colon dissection approach. This compared to an overall per-lesion sensitivity of 35.3% (<5 mm), 81.5% (5–10 mm), and 100.0% (>10 mm) using the endoluminal view. The average time consumption for CT colonography evaluation with the colon dissection software was 10 min versus 38 min using the endoluminal view. A colon dissection approach may provide a significant time advantage for evaluation of CT colonography while obtaining a high sensitivity. It is especially superior in the detection of lesions smaller than 5 mm.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Since its introduction in 1994 by Vining [1], computed tomography (CT) colonography has rapidly evolved, with substantial improvements in both scanner hardware and reconstruction software. Different methods for reviewing the acquired source transverse CT images are used. Besides evaluation of two-dimensional (2D) axial images, multiplanar reformatted images (MPR) and three dimensional (3D) display modes are commonly used. Several studies with different results have been published in recent years to compare axial image review with a variety of 3D modes [2–4].
The first aim of 3D reconstruction was to create a simulated intraluminal view of the colon to get a colonoscopy-like impression. This can be achieved using 3D endoluminal image rendering. Depending on the software used, navigation through the reconstructed colon can be performed with the help of a self-created, semiautomated, or automated path [5], and ante- and retrograde endoluminal cine views of the colon can be displayed. Most systems are also linked with multiplanar reformation software to further investigate lesions. The main disadvantage of this “endoluminal colonography” is the review time for postprocessing that is required. This is potentially limiting the use of CT colonography for the screening of larger populations. Although good results have been achieved with this technique, alternative visualization methods would be desirable to further accelerate postprocessing time to enable a more widespread use of CT colonography for colon cancer screening.
One approach to speed up CT colonography postprocessing is to unfold the whole 360° inner colon along a previously created path for a simultaneous review of the complete circumference (Fig. 1).

Fully automatically created path along the colon prior to colon dissection
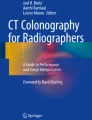
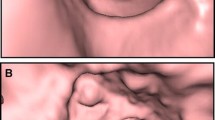
This unfolding makes it unnecessary to navigate through the colon in ante- and retrograde direction to look behind colonic folds. Vos et al. obtained their 360° view by using an unfolded cube projection, which renders 6°×90° images together [6]. In our approach, the colon is fully dissected and unfolded similar to a pathological preparation (Fig. 2), featuring an overlapping projection at the top and bottom, resulting in a 380° display.

Colon polyp in three different modalities; conventional colonoscopy (a), conventional colonography (b), and computed tomography (CT) colonography using colon dissection software (c)
The purpose of this study was to compare the standardized CT colonography workup of our institution based on an endoluminal view with this alternative 3D projection focusing on time consumption as well as sensitivity and specificity in detection of colorectal lesions.
Materials and methods
Twenty-one patients (nine men, 12 women; mean age 58.1 years, range 34–76) were included. Eighteen had a total of 37 endoscopically confirmed colorectal lesions; three had no findings. One lesion was identified as a colorectal carcinoma, one as a lipoma, and 35 as adenomatous polyps with a size ranging between 2 mm and 15 mm. CT colonography was performed following a standardized protocol for bowel cleansing over 2 days. Informed consent was obtained prior to the examination. With the patient positioned on the CT table, 40 mg of Hyoscine-N-butylbromide (Buscopan; Boehringer Ingelheim, Ingelheim, Germany) was administered intravenously for bowel relaxation. Thereafter, room air was carefully insufflated using a manual balloon pump through a rectal enema tube to achieve pneumocolon. The patient controlled the amount of filling and stopped air insufflation if discomfort was experienced. Air filling and distension of the colon was evaluated on the CT scout before CT colonography. Additional air was insufflated in case of insufficient distension of the colon. CT scans were performed with the patient in both supine and prone positions.
In 11 patients, a four-channel MDR-CT (Philips MX 8000, Philips Medical Systems, Best, NL) was used. Ten patients received CT colonography using a 16-channel MDR-CT (Philips MX 8000 IDT). Scan parameters are given in Table 1.
A blinded radiologist (TRF) with previous experience in both display methods reviewed all scans in a randomized order. The reader was unaware of the prevalence of polyps in the study group. All evaluations were performed on the same PC-based dedicated CT workstation (Extended Brilliance Workspace, Philips, Best, NL). For the endoluminal display ante- and retrograde colonoscopic views were obtained along a manually created path using both prone and supine image data sets (Extended Brilliance Workspace 1.2). Parallel-displayed MPR images were used to evaluate suspected lesions from the endoluminal views. Findings were scored with respect to size and location.
CT colonography using the colon dissection workup was also performed using both prone and supine data sets. The evaluation was performed as a single fly-through exclusively using the dissection display (Philips “Filet View”, Extended Brilliance Workspace 2.0 beta). No parallel display of multiplanar reformatted images was used in these readings. Findings were again scored in respect to size and location.
Statistical analysis
Statistically significant differences were determined using the Pearson’s product-moment correlation on a 95% level of significance. Normal distribution was tested using the Kolmogorov–Smirnov test. In non-normal-distributed and ordinal-scaled parameters, Spearman’s rank correlation was used (95% level of significance). In addition, an analysis of variance was performed. All statistics were calculated with SPSS 11.0 (SPSS GmbH, Munich, Germany).
Results
Conventional colonoscopy revealed 37 colorectal lesions (35 polypoid lesions, one colon carcinoma, and one lipoma) in 18 patients. Three patients had no findings. There were 17 polyps smaller than 5 mm and 16 between 5–10 mm. Four lesions measured more than 10 mm, including the colon carcinoma and the lipoma.
Conventional endoluminal view
The endoluminal view obtained an overall per-lesion sensitivity of 62.2% and a specificity of 92.1%. The endoluminal view had a sensitivity of 66.7% and specificity of 84.2% in the four-channel MDR-CT data sets compared with a sensitivity of 56.3% and specificity of 100.0% using the 16-channel MDR-CT data sets. Table 2 gives overall sensitivity and specificity in respect to lesion size.
Virtual colon dissection view
The colon dissection view obtained an overall per-lesion sensitivity of 54.1% and a specificity of 81.6%. It reached a sensitivity of 42.9% and specificity of 84.2% with four-channel MDR-CT data sets and a sensitivity of 68.8% and specificity of 79.0% using 16-channel MDR-CT data sets. Table 3 gives overall sensitivity and specificity in respect to lesion size.
Evaluation time
The average total time needed for evaluation using the colon dissection view was 10 min (5–13 min) versus 38 min (23 min–55 min) using the combination of endoluminal views and MPR.
Discussion
This study indicates that improvements in CT colonography postprocessing can result in a significantly faster process of evaluating the obtained CT data. The average time consumption for evaluation of a CT colonography data set using the endoluminal view approach was 38 min. This is within the range of results published in previous studies [4, 6–9] or slightly above it. One reason for increased speed may be that the software used in this study did not provide reliable automated path extraction requiring a manual navigation through the colon in prone and supine position. Furthermore the virtual “fly-through” was performed in ante- and retrograde direction to enhance surface visibility. As previously published, visibility can be enhanced up to 95% using this technique compared with 75% using either forward or reverse viewing solely [10]. The major contributor to the reduction in time for evaluation has to be attributed to the virtual dissection view approach. This technique does not require ante- and retrograde viewing because a surface visibility of up to 98% [10] is already obtained in a single direction mode. It is our opinion that investigation of both prone and supine positions is still required to overcome visibility limitations due to residual fluid and stool. Colon dissection mode took 10 min for investigation on average, which is less than one third compared with the conventional view in this study and is even below previously published data [4] using a similar method. Our method also uses a Mercator projection but, in comparison with Hoppe et al. using a 4×90° view, it provides a full 360° view with an additional overlap of 10° at the top and at the bottom, totaling in a 380° view.
Aside from the fact that the colon dissection mode is superior with regard to time consumption and therefore may be eligible for widespread use in clinical routine, it provides competitive sensitivity and specificity.
In the first studies on CT colonography (or “virtual colonoscopy”), the combined use of 2D and 3D images together was assumed to provide the highest sensitivity [7, 8]. Although some of the newer studies still favor a solitary 2D interpretation over 3D viewing [4], other publications prefer 3D reconstructions [3, 6]. The impressive results achieved in the latter studies all go along with further improved CT colonography software as well as CT scanner hardware.
The overall per-lesion specificity and sensitivity achieved with the endoluminal approach used routinely in our institution was in the range of most of the previous published studies [5, 11, 12]. The colon dissection view obtained a lower sensitivity and specificity in the overall performance in this study. This might be due to the fact that the prototype version of the virtual dissection view did not provide MPR integration. In contrast to most commercially available endoluminal view software systems, it was not possible to further evaluate lesions detected with the dissection mode in respect to their location in prone and supine positions, for example. This might especially be the cause of the relatively low sensitivity for lesions between 5–10 mm.
However the performance was better using 16-channel MDR-CT data with higher spatial resolution. In this subgroup, the sensitivity was 68.8% and therefore superior to the endoluminal view (56.3%). In accordance with the findings of Rottgen et al. [11], we obtained higher sensitivities, especially in detection of small lesions (<5 mm), using higher spatial resolutions. Overall sensitivity for lesions smaller than 5 mm was 47.1% with the colon dissection view and by this, within the range of previous studies published [7, 8, 13, 14] but superior to the endoluminal view sensitivity in our study. This fact points out the potential of this viewing method. It is much easier to pick out a very small lesion, especially if located on a fold, with the dissection view approach.
An often discussed issue is the diverse performance of experienced and inexperienced readers using 3D reconstruction software. Although the reader in this study was an experienced radiologist, he was untrained regarding the virtual dissection software, as this was a prototype version. Further studies need to evaluate whether there is a learning curve and whether higher sensitivities and specificities can be achieved after becoming familiar with this visualization method.
CT colonography is still a rapidly evolving technique. Since studies with large numbers of patients [9] have been published, it is gaining more acceptance in screening for colorectal cancer. The introduction of new CT scanners and postprocessing software improved sensitivity and specificity over the last 10 years. Further developments, such as automated mass detection, could help to improve sensitivity and specificity and decrease reading time. Patient compliance can be further enhanced with new positioning techniques or with performing the examination without bowel cleansing.
In conclusion, this pilot study shows a potential for a superior performance of a colon dissection postprocessing approach compared with the conventional endoluminal workup of CT colonography in regard to time efficiency. Furthermore, the colon dissection view obtained competitive sensitivity and specificity, especially when using high-resolution, 16-channel MDR-CT data sets. Further studies are warranted to provide better understanding of this approach and to determine what combination of 2D and 3D postprocessing yields the best results.
References
Vining D, Shifrin R, Grishaw E (1994) Virtual colonoscopy. Radiology 193:446
Karadi C, Beaulieu CF, Jeffrey RB Jr, Paik DS, Napel S (1999) Display modes for CT colonography. Part I. Synthesis and insertion of polyps into patient CT data. Radiology 212:195–201
Beaulieu CF, Jeffrey RB Jr, Karadi C, Paik DS, Napel S (1999) Display modes for CT colonography. Part II. Blinded comparison of axial CT and virtual endoscopic and panoramic endoscopic volume-rendered studies. Radiology 212:203–212
Hoppe H, Quattropani C, Spreng A, Mattich J, Netzer P, Dinkel HP (2004) Virtual colon dissection with CT colonography compared with axial interpretation and conventional colonoscopy: preliminary results. Am J Roentgenol 182:1151–1158
Bruzzi JF, Moss AC, Brennan DD, MacMathuna P, Fenlon HM (2004) Colonic surveillance by CT colonography using axial images only. Eur Radiol 14(5):763–767. Epub 2004 Feb 19
Pickhardt PJ (2003) Three-dimensional endoluminal CT colonography (virtual colonoscopy): comparison of three commercially available systems. Am J Roentgenol 181:1599–1606
Vos FM, van Gelder RE, Serlie IW, Florie J, Nio CY, Glas AS et al (2003) Three-dimensional display modes for CT colonography: conventional 3D virtual colonoscopy versus unfolded cube projection. Radiology 228:878–885
Macari M, Milano A, Lavelle M, Berman P, Megibow AJ (2000) Comparison of time-efficient CT colonography with two- and three-dimensional colonic evaluation for detecting colorectal polyps. Am J Roentgenol 174:1543–1549
Dachman AH, Kuniyoshi JK, Boyle CM, Samara Y, Hoffmann KR, Rubin DT et al (1998) CT colonography with three-dimensional problem solving for detection of colonic polyps. Am J Roentgenol 171:989–995
Pickhardt PJ, Choi JR, Hwang I, Butler JA, Puckett ML, Hildebrandt HA et al (2003) Computed tomographic virtual colonoscopy to screen for colorectal neoplasia in asymptomatic adults. N Engl J Med 349:2191–2200
Paik DS, Beaulieu CF, Jeffrey RB Jr, Karadi CA, Napel S (2000) Visualization modes for CT colonography using cylindrical and planar map projections. J Comput Assist Tomogr 24:179–188
Rottgen R, Schroder RJ, Lorenz M, Herbel A, Fischbach F, Herzog H et al (2003) CT-colonography with the 16-slice CT for the diagnostic evaluation of colorectal neoplasms and inflammatory colon diseases. Rofo Fortschr Geb Rontgenstr Neuen Bildgeb Verfahr 175:1384–1391
Pineau BC, Paskett ED, Chen GJ, Espeland MA, Phillips K, Han JP et al (2003) Virtual colonoscopy using oral contrast compared with colonoscopy for the detection of patients with colorectal polyps. Gastroenterology 125:304–310
Hara AK, Johnson CD, Reed JE, Ehman RL, Ilstrup DM (1996) Colorectal polyp detection with CT colography: two- versus three-dimensional techniques. Work in progress. Radiology 200:49–54
Morrin MM, Farrell RJ, Kruskal JB, Reynolds K, McGee JB, Raptopoulos V (2000) Utility of intravenously administered contrast material at CT colonography. Radiology 217:765–771
Taylor SA, Halligan S, Burling D, Morley S, Bassett P, Atkin W, Bartram CI (2004) CT colonography: effect of experience and training on reader performance. Eur Radiol 14(6):1025–1033. Epub 2004 Feb 10. PMID: 14872280
Luboldt W, Tryon C, Kroll M, Toussaint TL, Holzer K, Hoepffner N, Vogl TJ (2005) Automated mass detection in contrast-enhanced CT colonography: an approach based on contrast and volume. Eur Radiol 15(2):247–253. Epub 2004 Oct 15. PMID: 15490178
Luboldt W, Kroll M, Wetter A, Toussaint TL, Hoepffner N, Holzer K, Kluge A, Vogl TJ (2004) Phase- and size-adjusted CT cut-off for differentiating neoplastic lesions from normal colon in contrast-enhanced CT colonography. Eur Radiol 14(12):2228–2235. Epub 2004 Sep 23. PMID: 15449012
Bruzzi JF, Moss AC, Brennan DD, MacMathuna P, Fenlon HM (2004) Colonic surveillance by CT colonography using axial images only. Eur Radiol 14(5):763–767. Epub 2004 Feb 19. PMID: 14986051
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Juchems, M.S., Fleiter, T.R., Pauls, S. et al. CT colonography: comparison of a colon dissection display versus 3D endoluminal view for the detection of polyps. Eur Radiol 16, 68–72 (2006). https://doi.org/10.1007/s00330-005-2805-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-005-2805-y