
Abstract
Although popliteal cysts are most frequently identified in patients with osteoarthritis (OA), they may occur in patients with rheumatoid arthritis (RA), in which serious complicated cases such as cyst rupture can be developed. The objective of this study was to report four patients with RA (six knees) in combination with OA with a brief review of literature of previous similar published cases. This is a retrospective review of case records of patients with refractory and/or complicated popliteal cysts, who have successfully treated with arthroscopic intervention. We suggest that arthroscopic interventions such as radical debridement, synovectomy, biomechanical valve excision, and/or cystectomy should be considered in patients with refractory and complicated popliteal cysts associated with RA or RA in combination with OA.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Rheumatoid arthritis (RA) is one of the most prevalent chronic inflammatory arthritis affecting approximately 1% of the population worldwide. It is characterized by inflammatory proliferation of the synovium of the joint, with subsequent destruction of the articular structure such as cartilage, bone, and adjacent ligaments and tendons [1,2,3].
Popliteal cysts are usually seen secondary to osteoarthritis (OA), RA, and less commonly trauma, infections, and other causes of inflammatory arthritis [4]. Several etiological mechanisms of popliteal cyst have been suggested: (1) enlargement of the gastrocnemius–semimembranosus bursa, which has communication with the joint, (2) rupture of the posterior articular capsule and its transformation to a cyst in a chronic course, and (3) herniation of the posterior articular capsule due to a chronic increase in the intra-articular pressure [5].
Fielding et al. [6], in their study using MRI, reported that popliteal cyst was seen in adult populations at a rate of 4%, with the rate being higher in the elderly population. Andonopoulos et al. [7] reported that popliteal cyst was detected in 47.5% of RA using ultrasonography, only 43.3% of which had been diagnosed clinically. Although cysts present as an asymptomatic mass in most cases, they are also known to cause severe clinical problems such as pseudothrombophlebitis, thrombophlebitis, compartment syndrome, and neuropathy, most of which may need specific treatment such as surgical intervention [8,9,10,11].
A few previous reports have described the complicated popliteal cyst associated with RA [7, 12, 13]. However, since the underling pathophysiology of the disease itself and the particular pathology of popliteal cyst of RA might be quite different from that of OA, optimal surgical approaches and their technical aspect for good clinical outcome should be addressed. In this report, four patients with RA in combination with OA having refractory and complicated popliteal cysts who were successfully treated by means of arthroscopic treatment are described with a brief review of literatures of surgical management of popliteal cyst associated with RA.
Methods
This was a retrospective review of all cases with RA having refractory popliteal cysts that had been performed surgery during 2017–2018 at a single center in South Korea. We have reviewed the cases regarding demographic features, laboratory findings including autoantibodies such as rheumatoid factor (RF) and anti-citrullinated peptide antibody (ACPA), DAS 28-ESR (disease activity score 28-ESR), medications, radiographic findings including MRI, joint fluid analysis, number of intra-articular injection of glucocorticoid 6 months prior to surgery, and clinical outcomes after surgical treatment. The patients were informed that the data of the cases would be submitted for publication and provided their consent. This study was approved by the Institutional Ethics Review Board of Hanyang University Guri Hospital in South Korea.
Search strategy
An electronic literature search was performed using the Medline, Embase, and Scopus databases. Articles written in English from 1960 to 2018 were searched. The following keywords were used along with the Boolean search function: “popliteal cyst” and “rheumatoid arthritis”. Because the scope of the literature review is limited to patients with RA who had been performed surgery for popliteal cyst, we carefully screened for appropriate studies. As a result, a total of nine reports (including one with only abstract available) were reviewed.
Results
A total of four patients were eligible for the current review. Table 1 summarizes details of the cases. The table includes initial clinical characteristics, autoantibodies such as RF and ACPA, DAS 28, medications, radiographic findings including MRI, and clinical outcomes after surgical treatment. All were females and seropositive (RF positive or ACPA positive). DAS28-ESR that are widely used for assessment of disease activity for RA was among 3.1–4.84, which means moderate disease activity except case 3 that showed low disease activity. All cases were combined with OA that represented by Kellgren–Lawrence grade (K–L grade) 2 or 3. Case 1 is described in detail below, which includes patient’s history and physical examination, radiography, MRI, surgical procedure, and arthroscopic and histologic findings. The remaining three cases are described briefly.
Case 1
A 62-year-old woman with 15 years of history of seropositive RA presented with left knee joint discomfort and lower leg swelling. She was taking sulfasalazine 2 g/day, prednisolone 5 mg/day, and subcutaneous golimumab (anti-tumor necrosis factor monoclonal antibody). Intra-articular glucocorticoid injection was performed three times in the affected knee joint over a year, but without improvement. Her lower leg swelling had been aggravated for over 12 weeks, and she had suffered from increased pain with motion and limited knee flexion despite conservative treatment. Physical examination revealed cutaneous erythema, swelling, and tenderness of the left calf. She showed moderate disease activity of DAS28-ESR 4.84, erythrocyte sedimentation rate 110 mm/h, and C-reactive protein of 5.99 mg/dl. Radiologic imaging showed mild joint space narrowing without a significant valgus or varus deformity (K–L grade 2) (Fig. 1). Ultrasonography revealed popliteal cyst with synovial hypertrophy and analysis of joint fluid revealed white blood cell 17,200 with polymorphonuclear (PMN) cell 74%. MRI (fat-suppressed fast spin-echo T2-weighted images) revealed 4.1-cm multiloculated ganglion cysts at the popliteal fossa and a complicated popliteal cyst with leakage to the distal limb through a subcutaneous extension (Fig. 2). The distal leakage extended down to the mid-calf area. The patient was hospitalized to further evaluate the status and prevent further swelling of the lower limb. Fortunately, the patient did not develop severe complications such as compartment syndrome. Arthroscopy-assisted cyst decompression was planned. The operative procedure was conducted using three arthroscopic portals: the standard anterolateral, anteromedial, and the posteromedial portals. Using the posteromedial portal, the opening of the cyst was identified by inferiorly displacing the overlying capsular fold located at the posteromedial side of the medial head of the gastrocnemius. Once the opening had been identified, the capsular fold was resected using basket forceps and an arthroscopic shaver. The valvular opening of the posterior capsule was enlarged to completely resect the capsular fold. The arthroscope was then switched to the posteromedial portal using a switching stick. The arthroscope was advanced further to the posterior and distal aspect which revealed the popliteal cyst consisted of debris and wall septa. The cystic wall was hypervascular and friable, which was different from the popliteal cyst wall in osteoarthritic knee joint (Fig. 3). Careful attention was given when debriding the lateral wall of the popliteal cyst to prevent damage to the adjacent neurovascular structures. Further debridement of the capsule was done down to the leakage area. A biopsy sample was taken from the cystic wall. Histopathological examination showed fibro-hyalinized tissue and plasma cells resulting from active chronic inflammation (Fig. 4). All procedures were performed with a standard 30° arthroscope. The water pump pressure was minimalized throughout the operation (not exceeding 50 mmHg) to prevent any further leakage through ruptured cyst which might cause increased calf pressure (e.g., iatrogenic compartment syndrome of lower leg). The physical status of calf swelling was monitored continuously. In addition, radical synovectomy was performed intra-articularly, especially at the suprapatellar pouch and medial/lateral gutter area. A suction drainage was inserted at the cyst resection site and compressive dressing was applied. This drainage was removed the next day of operation and a full extension splint was applied for 7 days. Immediately after left knee operation, she complained of right knee pain and popliteal area discomfort due to the same complicated popliteal cyst, for which arthroscopic partial cystectomy was performed. Full weight bearing and active–passive motion were permitted from 1 week after surgery. Pain and swelling improved dramatically after surgery and further decreased after hospital discharge. Full range of motion of both knee joints was observed without recurrence of the popliteal cyst at the 12-month follow-up.

Radiologic image showing mild joint space narrowing on left knee joint (arrow) without a significant valgus or varus deformity

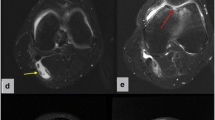
Magnetic resonance images (fat-suppressed fast spin-echo T2-weighted images) showing 4.1-cm sized multiloculated ganglion cysts at the popliteal fossa and complicated popliteal cyst with leakage to the distal limb through a subcutaneous extension (arrows). a Coronal, b sagittal, and c axial images

Popliteal cystic wall consisting of debris and wall septa. The walls were hypervascular and friable, different from the popliteal cyst wall of an osteoarthritic knee joint. The scope was introduced via the posteromedial portal, whereas the arthroscopic shaver was introduced through the standard anterolateral portal (arrow)

Histopathological images showing fibro-hyalinized tissue and plasma cells resulting from active chronic inflammation (hematoxylin and eosin staining, original magnification ×200)
Case 2
A 75-year-old woman with 11 years of history of seropositive RA presented due to swelling of left popliteal fossa and discomfort when bending the knee. The patient had a low activity of RA (DAS28-ESR 3.1) without any other joint involvement except the left knee joint. She took leflunomide 20 mg daily. Simple X-ray of the knee showed OA change with K–L grade 2. MRI revealed the multiloculated cysts without leakage to the distal limb but combined with meniscal tear and ligament damage. Joint fluid analysis revealed white cell count 400 (PMN 45%). She was treated with the intra-articular glucocorticoid injection, but the symptoms recurred within a few days. Arthroscopic cyst excision and debridement of medial meniscus were performed 3 months after the onset of symptoms. After the operation, the patient is under observation for 12 months without recurrence.
Case 3
A 54-year-old-woman with 18 years of history of seropositive RA presented with newly developed swelling of left lower leg. On examination, swelling was observed from the left knee to the ankle and pain was not accompanied. The patient was taking methotrexate 15 mg weekly, prednisolone 5 mg daily, and subcutaneous golimumab. She showed moderate disease activity (DAS28-ESR 4.71) and had no joint symptoms other than left knee. Simple knee X-ray showed OA change with K–L grade 3. MRI revealed popliteal cyst leakage with meniscal and ligament damage of left knee and laboratory investigation of aspirated fluid from cyst revealed white cell count 16,000 (PMN 73%). She underwent intra-articular glucocorticoid injection into the knee joint, but the symptoms recurred. Arthroscopic cystectomy and synovectomy was performed. During the follow-up period of 12 months after surgery, there was no recurrence of popliteal cyst.
Case 4
A 66-year-old woman with 7 years of history of seropositive RA presented with both knee pain. The disease activity of RA was well controlled and patient was taking methotrexate 15 mg weekly, hydroxychloroquine 200 mg daily. Simple knee X-ray revealed bilateral OA with K–L grade 3. MRI revealed septated popliteal cysts with meniscal tear in both knees and joint fluid analysis of left knee showed white cell count 90 (PMN 28%). Despite intra-articular glucocorticoid injection into both knee joints, symptoms persisted. Arthroscopic cyst excision and partial medial meniscectomywere performed on both knees. After the operation, the patient is under observation for 12 months without recurrence.
Discussion
In the present study, four RA patients (six knees) in combination with OA having refractory popliteal cysts have successfully been treated with arthroscopic operation including cystectomy, synovectomy, and/or correction of valvular communication of cysts. All cases have been actively treated with DMARDs and/or biologics such as golimumab for RA, by which disease activity of RA except knees was relatively well controlled.
Popliteal cysts are generated by the communication of the bursas around the knee joint. During knee flexion and extension, a pressure difference occurs between the intra-articular and intracyst regions, leading to fluid collection as a check-valve mechanism [14]. Popliteal cyst is usually asymptomatic; however, posterior knee pain, knee stiffness, swelling, palpable mass, and discomfort can occur with the cyst alone.
RA is a type of autoimmune disease that causes chronic inflammation in the whole body, in which the synovium is the primary target particularly. As the synovitis becomes more severe, the tissues become friable and may be easily torn in cases of popliteal cyst. If the extra-articular leakage is small and chronic, the patient may only present symptoms of swelling and/or edema of the lower extremity. However, if the leakage is acute and large in amount, this may result in serious complications such as compartment syndrome [8,9,10,11]. In cases of popliteal cyst rupture, extravasation of degraded blood products and inflammatory synovial fluid may cause irritation and inflammation of the surrounding fascia, muscles, and subcutaneous tissues. Liao et al. [4] have reported that RA was the second most common disease that were associated with popliteal cyst (20.6%) following OA (50.6%), which was investigated by ultrasonography. However, they have also emphasized that cases of ruptured popliteal cyst were more frequent in the inflammatory diseases (66.7%) such as RA than the degenerative one (33.3%).
Although various conservative treatments for popliteal cysts with RA could be successfully, surgical interventions may be required for refractory or/and complicated cysts as presented in this report. Optimal RA disease activity control is crucial to prevent recurrence.
One of the important implications of this report is that prompt evaluation should be conducted when lower leg swelling or edema develops in RA patients, as shown in case 1. All four cases in the present report were postmenopausal females and all six knees were combined with OA changes such as K–L grade 2 or 3, and meniscal/ligament damage on MRI. Therefore, underlying pathophysiology of popliteal cysts in the cases might result from that of OA. However, unlike the cystic wall of popliteal cyst in patients with only OA pathology, the popliteal cyst wall in RA patients tends to be hypervascular and inflammatory, which can possibly make the walls friable, leading to leakage and rupture. With extension of pain and swelling to the lower leg especially with acute development, popliteal cystic wall leakage and subsequent rupture should be considered in this subgroup of RA patients.
Since popliteal cyst is most frequently associated with OA, many reports regarding to treatment options have been focused on OA, with relatively few reports related to RA. In our literature review (Table 2) [15,16,17,18,19,20,21,22,23], which included nine reports, surgical interventions such as open synovectomy/cystectomy, arthroscopic synovectomy/cystectomy and biomechanical valve excision have been reported with overall successful outcomes. However, Ushiyama et al. [20] reported a case who had neurologic complication even after emergency fasciotomy, emphasizing the importance of early detection and intervention of such complicated popliteal cyst rupture for preventions of life-long neurologic impairments.
In conclusion, arthroscopic intervention which allows the surgeons to perform radical debridement, synovectomy, biomechanical valve excision, and/or cystectomy in a delicate nature should be considered in patients with refractory and complicated popliteal cysts associated with RA or RA in combination with OA.
References
Veale DJ, Orr C, Fearon U (2017) Cellular and molecular perspectives in rheumatoid arthritis. Semin Immunopathol 39:343–354
Gibofsky A (2014) Epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis: a synopsis. Am J Manag Care 20:S128–S135
Gibofsky A (2012) Overview of epidemiology, pathophysiology, and diagnosis of rheumatoid arthritis. Am J Manag Care 18:S295–S302
Liao ST, Chiou CS, Chang CC (2010) Pathology associated to the Baker’s cysts: a musculoskeletal ultrasound study. Clin Rheumatol 29:1043–1047
Perri JA, Rodnan GP, Mankin HJ (1968) Giant synovial cysts of the calf in patients with rheumatoid arthritis. J Bone Jt Surg Am 50:709–719
Fielding JR, Franklin PD, Kustan J (1991) Popliteal cysts: a reassessment using magnetic resonance imaging. Skelet Radiol 20:433–435
Andonopoulos AP, Yarmenitis S, Sfountouris H, Siamplis D, Zervas C, Bounas A (1995) Baker’s cyst in rheumatoid arthritis: an ultrasonographic study with a high resolution technique. Clin Exp Rheumatol 13:633–636
Moon SH, Im S, Park GY, Moon SJ, Park HJ, Choi HS et al (2013) Compressive neuropathy of the posterior tibial nerve at the lower calf caused by a ruptured intramuscular baker cyst. Ann Rehabil Med 37:577–581
Dash S, Bheemreddy SR, Tiku ML (1998) Posterior tibial neuropathy from ruptured Baker’s cyst. Semin Arthritis Rheum 27:272–276
Hamlet M, Galanopoulos I, Mahale A, Ashwood N (2012) Ruptured Baker’s cyst with compartment syndrome: an extremely unusual complication. BMJ Case Rep 2012:bcr2012007901
Kim JS, Lim SH, Hong BY, Park SY (2014) Ruptured popliteal cyst diagnosed by ultrasound before evaluation for deep vein thrombosis. Ann Rehabil Med 38:843–846
Hooper JC, Brookler M (1971) Popliteal cysts and their rupture in the rheumatoid arthritis simulating thrombophlebitis. Med J Aust 1:1371–1373
Colamussi V, Benini F (1970) Rupture of popliteal cysts and dissecting calf cysts in patients with rheumatic arthritis. Arcisp S Anna Ferrara 23:473–493
Lindgren PG, Rauschning W (1980) Radiographic investigation of popliteal cysts. Acta Radiol Diagn (Stockh) 21:657–662
Jayson MI, Dixon AS, Kates A, Pinder I, Coomes EN (1972) Popliteal and calf cysts in rheumatoid arthritis. Treatment by anterior synovectomy. Ann Rheum Dis 31:9–15
Kirkham B, Churchill M, Dasgupta B, Wedderburn L, Spencer J, Macfarlane DG (1991) Anterolateral rupture of popliteal cysts in rheumatoid arthritis. Ann Rheum Dis 50:187–188
Kanekasu K, Nagashima K, Yamauchi D, Yamakado K (1997) A clinical study of arthroscopic cystectomy on popliteal cysts associated with rheumatoid arthritis. Ryumachi (Rheumatism) 37:761–769
Tanaka N, Yamamura M, Ishii S (1999) Anterior arthroscopic synovectomy plus capsuloplasty with a pedicle graft for the treatment of rheumatoid popliteal cysts. J Rheumatol 26:1481–1485
Lee JH, Jun JB, Lee HS, Yun HR, Choi CH, Park SB et al (2000) Posterior tibial neuropathy by a Baker’s cyst: case report. Korean J Intern Med 15:96–98
Ushiyama T, Kawasaki T, Matsusue Y (2003) Anterior tibial compartment syndrome following rupture of a popliteal cyst. Mod Rheumatol 13:189–190
Mikashima Y, Momohara S, Tomatsu T (2004) The pathology and evaluation of surgical treatment in a ruptured giant popliteal/crural cyst associated with rheumatoid arthritis. Mod Rheumatol 14:453–458
Ravlic-Gulan J, Gulan G, Novak S, Sestan B (2009) Rapid recurrence of a giant popliteal cyst in a patient with rheumatoid arthritis. J Clin Rheumatol 15:300–302
Adiyeke L, Bilgin E, Duymus TM, Ketenci IE, Ugurlar M (2017) Giant Baker’s cyst associated with rheumatoid arthritis. Case Rep Orthop 2017:4293104
Author information
Authors and Affiliations
Contributions
JHY performed the surgery. JHY and HSL devised the project and the main conceptual ideas. HHK, JKL, and SYB aided in the interpreting the results and worked on the manuscript. JHY and HHK wrote the paper with input from all authors. JHY and HSL critically revised the manuscript at all stages of its production, final approval of manuscript, and review of literature. All authors discussed the outline and commented on the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Authors; Jae-Hyuk Yang, Hyuk-Hee Kwon, Jin Kyu Lee, So Young Bang, and Hye-Soon Lee declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Yang, JH., Kwon, HH., Lee, J.K. et al. Successful arthroscopic treatment of refractory and complicated popliteal cyst associated with rheumatoid arthritis in combination with osteoarthritis: case series and literature review. Rheumatol Int 39, 2177–2183 (2019). https://doi.org/10.1007/s00296-019-04278-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-019-04278-9