
Abstract
The aim of this study was to evaluate quality of life (QOL) in patients with ankylosing spondylitis (AS) and to determine the relationships between QOL and clinical variables including spinal mobility, disease activity and functional status. Forty-eight adult patients who fulfilled the modified New York criteria for AS were included in the study. After detailed physical examination, disease-specific instruments: the Bath ankylosing spondylitis disease activity index (BASDAI) and the Bath ankylosing spondylitis functional index (BASFI) were applied. QOL was assessed using short form-36 (SF-36). The mean age of the patients was 37.0 ± 9.7 years and the mean duration of symptoms was 11.7 ± 8.4 years. Most affected domains of SF-36 were bodily pain, vitality, and physical role, respectively. No significant correlations were found between SF-36 subgroup scores and chest expansion, wall–tragus distance, chin–sternum distance, and floor–finger tip distance. Only modified Schober correlated with two SF-36 domains: physical role and bodily pain. BASDAI and BASFI scores had significant negative correlations with all SF-36 domains except for general health. Identification of QOL in patients with AS is very important in evaluation of illness-related sufferings and development of new management strategies.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disease which mainly affects spinal joints and adjacent structures leading to progressive and ascending bony fusion of spine [1]. The cardinal complaints of patients with AS are pain, stiffness, and fatigue, resulting in various degree of functional limitation [2, 3]. Limitations in physical functioning may influence the ability to remain in employment and participate in leisure and domestic activities. The ability to fulfill social roles in family and society may thereby be restricted, thus influencing the person’s emotional state [4]. All these factors may have their own or combined negative impacts on quality of life (QOL) in AS patients.
Health-related QOL measures objectively reflects the actual effect of the disease on an individual and the extent of suffering [5, 6]. Knowing which aspects of QOL are most affected by a particular illness can help researchers prioritize their efforts and help clinicians by identifying prevalent illness-related problems or concerns that may not always be recognized or addressed in the medical encounter [7]. The medical outcomes study short form-36 health survey (SF-36), a generic QOL instrument, has been widely used for rheumatologic disorders [8–10]. In previous studies, assessing the health-related QOL of patients with AS, SF-36 is the most commonly used measurement technique [2–4, 7, 10–13]. In these studies, the researchers investigated mostly relationship between QOL and disease activity or functional status of the patients [11–14]. Nevertheless, there are only a few studies focused on the relationship between spinal mobility and SF-36 domains in patients suffering from AS [13, 15].
The aim of this study was to figure out which aspects of QOL sinks due to the disease in AS patients and to determine the relationship between QOL and clinical variables including spinal mobility, disease activity and functional status.
Materials and methods
Forty-eight adult patients who fulfilled the modified New York criteria for AS were randomly included in the study [16]. Patients with severe concomitant diseases such as cancer or psychiatric disorders were excluded. The demographic data including age, gender, education level, employment status, smoking status, physical activity level, family history, duration of symptoms of the patients and peripheral articular involvement were recorded. In physical examination modified Schober, wall–tragus distance, chin–sternum distance, floor–finger tip distance and chest expansion were measured. All measurements were performed at noontime and all patients were assessed by the same physician. Sacroiliitis was evaluated on standardized anterio-posterior sacroiliac joint radiography. Erythrocyte sedimentation rate (ESR) was determined by using the standard Westergren method (normal range 0–20) and serum C-reactive protein (CRP) by the turbidimetric method (normal range 0–5).
The Bath ankylosing spondylitis disease activity index (BASDAI) was used to evaluate disease activity [17]. This self-administered instrument consists of six questions dealing with five major symptoms relevant to AS: fatigue, spinal pain, joint pain/swelling, areas of localized tenderness, and morning stiffness. Morning stiffness is measured in terms of both severity and duration. Functional status of the patients were assessed by the Bath ankylosing spondylitis functional index (BASFI) [18]. The BASFI consists of eight questions relating to functional anatomy of patients, and two questions that assess the patient’s ability to cope with everyday life. Each questions of the BASDAI and BASFI is answered on a 10 cm visual analog scale which allows maximum reliability, and sensitivity to change and improve the capacity of an index to elicit a range of responses across the entire scale (0 = best, 10 = worst score). It was shown that the Turkish versions of these indexes were reliable and valid [19, 20].
In order to estimate the health-related quality of life, all patients completed the Turkish version of SF-36 [21]. This self-administered questionnaire evaluates problems experienced during the last 4 weeks in eight domains of QOL: physical functioning, role limitation due to physical problems, role limitation due to emotional problems, bodily pain, social functioning, mental health, vitality, and general health perception. The response choices in the role functioning scales are dichotomous (yes/no). The other items have three to six response choices. The raw scores were coded and recalibrated following standard guidelines, and the items were summed and transformed to the eight 0–100 scales; higher scores indicates better health conditions [22].
All statistical analyses were performed by using the SPSS 11.5 for Windows package program. Descriptive data are presented as mean ± standard deviation for continuous variables and as frequencies and percentages for categorical variables. The Pearson correlation test was applied to test for correlations. Multivariate linear regression analysis was performed to analyze relationship between clinical variables and QOL. Statistical significance was determined at p value <0.05.
Results
Forty-eight patients (44 males and 4 females) with a mean age of 36.9 ± 9.4 years (17–63) were enrolled in this study. Patients’ characteristics are presented in Table 1. All patients had 5 years or more of formal education, 42% of whom were university graduates. Almost all patients were employed; only one patient had to quit working due to the functional limitations of the disease. Sixteen (33%) patients reported family history of rheumatologic diseases and 29 (60%) patients were current smokers. None of the patients had peripheral articular involvement. The mean value of BASDAI score was 4.4 ± 2.0 (0.9–9.5) and BASFI score was 2.9 ± 2.4 (0–10). Twenty-four (%50) patients had BASDAI score ≥4. ESR and CRP levels were higher than normal values in 14 (29%) and 36 (75%) patients, respectively.
There were significant correlations between symptom duration and modified Schober (p < 0.001), wall–tragus distance (p = 0.01), chin–sternum distance (p < 0.001), floor–finger tip distance (p < 0.001), and chest expansion (p < 0.001). BASDAI and BASFI scores did not correlate with any of these physical examination measurements. Of the laboratory parameters, while ESR correlated significantly with BASDAI (p = 0.001) and BASFI scores (p = 0.005), disease activity (p = 0.074) and functional status index scores (p = 0.151) were not related to serum CRP levels.
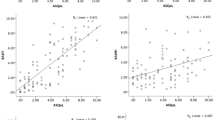
The mean scores for SF-36 domains are presented in Table 2. Most affected domains of SF-36 in AS patients were bodily pain (44.6 ± 20.9), vitality (49.6 ± 24.5), and physical role (53.1 ± 36.3). Age and body mass index had no significant correlation with SF-36 domains. Duration of symptoms has been only correlated with bodily pain (p = 0.050). No significant correlations were found between SF-36 subscale scores and chest expansion, wall–tragus distance, chin–sternum distance and floor–finger tip distance. Only modified Schober correlated with two SF-36 domains: physical role (p = 0.047) and bodily pain (p = 0.007). BASDAI and BASFI scores had significant negative correlations with all SF-36 domains except for general health. ESR correlated with all domains of SF-36 except for general health and mental health. CRP negatively correlated with vitality (p = 0.013), bodily pain (p = 0.016), role emotional (p = 0.022) and social function (p = 0.048) domains of SF-36 (Table 3).
Regression models were constructed to identify variables associated with the most affected SF-36 domains. According to multiple regression analysis (Table 4), it has been found out that BASFI (p < 0.001) and modified Schober (p < 0.001) were associated with physical role. The most significant correlation with vitality was BASDAI score (p < 0.001). And finally, regression model with bodily pain as dependent variable revealed three contributing variables BASDAI (p < 0.001), modified Schober (p = 0.012) and ESR (p = 0.006), explaining 51% of total variance.
Discussion
Individuals with chronic diseases usually perform activities of daily life insufficiently. Functional weakness, symptoms of the disease and deterioration of physical condition in these patients make adaptation to therapy more difficult, weaken the will to take care of oneself, and cause various psychological problems. Owing to the combination of all these factors, the QOL of the individuals may be affected negatively [23]. Since the burden of illness in AS results from pain and reduced function, the studies investigating the QOL of these patients increased in recent years [3, 4, 10–15]. However, the relationship between spinal mobility and QOL is not well established as the relationship between SF-36 domains and disease activity or functional status in patients with AS.
Limitations of spinal mobility generally worsen with age and longer disease duration [14, 24]. The present study confirms the existence of such relationships between all physical examination measurements and duration of disease or symptoms. Like in the previous studies, no significant correlations were found between spinal mobility measures and disease activity. However, dissimilarly, any of these measures had no association with BASFI [11, 13]. The discriminative power of ESR and CRP do not comprehensively represent the process of disease in AS. But there is some evidence for an association of ESR and CRP with disease activity [25]. In a previous study, it was reported that clinical measures of disease activity and functional disability correlated more with ESR than with other laboratory variables [14]. According to our results, only ESR correlated with BASDAI and BASFI scores. In fact, recent studies concluded that neither CRP nor ESR is superior in assessing disease activity [25, 26].
In order to examine the self-reported health status in patients, SF-36 instrument was used in this study. The subgroups of SF-36 enable us to evaluate which aspects of the QOL are affected by the disease. A concern is that the broad scope of the generic instruments might not adequately reflect health status in populations with specific disorders. However, similar to another study, it was found that the disease-specific and the generic instrument correlated well (BASDAI and SF-36 bodily pain, BASFI and SF-36 physical functioning) [4]. In the present study most affected domains of SF-36 in AS patients were bodily pain, vitality and physical role, respectively. On the other hand, patients received the highest score from emotional role. These findings are consistent with previous studies indicating the physical domain was significantly more impaired than the mental one [3, 11, 13]. Mental health, limitations imposed by emotional difficulties and social relationships were usually problems for only a minority of patients with AS [7, 10, 11]. In a study, 175 patients with AS of broad range of durations were asked to rate the presence and importance of problems in 23 aspects of QOL, including symptoms, disability, mood, relations with others, and concerns about the treatments and the future. Besides, participants completed SF-36. As a result, the most prevalent QOL concerns included stiffness (90.2%), pain (83.1%), fatigue (62.4%), poor sleep (54.1%), concerns about appearance (50.6%), worry about the future (50.3%), medication side effects (41%). Of the domains of SF-36 pain, energy/fatigue, and general health perceptions were the most severely affected, mental health, role limitations due to emotional problems and social functioning were least affected [7]. Similarly, Ozgul et al. [3] reported that patients enrolling in their study received the highest and lowest scores from social functioning and physical role limitation, respectively. Also in another study, it was shown that physical role and bodily pain were the most significantly affected SF-36 subgroups, whereas mental health and physical function were least affected in patients with AS [13].
BASDAI and BASFI with proven reliability and validity are commonly used in the clinical observations of AS patients [17, 18]. In this study, it was detected that BASDAI and BASFI scores had significant negative correlations with all SF-36 domains except for general health. Similarly, Vesović-Potić and et al. [13] reported that BASDAI correlated with all SF-36 domains except for emotional role and BASFI correlated with physical function, role physical, bodily pain, general health, vitality and mental health. In contrast to these findings, Turan et al. [12] showed that among SF-36 subgroups, BASDAI had a significant correlation only with general health and a negatively significant correlation has been identified only between BASFI and emotional role.
In the relevant literature, there are very few studies assessing the relationship between QOL and spinal mobility measures [13, 15]. In a very recent one, it was shown that spinal mobility measures were mostly correlated with physical domains of QOL in patients with AS. While occiput–wall distance was negatively correlated with two SF-36 domains, physical function and mental health; chest expansion correlated with general health and emotional role. Furthermore, they have shown that BASMI had negative correlation with SF-36 physical function and general health subscales. However, they could not confirm a significant association of any spinal mobility measure with four SF-36 domains: physical role, bodily pain, social function and vitality [13]. In the present study, there were no significant correlations between SF-36 domains and measurements of chest expansion, wall–tragus distance, chin–sternum distance and floor–finger tip distance. Only modified Schober correlated with two SF-36 domains: physical role and bodily pain. Like in a previous study, no relationship between spinal mobility status and mental health were detected [15].
Physical role describes the problems at work or in other daily life activities due to the deterioration of physical health [27]. In multiple regression analysis, it has been found out that BASFI and modified Schober were the main factors associated with physical role, suggesting that functional disability and decrease in spinal mobility leads to deterioration of physical role in AS patients. Similarly, in a previous study, BASFI was presented as the main associated factor with health-related QOL [11]. Vesović-Potić et al. [13] developed a regression model to identify variables associated with physical function domain of SF-36 and reported that BASFI score was the independently associated factor. In this study, it was determined that the most closely related variable with vitality was BASDAI, and 51% of total variance of bodily pain was explained with BASDAI, modified Schober and ESR. These results indicate that as the disease activity increases, the bodily pain and tiredness of patients increases as well. In a previous study in which 51 patients’ QOL was evaluated by Nottingham Health Profile, it was suggested that the most important determinants in self-reported QOL were the levels of functional disability and disease activity [14].
Finally, the limitations of this study are its cross-sectional design and relatively small number of participants. Furthermore, similar to most of the previous studies focusing on QOL of AS patients, the patient group examined in this study was also very heterogeneous concerning duration of the symptoms and activity of the disease [4, 7, 11–14]. Ariza-Ariza et al. reported that the wide ranges of the scores of the disease-related variables reflect the broad spectrum of their population with AS. However, they suggested that the broad spectrum of 92 patients enrolling in the study supports the idea that they represent the entire population [11]. In another study which assessed a relatively larger number of patients (175 patients) with varying durations of AS, heterogeneity of the group was mentioned as the strength of the study [7]. Like in most rheumatic diseases, the severity of symptoms in AS varies greatly among patients. Besides, symptoms in the same individual could periodically flare in the course of disease [2]. Functional limitations in early AS may be closely related to symptom severity and factors that modify symptoms, whereas functional limitations in long-standing AS may be more closely related to cumulative factors leading to spinal fusion and long-term structural damage [28]. Hence, high variability in the course of disease makes a general deduction of QOL in AS very difficult. On the other hand, QOL defined as a subjective concept that not only encompasses the symptoms, but also the consequences of a disease such as impairment in activities of daily life [29]. Therefore, whatever the reason for loss of spinal mobility or functional disability is, inflammatory pain or ankylosis, its impact on the individual’s full and productive life is important. Further, longitudinal studies are required to identify the definitive relationship between spinal mobility and QOL in a larger sample of patients suffering from AS.
In conclusion, it is obvious that there is a significant impairment especially in physical components of QOL in patients with AS. Recognizing these potential limitations, this study demonstrates that in addition to BASDAI and BASFI scores, modified Schober index significantly correlated with physical role and bodily pain domains of SF-36. It is important for clinicians to be aware of complicated relationships between clinical variables and QOL. Current management strategies should focus on reducing disease activity, improving lumbar spinal mobility and functional status in AS.
References
Boulware DW, Arnett FC, Cush JJ, Bennett RM, Mielants H, De Keyser F, Veys EM (2003) The seronegative spondyloarthropathies. In: Koopman WJ, Boulware DW, Heudebert GR (eds) Clinical primer of rheumatology. Lippincott, Williams and Wilkins, Philadelphia, pp 127–163
Ward MM (1998) Quality of life in patients with ankylosing spondylitis. Rheum Dis Clin North Am 24:815–827
Ozgul A, Peker F, Taskaynatan MA, Tan AK, Dinçer K, Kalyon TA (2006) Effect of ankylosing spondylitis on health-related quality of life and different aspects of social life in young patients. Clin Rheumatol 25:168–174
Dagfinrud H, Mengshoel AM, Hagen KB, Loge JH, Kvien TK (2004) Health status of patients with ankylosing spondylitis: a comparison with the general population. Ann Rheum Dis 63:1605–1610
Fitzpatrick R (1993) The measurement of health status and quality of life in rheumatologic disorders. Baillieres Clin Rheumatol 7:297–317
Ortiz Z, Shea B, Garcia Dieguez M, Boers M, Tugwell P, Boonen A, Wells G (1999) The responsiveness of generic quality of life instruments in rheumatic diseases. A systematic review of randomized controlled trials. J Rheumatol 26:210–216
Ward MM (1999) Health-related quality of life in ankylosing spondylitis: a survey of 175 patients. Arthritis Care Res 12:247–255
Brazier JE, Harper R, Jones NM, O’Cathain A, Thomas KJ, Usherwood T, Westlake L (1992) Validating the SF-36 health survey questionnaire: new outcome measure for primary care. BMJ 305:160–164
Husted JA, Gladman DD, Farewell VT, Long JA, Cook RJ (1997) Validating the SF-36 health survey questionnaire in patients with psoriatic arthritis. J Rheumatol 24:511–517
Chorus AM, Miedema HS, Boonen A, Van der Linden S (2003) Quality of life and work in patients with rheumatoid arthritis and ankylosing spondylitis of working age. Ann Rheum Dis 62:1178–1184
Ariza-Ariza R, Hernández-Cruz B, Navarro-Sarabia F (2003) Physical function and health-related quality of life of Spanish patients with ankylosing spondylitis. Arthritis Rheum 49:483–487
Turan Y, Duruöz MT, Cerrahoglu L (2007) Quality of life in patients with ankylosing spondylitis: a pilot study. Rheumatol Int 27:895–899
Vesović-Potić V, Mustur D, Stanislavljević D, Ille T, Ille M (2009) Relationship between spinal mobility measures and quality of life in patients with ankylosing spondylitis. Rheumatol Int 29:879–884
Bostan EE, Borman P, Bodur H, Barça N (2003) Functional disability and quality of life in patients with ankylosing spondylitis. Rheumatol Int 23:121–126
Hamdi W, Azzouz D, Saadellaoui K, Daoud L, Kochbati S, Ben Hamida A, Zouari B, Kochir MM (2007) Correlations between Bath ankylosing spondylitis metrology index (BASMI), functional, structural, enthesopathy, disease activity index, and quality of life in 120 patients with ankylosing spondylitis. Ann Rheum Dis 66(Suppl 2):398
Van der Linden S, Valkenburg HA, Cats A (1984) Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 27:361–381
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A (1994) A new approach to defining disease status in AS: the Bath ankylosing spondylitis disease activity index. J Rheumatol 21:2286–2291
Calin A, Garrett S, Whitelock H, Kennedy LG, O’Hea J, Mallorie P, Jenkinson T (1994) A new approach to defining functional ability in AS: the development of the Bath ankylosing spondylitis functional index. J Rheumatol 21:2281–2285
Akkoç Y, Karatepe AG, Akar S, Kirazlı Y, Akkoç N (2005) A Turkish version of the Bath ankylosing spondylitis disease activity index: reliability and validity. Rheumatol Int 25:280–284
Yanık B, Gürsel YK, Kutlay Ş, Ay S, Elhan AH (2005) Adaptation of the BASFI to the Turkish population, its reliability and validity: functional assessment in AS. Clin Rheumatol 24:41–47
Koçyiğit H, Aydemir Ö, Fişek G, Ölmez N, Memiş A (1999) Kısa Form-36 (SF-36)’nın Türkçe versiyonunun güvenilirliği ve geçerliliği. Romatizmal hastalığı olan bir grup hasta ile çalışma. İlaç ve Tedavi Dergisi 12:102–106
Ware JE Jr, Sherbourne CD (1992) The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 30:473–483
Hays RD, Hahn H, Marshall G (2002) Use of the SF-36 and other health-related quality of life measures to assess persons with disabilities. Arch Phys Med Rehabil 83(Suppl 2):S4–S9
Martindale J, Smith J, Sutton CJ, Grennan D, Goodacre L, Goodacre JA (2006) Disease and psychological status in ankylosing spondylitis. Rheumatology (Oxford) 45:1288–1293
Ruof J, Stucki G (1999) Validity aspects of erythrocyte sedimentation rate and C-reactive protein in ankylosing spondylitis: a literature review. J Rheumatol 26:966–970
Spoorenberg A, van Heijde D, Klerk E, Dougados M, de Vlam K, Mielants H, van der Tempel H, van der Linden S (1999) Relative value of erythrocyte sedimentation rate and C-reactive protein in assessment of disease activity in ankylosing spondylitis. J Rheumatol 26:980–984
Ware JE Jr (2000) SF-36 health survey update. Spine (Phila Pa 1976) 25:3130–3139
Ward MM, Weisman MH, Davis JC Jr, Reveille JD (2005) Risk factors for functional limitations in patients with long-standing ankylosing spondylitis. Arthritis Rheum 53:710–717
Cella D, Nowinski CJ (2002) Measuring quality of life in chronic illness: the functional assessment of chronic illness therapy measurement system. Arch Phys Med Rehabil 83(Suppl 2):S10–S17
Conflict of interest statement
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Özdemir, O. Quality of life in patients with ankylosing spondylitis: relationships with spinal mobility, disease activity and functional status. Rheumatol Int 31, 605–610 (2011). https://doi.org/10.1007/s00296-009-1328-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-009-1328-2