
Abstract
PFAPA is a periodic fever disease, of unknown etiology, characterized by aphthous stomatitis, pharyngitis and cervical adenitis. To inquire whether genes implicated in other auto-inflammatory diseases might be involved in its pathogenesis, predominant mutations in the genes causing familial Mediterranean fever, TNF receptor-associated periodic fever syndrome, Crohn’s disease and Muckel–Wells syndrome were analyzed in PFAPA patients. Patients (n = 57) with PFAPA, according to previously published criteria were recruited, at the Meyer Children Hospital during 2006–2007. Clinical information was complemented during physicians–parents encounter. Predominant mutations in MEFV, TNF1rA, CARD15/NOD2 and NLRP3 genes were tested. Mean age at diagnosis was 30.64 ± 16.4 months. Boys (n = 33; 58%) were diagnosed earlier than girls (n = 21; 42%) at 26.18 ± 13.83 and 36.41 ± 18.32 months, respectively (P = 0.05). Fifteen patients (27%) carried an MEFV mutation; two patients (3.6%) a CARD15 mutation, one patient (1.8%) a variance in TNF1rA and another had both an MEFV and a CARD15 mutation. Clinical symptoms were equally manifested in carriers and non-carriers. The high carrier rate of MEFV mutations in our PFAPA cases compares well with that of the general population in Israel. It is debated whether MEFV mutations, when mediated by the presence of additional modifiers, may expose a transient fever condition, namely PFAPA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Periodic fever syndromes refer to a group of auto-inflammatory conditions sharing similar symptoms and characterized by recurrent unprovoked inflammation in the absence of infection [1]. These diseases primarily include familial Mediterranean fever (FMF), TNF receptor-associated periodic fever syndrome (TRAPS), hyperimmunoglobulinaemia D (HIDS), cryopyrin-associated periodic syndrome (CAPS) including familial cold auto-inflammatory syndrome (FCAS), Muckle–Wells syndrome (MWS), neonatal onset multi-system inflammatory disease (NOMID)/chronic infantile neurological cutaneous and articular syndrome (CINCA) [2] and periodic fever with aphthous stomatitis, pharyngitis and cervical adenitis (PFAPA) syndrome. Crohn’s disease, although not clustered as one of the above group of diseases, is a chronic, relapsing inflammatory disease of the gastrointestinal tract [3].
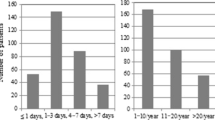
Except for PFAPA, the pathogenesis and the genetic basis of most of auto-inflammatory diseases is known. PFAPA, as described by Marshall et al. (1987, 1989) [4, 5] is a clinically diagnosed condition of unknown cause, characterized by sudden onset of fever, which persists for 4–5 days and resolves spontaneously. After few weeks the cycle recommences [6]. The clinical symptoms include fever at young age, on average 2–3 years of age, pharyngitis, cervical lymphadenopathy and aphthous stomatitis. Less common symptoms include arthralgia, gastrointestinal disturbances and rash [7, 8]. Laboratory testing during febrile episodes may reveal mild leukocytosis and mild elevations in immunoglobulin A, G and M. Children with PFAPA have elevated levels of the proinflammatory mediators interleukin (IL)-1β, IL-6, tumor necrosis factor (TNF)-α and IL 12p70 between attacks, and increased levels of IL-6 and interferon-γ during fever episodes [6].
Only few studies inquired unto the genetic basis of PFAPA. Mutations in MEFV (the gene associated with FMF) and CARD15/NOD2 (the gene associated with Crohn’s disease) were not found to be over-represented in PFAPA syndrome [9, 10].
In an attempt to claim a plausible genetic contribution to PFAPA syndrome, predominant mutations in MEFV, CARD15/NOD2, TNFr1A and NLRP3 were studied in patients diagnosed with PFAPA syndrome.
Patients and methods
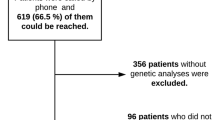
Children with PFAPA were carefully selected based on established clinical criteria proposed by Marshal et al. [4]. Inclusion criteria were remitting episodes of high fever lasting 3–5 days, in the absence of upper respiratory tract infection with at least one of the following clinical signs: pharyngitis, cervical lymphadenitis and aphthous stomatitis in an otherwise normal developed child [5]. Children with suspected familial Mediterranean fever (FMF), Behcet disease and cyclic neutropenia were excluded from the study. All patients were recruited at the Pediatric Rheumatology clinic, Meyer Hospital of Children, during 2006–2007. Parents were invited to include their PFAPA diagnosed children in the study and to sign inform consent forms as customary. Clinical information was complemented during physicians–parents encounter and a blood sample was drawn for molecular testing.
Genetic testing
PCR and RFLPs for the predominant mutations in MEFV, TNF1A, CARD15/NOD2 and NLRP3 genes were performed.
MEFV mutations
Predominant mutations in MEFV gene, namely, M694V, V726A, E148Q M694I and M680I were determined as described by Gershoni-Baruch et al. [11]. The predominant mutations in MEFV gene were studied based on the ethnic descent of individuals tested as published earlier by Gershoni-Baruch et al. [12].
CARD15/NOD2 mutations
Three predominant mutations in CARD15/NOD2, known as the LfinsC1007P, R702W and G908R were tested. PCR for LfinsC1007P was performed using forward 5′-GGCTAACTCCTGCAGTCTCT-3′ and reverse 5′-GGAGAGCTAAAACAGGCCTG-3′ primers yielding a product of 205 bp. Restriction by NLAIV separated the mutant and the wild-type alleles. PCR for R702W was performed using forward 5′-TTCAGATCACAGCAGCCTTC-3′ and reverse 5′-GGTGCAGCTGGCGGGATGG-3′ primers yielding a product of 170 bp. Restriction by MspI separated the mutant and the wild-type alleles. PCR for G908R was performed with mismatched forward 5′-TTTGGCCTTTTCAGATTCC*TGG-3′ and reverse 5′-CTCTTCACCTGATCTCC-3′ primers yielding a product of 149 bp. Restriction by NciI separated the mutant and the wild-type alleles.
TNFr1A mutations
Two predominant mutations in TNFRSFA1, known as P46L and R92Q were tested. PCR was performed using forward 5′-TGTGTTCTCACCCGCAGCCTAAC-3′ and reverse 5′-CTGAGGCCAAGCCCTCTC-3′ primers yielding a product of 574 bp. Restriction by MspI separated the mutant and the wild-type alleles of both the P46L and the R92Q mutation.
NLRP3
One predominant mutation in NLRP3, known as L353P was tested. PCR was performed using forward 5′-GAGGCCTCTCTGCTCATCAC-3′ and reverse 5′-CCATCTGCTGTTTCAGTCCA-3′ primers yielding a product of 253 bp. Restriction by BstnI separated the mutant and the wild-type alleles.
Statistical analysis
To detect differences between genetic, demographic and clinical variables, χ2 and t test analyses were used when appropriate.
Results
Table 1 describes the demographic and clinical manifestation of 57 children with PFAPA. The cohort consisted of 33 (58%) boys and 24 (42%) girls. The mean age at onset was 30.64 ± 16.54 months. Mean duration of follow-up/illness was 6.47 ± 3.0 years. Most patients were non-Ashkenazi Jews predominantly of North African descent. Symptoms noted, other than recurrent pharyngitis, were cervical lymphadenitis (25; 43.8%), abdominal pain (20; 35.1%) and aphthous stomatitis (19; 33.3%).
Predominant mutations in MEFV were found in 16 (28.1%) children of whom nine carried the M694V mutation, five carried the V726A mutation and two were E148Q heterozygotes. Mutations in CARD15 were detected in three (5.2%) children (one carried the G908R mutation and two had the R702W mutation). One (1.8%) child carried the R92Q mutation in TNFr1A and none had the predominant L353P NLRP3 gene mutation (Table 2).
Clinical symptoms (pharyngitis, aphthous stomatitis, abdominal pain and cervical adenitis) were equally manifested between carriers and non-carriers. Boys were diagnosed earlier than girls (26.18 ± 13.83 and 36.41 ± 18.32 months, respectively, P = 0.05) (Table 3). However, carriage of any mutation was not associated with earlier age at diagnosis and/or any of the clinical manifestations evaluated.
Discussion
Of the 57 children diagnosed with PFAPA according to established criteria [4, 5], 16 (28.1%) carried one of the common mutations in MEFV, the gene implicated in FMF. FMF, the most common genetic auto-inflammatory disease in Israel, is an autosomal recessive disorder characterized by multiple attacks of serosal inflammation. It affects primarily people of Mediterranean origin, Sephardic Jews, Armenians, Arabs and Turks [13, 14]. The overall carrier frequency is extremely high in all ethnic groups of the Israeli population and varies from 1:3.5 to 1:4.7 for the four common mutations taken together [12]. The overall carrier frequency in our cohort of children diagnosed with PFAPA reached 1:3.6 and should be attributed to their Mediterranean extraction rather than related to PFAPA syndrome.
Three children (5.3%) carried a mutation in CARD15/NOD2. A case–control study in Crohn’s disease patients revealed a 10.7 and a 2.4% frequency for CARD15/NOD2 mutations in healthy Jewish and Arab individuals, respectively [3]. Hence, our results ruled out a possible association between CARD15/NOD2 mutations and PFAPA syndrome, in line with the results obtained by Cazeneuve et al. 2003 [9].
One child (1.8%) was heterozygote for the TNFr1A R92Q mutation associated with TRAPS. TRAPS is an auto-inflammatory syndrome caused by dominant mutations in TNFr1A, leading to a decrease in the soluble TNF receptor and increased TNF activity [15]. The clinical symptoms include deep muscle cramping usually associated with fever, severe abdominal and scrotal pain, arthritis and pleuritis [6]. The R92Q mutation reaches a frequency of 1% in the general population and a higher frequency in the TRAPS population and is considered as a variant that is rather asymptomatic and sometimes associated with a mild form of disease [15, 16]. With this in mind the R92Q mutation in the TNF receptor can be excluded as a susceptibility marker contributing to PFAPA.
Taken together, 19 patients were heterozygotes for a mutation in the genes tested, predominantly MEFV with an overall frequency of 28.1%. In spite of their high frequency, we cannot conclude that these variants are legated to PFAPA and whether, when mediated by the presence of additional modifiers, may expose a transient condition, namely PFAPA, limited to patients of young age.
References
Samuels J, Ozen S (2006) Familial Mediterranean fever and the other autoinflammatory syndromes: evaluation of the patient with recurrent fever. Curr Opin Rheumatol 18:108–117. doi:10.1097/01.bor.0000198006.65697.5b
Yao Q, Furst DE (2008) Autoinflammatory diseases: an update of clinical and genetic aspects. Rheumatology 47:946–951. doi:10.1093/rheumatology/ken118
Karban A, Atia O, Leitersdorf E, Shahbari A, Sbeit W, Ackerman Z, Mualem R, Levine A, Nesher S, Safadi R, Eliakim R (2005) The relation between NOD2/CARD15 mutations and the prevalence and phenotypic heterogeneity of Crohn’s disease: lessons from the Israeli Arab Crohn’s disease cohort. Dig Dis Sci 50:1692–1697. doi:10.1007/s10620-005-2917-x
Marshall GS, Edwards KM, Butler J, Lawton AR (1987) Syndrome of periodic fever, pharyngitis, and aphthous stomatitis. J Pediatr 110:43–46. doi:10.1016/S0022-3476(87)80285-8
Feder HM Jr, Bialecki CA (1989) Periodic fever associated with aphthous stomatitis, pharyngitis and cervical adenitis. Pediatr Infect Dis J 8:186–187
Lierl M (2007) Periodic fever syndromes: a diagnostic challenge for the allergist. Allergy 62:1349–1358. doi:10.1111/j.1398-9995.2007.01534.x
Miller LC, Sisson BA, Tucker LB, Schaller JG (1996) Prolonged fevers of unknown origin in children: patterns of presentation and outcome. J Pediatr 129:419–423. doi:10.1016/S0022-3476(96)70075-6
Padeh S, Brezniak N, Zemer D, Pras E, Livneh A, Langevitz P, Migdal A, Pras M, Passwell JH (1999) Periodic fever, aphthous stomatitis, pharyngitis, and adenopathy syndrome: clinical characteristics and outcome. J Pediatr 135:98–101. doi:10.1016/S0022-3476(99)70335-5
Cazeneuve C, Geneviève D, Amselem S, Hentgen V, Hau I, Reinert P (2003) MEFV gene analysis in PFAPA. J Pediatr 143:140–141. doi:10.1016/S0022-3476(03)00259-2
Maschio M, Oretti C, Ventura G, Pontillo A, Tommasini A (2006) CARD15/NOD2 mutations are not related to abdominal PFAPA. J Pediatr 149:427. doi:10.1016/j.jpeds.2006.02.032
Gershoni-Baruch R, Kepten I, Shinawi M, Brik R (1999) Direct detection of common mutations in the familial Mediterranean fever gene (MEFV) using naturally occurring and primer mediated restriction fragment analysis. Mutation in brief no. 257. Online. Hum Mutat 14:91. doi:10.1002/(SICI)1098-1004(1999)14:1<91::AID-HUMU22>3.0.CO;2-8
Gershoni-Baruch R, Shinawi M, Leah K, Badarnah K, Brik R (2001) Familial Mediterranean fever: prevalence, penetrance and genetic drift. Eur J Hum Genet 9:634–637. doi:10.1038/sj.ejhg.5200672
Pras M, Bronshpigel N, Zemer D, Gafni J (1982) Variable incidence of amyloidosis in familial Mediterranean fever among different ethnic groups. Johns Hopkins Med J 150:22–26
Sohar E, Gafni J, Pras M, Heller J (1967) Familial Mediterranean fever: a survey of 470 cases and review of the literature. Am J Med 43:227–253. doi:10.1016/0002-9343(67)90167-2
Hull KM, Drewe E, Aksentijevich I, Singh HK, Wong K, McDermott EM, Dean J, Powell RJ, Kastner DL (2002) The TNF receptor-associated periodic syndrome (TRAPS): emerging concepts of an autoinflammatory disorder. Medicine (Baltimore) 81:349–368. doi:10.1097/00005792-200209000-00002
Ravet N, Rouaghe S, Dodé C, Bienvenu J, Stirnemann J, Lévy P, Delpech M, Grateau G (2006) Clinical significance of P46L and R92Q substitutions in the tumour necrosis factor superfamily 1A gene. Ann Rheum Dis 65:1158–1162. doi:10.1136/ard.2005.048611
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Dagan, E., Gershoni-Baruch, R., Khatib, I. et al. MEFV, TNF1rA, CARD15 and NLRP3 mutation analysis in PFAPA. Rheumatol Int 30, 633–636 (2010). https://doi.org/10.1007/s00296-009-1037-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-009-1037-x