
Abstract
The outcomes of Leishmania infection are determined by host immune and nutrition status, parasite species, and co-infection with other pathogens. While subclinical infection and self-healing cutaneous leishmaniasis (CL) are common, uncontrolled parasite replication can lead to non-healing local lesions or visceral leishmaniasis (VL). It is known that infection control requires Th1-differentiation cytokines (IL-12, IL-18, and IL-27) and Th1 cell and macrophage activation. However, there is no generalized consensus for the mechanisms of host susceptibility. The recent studies on regulatory T cells and IL-17-producing cells help explain the effector T cell responses that occur independently of the known Th1/Th2 cell signaling pathways. This review focuses on the immunopathogenesis of non-healing American CL and progressive VL. We summarize recent evidence from human and animal studies that reveals the mechanisms of dysregulated, hyper-responses to Leishmania braziliensis, as well as the presence of disease-promoting or the absence of protective responses to Leishmania amazonensis and Leishmania donovani. We highlight immune-mediated parasite growth and immunopathogenesis, with an emphasis on the putative roles of IL-17 and its related cytokines as well as arginase. A better understanding of the quality and regulation of innate immunity and T cell responses triggered by Leishmania will aid in the rational control of pathology and the infection.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Leishmaniasis represents a group of neglected tropical diseases caused by infection with protozoan parasites from the genus Leishmania. These parasites are widely distributed in 88 tropical and subtropical countries and pose a major public health problem and a risk for people living in or traveling to the endemic areas. It has an annual estimated worldwide incidence of 600,000 and prevalence of 12 million cases. Leishmaniasis is a vector-transmitted disease, and at least 20 species of Leishmania are known to be pathogenic for humans [1]. These parasites have a di-genetic life cycle, multiplying as flagellated promastigotes in the midgut of sand flies and as non-flagellated amastigotes within mammalian phagocytes. Uncontrolled parasite replication can lead to non-healing cutaneous leishmaniasis (CL), diffuse cutaneous leishmaniasis (DCL), mucosal leishmaniasis (ML), or visceral leishmaniasis (VL). The available anti-Leishmania drugs are far from satisfactory due to high costs, toxicity, or drug resistance. While prophylactic and therapeutic vaccines are in great need, there are currently no effective vaccines for any leishmaniasis forms. This is partially due to an incomplete understanding of correlates of protective immunity and insufficient information on parasite antigens that elicit protective T cell response and appropriate regulation, since both inadequate and excessive immune responses can contribute to pathogenesis, leading to vaccine failure.
The epidemiology of leishmaniasis is extremely diverse. The outcomes of infection are determined by both the host immune status and the parasite species involved. Subclinical infection and self-healing CL are common. Asymptomatic Leishmania infection is detected in endemic areas by a positive, delayed-type hypersensitivity (DTH) skin test (called leishmanin or Montenegro skin test). In some individuals, infections can progress to non-healing skin or mucosal lesions, or other severe forms. Co-infection with other pathogens can also complicate disease severity. Leishmaniasis and human immunodeficiency virus (HIV) are common infectious diseases with overlapping and expanding endemic areas, a situation which has led to an increased occurrence of Leishmania/HIV co-infection [2]. For example, while Southern Europe had the most co-infection cases reported to WHO in 2001, the number of co-infection cases in other endemic areas has markedly increased, as 30 % of all VL patients in Northwest Ethiopia are also infected with HIV [3]. These two pathogens promote each other by enhancing pathogen intake, intracellular survival, and disease progression [4], and such cross-interactions markedly complicate diagnosis, treatment, and patient management [2, 3].
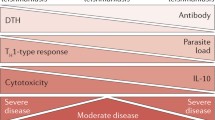
Host immune responses to Leishmania parasites are regulated by highly complex pathways. Animal models of CL and VL have been instrumental for dissecting the mechanisms underlying protective immunity and disease pathogenesis. The current paradigm in murine CL models of Leishmania major infection is that healing requires sequential events, including the activation of dendritic cells (DC), the production of Th1 differentiation cytokines (IL-12, IL-18, and IL-27), the activation of IFN-γ/TNF-α-producing Th1 cells, and the classical activation of macrophages (MΦ; reviewed in [5], as illustrated in red in Fig. 1). The biochemical pathways in classically activated MΦ, as well as roles of reactive oxygen species (ROS) and reactive nitrogen intermediates, such as nitric oxide (NO) in parasite killing are well described [6]. However, there is no generalized consensus for the mechanisms of host susceptibility, as different events are preferentially triggered in a given host (humans versus animal models) following infection with different Leishmania species (as illustrated in blue in Fig. 1). For example, IL-4, IL-10, and IL-13 have differential roles in host susceptibility to distinctive substrains of L. major [5]. Notably, the Th1/Th2 polarization of IFN-γ/IL-4 production observed in murine models of L. major infections is not fully applicable to human diseases and to some other Leishmania infection models (reviewed in [7]). Much less is known regarding the pathogenic mechanisms of non-healing American CL and progressive VL.

The complex factors for the regulation of healing and non-healing leishmaniasis
IL-17-producing CD4+ T cells (Th17) have recently been defined as a separate effector T cell lineage, important in the maintenance of homeostasis through the production of IL-17A, IL-17F, IL-21, and IL-22 [8, 9]. The discovery of this new CD4+ T cell subset explains the effector T cell responses that occur independently of known Th1 and Th2 cell signaling pathways. RORγt and RORα are the two master transcriptional regulators involved in Th17 differentiation, but other transcriptional factors (e.g., STAT3, IRF4, and BATF) also contribute to this process (reviewed in [10]). Ghoreschi et al. [9] have reported two distinct Th17 subsets under in vitro stimulation conditions: the conventional Th17 (or Th17β) cells generated following TGF-β/IL-6 stimulation and inflammatory Th17 cells generated following IL-6/IL-23/IL-17 stimulation. These Th17 subsets play pivotal roles in autoimmunity and chronic inflammatory diseases [11] and participate in defense mechanisms against certain pathogens including Leishmania (see below). These seminal studies open new areas for investigation and validation in humans and experimental animals.
In this review, we focus on the immunopathogenesis of non-healing American CL and progressive VL. The purpose of this review is not to provide a comprehensive summary for the host immune responses against Leishmania parasites or protective/deleterious host immunity against L. major, as there are excellent reviews covering these areas [5, 12]. Instead, we will summarize recent evidence from human patients and animal studies that reveals the mechanisms of dysregulated, hyper-responses to Leishmania braziliensis, as well as the presence of disease-promoting responses to Leishmania amazonensis and Leishmania donovani parasites or the absence of protective responses. We will highlight immune-mediated parasite growth, as well as the immunopathogenesis of non-healing CL and progressive VL, with emphasis on the putative roles of IL-17 and its related cytokines, as well as macrophage-derived arginase and parasite-derived factors. A better understanding of the quality and regulation of innate immunity and T cell responses triggered by Leishmania, especially in the context of HIV co-infection, would aid in the rational control of pathology and the infection.
Non-healing human diseases associated with L. braziliensis infection
Parasites in the Leishmania (Viannia) subgenus (L. braziliensis, Leishmania guyanensis, Leishmania panamensis, and Leishmania peruviana) are the most prevalent etiologic agents of human CL in Central and South America. Among these infections, approximately 2–3 % of patients develop disseminated skin lesions, and 3–5 % of patients progress to ML [13]. The main pathogen of ML in the Amazon region is L. braziliensis, followed by L. guyanensis [14]. ML is a severe and disfiguring form of the disease, usually compromising mucosal regions of the nose, mouth, and pharynx [15, 16]. Pathologically, ML is characterized by excessive T and B cell responses to the parasite. These patients tend to produce elevated levels of anti-Leishmania antibodies and excessive amounts of proinflammatory cytokines (e.g., IFN-γ, TNF-α, and IL-6) [15, 17]. Large-scale, gene polymorphism studies indicated that promoter polymorphisms for high production of IL-10 by monocytes and regulatory T (Treg) cells increase the risk of CL lesions [18], whereas polymorphisms for high production of IL-6 and CCL2 increase the risk of ML, but not of localized CL [19, 20]. These studies may indicate a differential link between the host genetic predisposition for dysregulated inflammatory responses and the risk of severe infections. However, how host-, pathogen-, and microenvironment-associated factors lead into ML progression remain largely uncharacterized. Recent studies discussed below have shed some new light on contributors to the infection outcomes.
Roles of IL-17-producing cells
In response to stress, tissue injury, or invading pathogens, host innate immune cells [21] and newly described T cell subsets can produce IL-17 [8, 9]. IL-17-producing cells play a pivotal role in neutrophil recruitment at early stages of infection, as well as in autoimmunity and chronic inflammatory diseases. In human infection caused by L. donovani, IL-17 and IL-22 are associated with protection against kala azar [22, 23]. With regard to American CL, four studies have investigated the production of and possible roles for IL-17 in L. braziliensis infection. Bacellar et al. [24] first reported in 2009 that lymphocytes obtained from patients with ML and CL produce higher levels of IL-17 than did lymphocytes obtained from uninfected control subjects, implying a role for IL-17 in the pathogenesis of the inflammatory reaction in leishmaniasis. This group also compared cytokine profiles in PBMCs of subclinical infection, patients with CL, and healthy subjects [25]. They found no major roles for regulatory cytokines such as IL-10 and IL-27, but the subclinical group tended to have higher levels of IL-17 than the other two groups. A similar association between IL-17 and protection was found in individuals exposed to L. donovani during an outbreak of VL [23] (see below). A possibility of IL-17 in an innate immune response to L. braziliensis infection is suggested by the authors, but not thoroughly investigated. Boaventura et al. evaluated the involvement of the IL-17-type response in the inflammatory infiltrate of biopsy specimens from ML patients. They found that IL-17+ T cells and neutrophils, as well as IL-17-inducing cytokines (IL-1β, IL-23, IL-6, and TGF-β), were readily detected in the ML biopsies, and that these staining patterns were coincident with those of neutrophil elastase, myeloperoxidase, and MMP-9 [26]. In models of arthritis, Th17 cells have been identified to be osteoclastogenic and mediate bone desorption [27, 28], so these cells may similarly drive the destructive processes in ML. Therefore, IL-17 may contribute to ML pathogenesis through several mechanisms, including neutrophil activation, tissue injury, and osteoclast activation (as illustrated in blue in Fig. 1).
More recently, Castellano et al. [29] found that following stimulation with L. braziliensis antigens, there was a decreased frequency of IL-17+CD3+CD4+ cells in circulating T cells from an HIV-positive ML patient; however, the biological significance of this alteration remained unclear. Collectively, these clinical studies indicated that the regulated production of IL-17 contributes to infection control, while excessive IL-17 can promote neutrophil influx and tissue damage, thereby increasing the risk of ML. Additional studies will verify this hypothesis and reveal the major producers of IL-17 at early versus late stages of infection. Furthermore, in light of the previous finding of reduced IL-10 receptor expression in ML compared to CL lesions [30], the role of IL-10 in regulating the IL-17-driven inflammatory response needs additional investigation. Since human neutrophils and monocytes can express two IL-8 receptors, CXCR1/IL-8RA and CXCR2/IL-8RB [31], it is important to examine whether the differential expression of these receptors has any functional significance in proinflammatory activities of neutrophils during Leishmania infection. Along this line, there is a report of an association of ML with the rare derived G allele at CXCR1 and for a positive role of neutrophils in preventing this form of the disease [32]. Additional immunological studies are warranted to define the regulation of IL-17 and CXCR1 in neutrophil-mediated responses.
Roles of IFN-γ- and TNF-α-related mediators
IFN-γ and TNF-α are key cytokines in the protective responses against intracellular pathogens, and their gene expression levels are regulated by single nucleotide polymorphisms (SNP) [33, 34]. Analysis of TNF polymorphisms in Venezuelan CL patients clearly indicates a positive association with ML [34]. Matos et al. conducted an IFN-γ SNP study with 78 CL and 58 ML cases and 609 healthy controls in Brazil. They found no association between IFN-γ polymorphism and American CL forms, but reported that gene polymorphisms can influence parasite-induced IFN-γ production [35]. Given that excessive production of IFN-γ and TNF-α is a hallmark for ML, it is also possible that L. braziliensis parasites are intrinsically potent in stimulating host responses, favoring cellular recruitment and disease severity. To test this hypothesis, our group examined the response of healthy volunteer PBMCs to L. braziliensis and used L. amazonensis as an infection control [36]. We observed that while L. braziliensis infection induced the production of CXCL10 (also known as IP-10) and IL-10 in human PBMCs and blood monocytes, an enhanced expression of CXCL10 and its receptor CXCR3 was predominantly detected in CD14+ monocytes. The chemoattractant factors secreted by L. braziliensis-infected cells were more efficient in recruiting uninfected PBMCs (predominantly CD14+ cells) than were L. amazonensis-infected cells. Also, we found that sera of L. braziliensis-infected patients (especially the ML cases) had significantly elevated levels of CXCL10, CCL4, and soluble TNF receptor II [36]. Therefore, L. braziliensis parasites are highly competent in stimulating the host to produce multiple inflammatory mediators, and different chemokines may affect the predominance of cell infiltration in distinct clinical manifestations. CXCL10 is secreted mainly by monocytes, fibroblasts, and endothelial cells in response to stimuli (e.g., viral infection, LPS, IL-1β, and IFN-γ) and involves the recruitment of monocytes, MΦs, and T cells to sites of inflammation (see review in [37]). The investigation of CXCR3 ligands (CXCL9, CXCL 10, and CXCL11) and other inflammatory chemokines, in the context of IFN-γ/TNF-α production, in localized versus disseminated lesions has shed new light on the complex regulation of inflammatory responses during L. braziliensis infection [38].
Non-healing human diseases associated with L. amazonensis and Leishmania mexicana infection
Parasites in the L. L. mexicana complex (L. mexicana, L. amazonensis, and Leishmania pifanoi) are the etiological agents for a broad spectrum of leishmaniasis in Central and South American countries, including mild and localized CL, DCL, and rarely fatal VL [39]. DCL is a rare, but severe, form and is not limited to patients in South America. In patients with Leishmania tropica, L. major, or L. donovani infections in India and Africa, DCL or disseminated CL is also considered a clinical indicator of HIV co-infection [40, 41]. There is also a case report of DCL that developed in the context of the immune reconstitution inflammatory syndrome in a man with AIDS following initiation of antiretroviral therapy [18]. Generally speaking, patients with DCL share some clinical characteristics. For example, the lesions have a presentation of numerous non-ulcerating nodules and are histopathologically characterized by heavily parasitized MΦs. These patients often have a negative reaction to the leishmanin skin test and poor antigen-stimulated T cell proliferation in vitro, although some patients remain responsive to other antigens such as tuberculin and lepromin [39]. These profound impairments in cell-mediated immune responses partially explain the relatively poor responses and frequent relapses of DCL patients following anti-Leishmania chemotherapy. This antigen-specific T cell anergy is likely due to alterations in the activation of DC and MΦ following infection with L. amazonensis (see review in [15, 42] and illustration in blue in Fig. 1).
Impaired host innate immunity
Among the Leishmania species that are pathogenic to humans, only the L. mexicana complex parasites are capable of forming huge parasitophorous vacuoles that contain numerous amastigotes. Under cell-free and in vitro conditions, L. amazonensis parasites (especially the amastigote form) are highly resistant to neutrophil- or MΦ-derived leishmaniacidal molecules, or anti-Leishmania drugs, compared to other Leishmania species [43, 44]. These are indicative of biological features that are unique and intrinsic to these parasites. L. amazonensis amastigotes are superior in silent invasion, preventing the activation of NK, DC, and MΦ triggered by exogenous stimuli such as LPS [42, 45]. The intracellular events triggered by L. amazonensis infection in MΦs have been described in detail [45, 46]. The suppression of host cell activation can be initiated at early stages of amastigote–host contact. On one hand, L. amazonensis amastigotes can infect human DCs through multiple receptors such as Fc receptors, complement receptors, heparin-binding proteins, and DC-SIGN [47]. Signaling through these receptors can lead to altered DC activation and impaired responsiveness to exogenous stimuli through MAP kinase-mediated mechanisms [48]. On the other hand, L. amazonensis amastigotes can expose phosphatidylserine (PS) on their surface, leading to enhanced parasite growth and host suppression through IL-10 and TGF-β production by host cells [49]. Although the origin and biochemical nature of PS detected on amastigote surface remains undefined, PS exposure may contribute to the suppression of anti-Leishmania immunity [50], as reported for other pathogens such as Toxoplasma gondii and Vibrio cholerae [51, 52]. No doubt, L. amazonensis and its related parasites have evolved complex strategies to down-modulate host innate immune responses, leading to T cell malfunction (as illustrated in black in Fig. 1).
The quality of T cell responses to L. amazonensis and L. mexicana
In a recent report, Campanelli et al. [53] analyzed leukocytes isolated from early skin lesions (<30 days of infection), late lesions (>60 days of infection), and DCL lesions (>10 years). Compared with the early-infection lesions, the late-infection lesions showed a reduced frequency of CXCR3+ cells, but an increased frequency of CCR4+ and IL-10+ T cells. Compared with the CL lesions, the DCL lesions exhibited a reduced frequency of CCR3-, CCR4-, CCR5-, and CCL17-positive cells, but an increased frequency of CCL7-positive cells. These changes correlate with the impaired T cells responses observed by other groups [17, 54], implying a poor quality of T cell responses to L. amazonensis antigens. This notion is further supported by a recent study of Macedo et al. [55], which compared the quality of T cell responses induced by promastigote crude antigens of L. braziliensis and L. amazonensis in PBMCs from healed CL patients. Their multi-parametric flow cytometric studies indicated that L. braziliensis antigens induced an important proportion of multi-cytokine-producing CD4+ T cells (28 % of the total Th1 response evaluated), whereas L. amazonensis antigens mostly (68 %) induced single-positive cells, 57 % of which were IFN-γ single positives. Since the percentages of total IFN-γ-producing CD4+ T cells induced by both antigens were comparable, this study emphasizes the importance of Th1 response quality, not just its magnitude, in the study of diverse immunopathogenesis of leishmaniasis.
The role of CD8 cytotoxicity in DCL versus CL patients is less clear. Hernandez-Ruiz et al. [56] compared the overall immune effector functions of CD8+ T cells for ten CL and four DCL Mexican patients diagnosed with L. mexicana infection. They found that in comparison to the CL group, peripheral CD8+ T cells from DCL patients displayed impaired effector functions, as judged by their levels of IFN-γ production in vitro and cytotoxicity against L. mexicana-infected autologous MΦs. This impaired CD8 function correlated with the reduced numbers of CD8+ T cells and TUNEL+ apoptotic cells in lesions of DCL patients. These authors have suggested a functional exhaustion of CD8+ T cells in DCL patients and provided some evidence for restoring their effector functions, following the stimulation of these CD8+ T cells with TLR2-specific agonists such as Pam3Cys and L. mexicana LPG [56]. This is the first in vitro study for TLR2-mediated restoration of effector functions for CD8+ T cells derived from DCL patients. Given that DCL patients lack effective innate and adaptive immune responses for controlling parasite infection and anti-Leishmania drugs only achieve transitory remission in DCL patients, this report, together with related studies in patients and mice, highlights the need for comprehensive treatment schemes for patients infected with L. amazonensis and L. mexicana. Since the number of CD8+ T cells tends to increase during the healing process of the skin lesions of DCL patients [57], it is important to further define the overall effector mechanisms of CD8+ T cells in human leishmaniasis.
Animal models of L. braziliensis and L. amazonensis infection
While genetically resistant and susceptible strains of mice are valuable for defining polarized Th1 and Th2 immune responses, as well as the contribution of Th17 and Treg, during L. major infection [5], the susceptibility of mice to the New World Leishmania species is diverse and complex, depending on the parasite species under investigation. In general, all commonly used inbred strains of mice (including BALB/c mice) are genetically resistant to L. braziliensis infection. The gene-targeted deletion of key molecules involved in NO production can increase mouse susceptibility to L. braziliensis. Although mice are also generally resistant to L. guyanensis, L. panamensis, and L. peruviana, chronic skin lesions can be successfully induced following infection of BALB/c mice with percoll-purified promastigotes of L. panamensis [58]. For parasites in the L. Viannia subgenus, hamsters are a more suitable model than mice for the pathological study of localized and metastatic lesions [59]. In contrast, commonly used inbred strains of mice are genetically susceptible to L. amazonensis infection (see review by [60]). The deletion of either the IL-4 or IL-10 gene has no major effect on mouse susceptibility to L. amazonensis; however, deleting functional CD4+ T cells or B cells markedly reduces lesion pathology [61, 62], implying a complex, Th2-independent regulation of host susceptibility to L. amazonensis infection (see review by [63]).
Self-healing infection caused by L. braziliensis
L. braziliensis infection is self-healing in all inbred strains of mice, and small lesions reach their peaks at about 4–6 weeks post-infection. Parasite clearance is primarily due to the efficient activation of DC, MΦ, and T cells at the site of infection and in the draining lymph nodes, and to the intrinsic susceptibility of this parasite to microbicidal activities of the host cell. The interaction of neutrophils with L. braziliensis-infected MΦ also promotes parasite killing via TNF-α- and superoxide-associated mechanisms [64]. To further test the notion that L. braziliensis infection efficiently triggers innate and adaptive responses, we generated axenic amastigotes of L. braziliensis and examined DC and MΦ responses to L. braziliensis and L. amazonensis. By using fluorescence-labeled promastigotes and amastigotes, we found that L. braziliensis (but not L. amazonensis) infection-induced DC activation/maturation and IL-12p40 production in both infected and bystander cells, and that DC activation was accompanied by upregulation of the JAK/STAT signaling pathway, especially in regard to the expression of phosphorylated-STAT1 and -STAT3, IFN regulatory factor 1 (IRF-1), and ISG15. Moreover, L. braziliensis-infected DCs were highly efficient in priming naïve CD4+ T cells to proliferate and produce IFN-γ and IL-17 [42, 65]. These new findings from mouse models aid in our understanding as to how the host mounts immune responses against L. braziliensis. However, L. braziliensis-infected mice are not good models for studying ML, partially due to the relatively high sensitivity of their promastigotes and axenic amastigotes to NO-mediated killing (Fig. 2a) and to the relative ease of the mouse MΦs to produce NO (in comparison to human or hamster MΦs [66]).

Differential responses of Leishmania amazonensis (La) and Leishmania braziliensis (Lb). a Kinetics of NO-mediated killing of La and Lb parasites. CFSE-labeled promastigotes (Pm) and axenic amastigotes (Am, 1 × 107/ml) were exposed to 10 mM NaNO2 in PBS pH 4.5 at 23 °C. The intensity of CFSE was determined by flow cytometry. For untreated parasites, only the 90-min data are shown. b Bone marrow-derived DCs were generated from C57BL/6 mice and infected with promastigotes and axenic amastigotes of La and Lb at the indicated ratios. At 24 h post-infection, the levels of IL-12p40 in culture supernatants were assayed by ELISA. c DC (infected for 24 h) were co-cultured with naïve CD4+ T cells (2 × 106/ml) at an 1:10 DC-to-T ratio for 4 days. The levels of cytokines in culture supernatants were assayed by ELISA. *p < 0.05; **p < 0.01; ***p < 0.001. b and c were adapted from Vargas-Inchaustegui et al. [65]
Non-healing CL caused by L. amazonensis
In sharp contrast, L. amazonensis infection is non-healing in all inbred strains of mice (see review by [60]). Skin lesions become evident after 2–4 weeks and progress continuously for a few months, and some of these lesions can be ulcerated at late stages. The dermal lesions of L. amazonensis-infected mice have a dense cellular infiltrate, composed mainly of parasitized, vacuolated MΦs, and scattered T and B lymphocytes [61, 62]; these histopathological features closely resemble those of non-healing lesions observed in DCL patients [39, 67]. Although promastigotes of L. amazonensis can transiently trigger a low level of DC and MΦ activation, amastigote-carrying cells show little signs of activation (Fig. 2b). In general, L. amazonensis-infected DCs are poor antigen-presenting cells, and their co-cultured T cells are poorly activated (Fig. 2c) [42, 65, 68]. Therefore, repression of host cell activation by Leishmania parasites appears to be species-specific, and L. amazonensis amastigote infection may represent an anergic pathogenicity extremity [17]. Yet, lesion pathology in mice relies on activation of pathogenic CD4+ T cells that produce low levels of IFN-γ, IL-10, IL-17, and other cytokines/chemokines [68, 69]. On one hand, these low-quality T cell responses are ample for recruiting monocytes/MΦs, but are insufficient for activating them fully. Of note, L. amazonensis amastigotes are relatively resistant to NO-mediated parasite killing (Fig. 2a), as well as to neutrophil-mediated parasite killing [44]. L. amazonensis may also be unique in sensing both the external and internal arginine pool by regulating two transporter-coding genes, or in utilizing host innate machineries (e.g., the autophagic and lipid metabolic pathways) for their favored intracellular growth [63, 70]. Therefore, L. amazonensis parasites are extraordinary in their ability to repress host cell activation, resist host anti-microbial machinery, and utilize host resources for their own growth (as illustrated in blue in Fig. 1).
The implication of the new and interesting findings is that a multi-pronged treatment regimen may be desirable for L. amazonensis infection. Thus, for example, an anti-Leishmania therapy in conjunction with immune stimulation may be optimal. We therefore tested whether pre-exposure to L. braziliensis can stimulate anti-L. amazonensis responses. We found that pre-exposure to L. braziliensis can partially protect mice against L. amazonensis infection by increasing the magnitude of T cell responses [69]. It will be interesting to identify the T cell-stimulating antigens of L. braziliensis unique to this species or common to other species. Such antigens would be of value for monitoring human and mouse T cell responses at different stages of infection with L. braziliensis and for potential development of prophylactic or therapeutic vaccines against leishmaniasis.
Spectrum and immunopathogenesis of progressive VL in humans
Infection with L. donovani and Leishmania infantum/Leishmania chagasi can be asymptomatic or subclinical (oligosymptomatic) in a majority of individuals. Less than 10 % of infected people develop active VL or kala azar, which is characterized by fever, fatigue, anorexia, weight loss and cachexia, hepatosplenomegaly, and pancytopenia. The course of disease typically runs over several months and is usually fatal unless the patient receives specific treatment. Asymptomatic Leishmania infection is detected by a positive DTH response, whereas subclinical or non-progressing oligosymptomatic infection is usually evident due to a positive serological test with a few mild and non-specific symptoms [71, 72]. Both retrospective and prospective studies have demonstrated that asymptomatic or subclinical infections are six- to tenfold more common than active VL [73]. Individuals who have had an asymptomatic infection have been shown in limited epidemiological and human challenge studies to be protected from the development of active disease. The immunopathogenic mechanisms of VL in humans are not fully understood. Most information has been gained by comparing parasite antigen-induced immune responses between asymptomatically infected (putatively resistant) individuals and those with active disease (putatively susceptible). This approach makes the tenuous assumption that susceptibility is driven solely by the host immune response and not modified by parasite or environmental factors.
Cytokines, T cell responses, and Treg cells
PBMCs from asymptomatic skin test-positive subjects in VL endemic areas demonstrate strong antigen-induced IFN-γ responses and induction of intracellular parasite killing, whereas PBMCs from active VL patients produce low levels of IFN-γ. Furthermore, low IFN-γ production is characteristic of individuals with subclinical infection that subsequently progressed to VL. While these descriptive studies identify immunological features of active disease, they do not differentiate a permissive host response that led to active disease from a host response that is modulated by the infection. Several pieces of evidence indicate that the production of IFN-γ is insufficient to confer a protective immune response to the visceralizing Leishmania. First, there is elevated expression of IFN-γ (and IL-12) in the plasma of patients with active VL [74, 75]. Second, there is a high level of IFN-γ mRNAs in the lymph node [76], spleen [77], and bone marrow [78] of patients with active VL. Third, whole blood stimulation assays indicate IFN-γ production by blood cells during active VL [79]. Lastly, not all Leishmania-reactive, IFN-γ-producing T cell clones derived from a subclinically infected individual were able to activate infected MΦ to kill intracellular parasites [80]. Th17 cells and IL-17 have been shown to play a protective role against some, but not all, intracellular pathogens [81], but also may be responsible for the excessive inflammation seen in some pathological states, including ML [26]. Recently, individuals exposed to L. donovani during an outbreak of VL in eastern Sudan were found to be most protected against the development of VL when their PBMCs produced IL-17 and IL-22 in response to stimulation with heat-killed parasites [23].
The finding that a robust proinflammatory and type 1 cytokine response does not mitigate progressive VL in humans prompted the consideration that other cytokines known to impair MΦ-mediated killing of Leishmania could have a pathological role [82, 83]. IL-4 and IL-13, which play a prominent disease-promoting role in L. major infection [84], were found to be increased in the serum of some, but not all, patients with active VL [74, 85–87]. The importance of IL-10 in the pathogenesis of human VL is more strongly supported [82]. Patients with VL have elevated levels of IL-10 in serum or plasma [74, 86–88] and increased IL-10 mRNA expression in the spleen and bone marrow [85]. Circulating levels of IL-10 correlated strongly with parasite loads in the blood of patients with VL [89]. In vitro neutralization of IL-10 in PBMC cultures from patients with VL resulted in enhancement of Th1 cell responses to Leishmania antigens, but more notably, neutralization of IL-10 in ex vivo cultured cells from splenic aspirates promoted parasite clearance [90]. T cell IL-10 production in VL may be driven by the proinflammatory cytokine IL-27, as the expression of IL-27's subunits (IL-27-28 and EBI-3) was upregulated in a CD14+ MΦ-enriched fraction of splenocytes isolated from patients with active VL [91]. In this same study, increased T cell expression of IL-21, which can amplify IL-27 production, was identified in the spleens of patients with VL, and treatment of cells with IL-27 and IL-21 significantly enhanced the antigen-induced production of IL-10. Recently, a disease-promoting proinflammatory cytokine response was attributed to increased bacterial translocation from the gastrointestinal tract and endotoxin-mediated immune modulation in patients with VL [92].
Treg (CD4+ CD25+ Foxp3+) cells are a source of IL-10 and contribute to chronic infection in murine L. major infection [93]; however, their possible role in VL has been somewhat controversial. CD4+CD25+ cells that also expressed Foxp3 mRNA and produced IL-10 were also found at increased levels in the spleens and lymph nodes of mice infected with L. infantum [94]. Before treatment, CD4+CD25+ cells were also elevated in the peripheral blood of patients with VL compared to findings post-treatment and when compared to those in endemic controls [95]. However, the CD4+CD25+ population may also include activated, conventional T cells and will not allow the discrimination of Treg without including the Foxp3+ marker. Elegant work by Nylen et al. and Maurya et al. showed that CD25+Foxp3+ Treg do not accumulate in the spleen [85, 96] and are not a major source of IL-10 in patients with active VL [85]. They proposed that IL-10-producing CD4+CD25−Foxp3− T cells are likely a major contributor to the pathogenesis of VL [85]. However, recent work by Rai et al. identified an increased accumulation of CD4+CD25+Foxp3+ cells (but not conventional activated CD4+CD25+Foxp3− T cells) in the bone marrow of patients with VL compared to the patient's peripheral blood or to bone marrow from healthy controls [97]. This finding of increased Treg in the bone marrow [97] but not in the spleen [85, 96] is puzzling and deserves further investigation. In patients with post-kala azar dermal leishmaniasis (PKDL), the expression of mRNAs for Foxp3, CD25, and IL-10 correlated with tissue parasite loads, implying the accumulation of natural Treg cells [98].
Impact of malnutrition
Epidemiologic studies have documented a greatly increased risk for VL in the malnourished host (reviewed in [99]). In fact, one could argue that since VL is a disease of the severely impoverished, rarely does it occur in the well-nourished host. Malnutrition was identified as a risk factor for severe disease and death from VL in both children (OR 5.0) and adults (OR 11.0) [100]. Malnutrition-related VL is particularly evident in displaced and impoverished populations [101, 102], and the recently described movement of transmission into peri-urban slums is likely to lead to an increase in the malnutrition-infection synergism [103]. Although the immunopathogenic basis for the malnutrition-related risk of VL has not been investigated, investigations in a murine model of polynutrient deficiency (deficient protein, energy, zinc, and iron) [104–106], which closely mimicked moderate acute malnutrition, revealed an increased rate of early dissemination following cutaneous infection with L. donovani [105]. Notably, this dissemination was related to the loss of lymph node barrier function and early parasite escape from the draining lymph nodes in the polynutrient-deficient mice. Other investigations in this murine model revealed alteration of the innate MΦ response [104, 106] and impaired adaptive immunity (reduced IFN-γ production) in mice vaccinated against L. chagasi [107].
Impact of HIV co-infection
The cruel synergism between L. donovani and HIV is increasingly evident, as there is an expansion of regions in the world where co-infections occur. It is estimated that HIV increases the risk of VL development in L. donovani-exposed populations by several hundred-fold [3], through either decreased resistance to a new primary infection or reactivation of a previous subclinical infection [108]. Co-infection studies in primary human monocyte-derived MΦs, DCs, and tonsillar tissue demonstrated that each pathogen has a detrimental effect on containment of the other—Leishmania infection enhances HIV replication via chronic immune activation, and that HIV promotes Leishmania infection by suppressing a protective host defense [109–112]. The latter is corroborated by higher levels of L. donovani parasitemia in HIV co-infected individuals [113] and low CD4+ T cell counts despite suppression of viral load by antiretroviral therapy [114].
Mouse and hamster models of VL
The immunopathogenesis of visceralizing Leishmania infection has been most commonly studied in murine models of systemic infection. Mice infected by the intravenous route develop an acutely increasing visceral parasitization, followed by control of parasite replication and reduction in parasite load in the liver over 4–6 weeks and a more chronic infection in the spleen. Although the chronic parasitism does not lead to significant overt morbidity or mortality, the model has been instructive in elucidating immunoprotective and immunopathogenic mechanisms in both the liver and spleen.
Control of hepatic infection in mice
Resolution of hepatic infection is mediated by several critical immunological processes: (1) generation of a type 1 T cell response, (2) effective granuloma formation, and (3) induction of classical macrophage activation (reviewed in [115, 116]). Polarization of T cells to a Th1 phenotype is evident early in the course of infection and maintained by the balance of ongoing stimulation/expansion and increased apoptosis. The critical requirement for IFN-γ-producing Th1 cells is established by demonstration of impaired control of infection in IFN-γ-, STAT1-, and T-bet-deficient mice [117]. IRF-7 and IRF-5, both of which are activated by MyD88-dependent TLR7 signaling, are critical to the generation of effector Th1 responses [118, 119]. Effector T cell migration into the hepatic granuloma is dependent on the expression of CCL19 and CCL21 [120]. Kupffer cells, which make up the primary parasitized phagocyte in the granuloma, present antigens to T cells to initiate the effector response. Neutrophil responses to L. donovani contribute to host defense directly through anti-parasitic effector activity and indirectly by modulating the adaptive immune response toward a protective type 1 phenotype [121]. Classical MΦ activation by IFN-γ/TNF-α or other proinflammatory microbial products leads to the generation of ROS and NO. Both ROS and NO contribute to the control of parasite replication in vivo because mice deficient in gp91phox (a component of NADPH oxidase) have impaired early control of infection (even though these mice ultimately resolve hepatic infection), and NOS2-deficient mice have impaired early and late control of infection [122]. Other, yet-to-be-identified MΦ effector mechanisms also are likely to have a role [123].
The generation of an anti-leishmanial hepatic granulomatous response requires the coordinated interaction of multiple cell types, cytokines, and effector molecules [124]. The production of chemokines (CCL2, CCL3, and CXCL10) by Kupffer cells leads to an influx of inflammatory monocytes and neutrophils within the first few days of infection. CD4+ and CD8+ T cells subsequently accumulate through recruitment and local expansion, leading to the formation of an inflammatory granuloma that generates IFN-γ and TNF-α (reviewed in [115, 116]). A number of other proinflammatory cytokines [IL-2, IL-12, lymphotoxin, and granulocyte macrophage-colony stimulating factor (GM-CSF)] also contribute to granuloma formation and function. Although Th2 cytokines are generally considered to have an immunopathogenic role in some CL models, they play an important role in granuloma formation and protection against L. donovani. In mice deficient in IL-4, IL-13, or IL-4Rα, there was impaired granuloma maturation and control of hepatic replication of L. donovani [125, 126].
Non-resolving splenic infection in mice
L. donovani infection is not as readily controlled in the murine spleen. Following systemic infection, L. donovani parasitizes the marginal zone MΦs (MZM) and marginal metallophilic MΦs in the splenic marginal zone (MZ). The early production of IL-12 by DCs that have migrated from the MZ into the periarteriolar lymphocyte sheath (PALS) in response to CCL19 and CLL21 was found to be critical for the generation of effector T cells and control of parasite replication early in the course of infection [120]. However, these early responses are inadequate to clear parasites from the spleen (in contrast to the resolution of infection in the liver) because there is a slow increase in parasite burden after several weeks, accompanied by splenomegaly and extensive remodeling of the splenic micro-architecture (reviewed in [115, 116]). Splenic expression of IL-10, but not IL-4, contributes to the maintenance of parasite replication (reviewed in [83]). Moreover, IL-10-deficient mice have shown an increased resistance to experimental L. donovani infection [127, 128].
Central to the splenic remodeling is the widely distributed and excessive production of TNF-α (as noted above, moderate levels of TNF-α are required for the protective immune response in the liver), which mediates the loss of MZMs [129] and the depletion of stromal fibroblastic reticular cells (FRC) in the PALS [130]. The FRC make up the splenic conduits that are a critical source of the cytokines CCL19 and CCL21, which mediate CCR7-dependent migration of DCs from the MZ to the PALS [131]. However, the infection-induced depletion of splenic FRC over time has been reported to lead to reduced chemokine expression and less recruitment of CCR7-bearing DCs and naïve T cells into the T cell zone of the PALS [130]. However, DCs isolated from naïve mice were able to migrate into the PALS of L. donovani-infected spleens, mediating a reduction in splenic parasite loads, but DCs isolated from infected mice had impaired migration related to reduced CCR7 expression [130]. Thus, the reduced migration of DCs into the PALS is probably a consequence of the suboptimal expression of both the receptor and its ligands. As splenic infection progresses, the white pulp becomes shrunken and disorganized, and there is destruction of follicular DCs and loss of germinal centers. This destruction is associated with neovascularization and infiltration of the white pulp with heavily parasitized MΦs [132]. The neovascularization process was reversed to some degree by administration of the broadly acting receptor tyrosine kinase inhibitor, sunitinib, which also enhanced the generation of IFN-γ-producing Th1 cells [132]. In parallel with the remodeling of the white pulp, there was also expansion of the red pulp vasculature, which was dependent on the influx of Ly6C+ inflammatory monocytes [133]. The remodeled red pulp in the L. donovani-infected spleen also showed enhanced myelopoiesis, evident by a 20- to 30-fold increase in the numbers of colony-forming units-granulocyte, monocyte (CFU-GM) [134]. This increase was in part due to the active proliferation of progenitor cells and was dependent on increased GM-CSF and TNF-α [134, 135]. This profound expansion of splenic myeloid progenitor cells was accompanied by an increase in parasite loads [134], implying that the accumulation of myeloid cells supported parasite replication.
Progressive disease in hamsters
The Syrian hamster model of VL provides an opportunity to investigate immunopathogenic mechanisms in a model of disease that mimics the progressive, fatal disease of humans. Hamsters infected with L. donovani were found to develop a remarkably higher visceral parasite burden than mice and suffer cachexia, massive splenomegaly, pancytopenia, and ultimately death [136]. Following a period of relatively silent infection, the splenic parasite burden was reported to increase dramatically, and there was an accompanying increase in splenic cellularity, primarily the result of an expansion of the myeloid population [137]. During the course of infection, hamsters showed disrupted splenic architecture accompanied with lymphoid depletion [138] and the loss of antigen-reactive T cell responses [137, 139, 140]; however, the adherent cell-free T cells isolated from hamsters were able to respond to leishmanial antigens and to transfer parasite-specific DTH reactivity to naïve hamsters [139]. Lymphocytes from the lymph nodes of L. donovani-infected hamsters were found to show both cell-cycle arrest and TGF-β-triggered apoptotic death mediated through upregulation of tyrosine phosphatase activity [140]. In the liver, there was heavy parasitization of the Kupffer cells, which are surrounded by an inflammatory infiltrate, but fully organized granulomas did not develop [138]. The uncontained infection was found to occur despite a vigorous type 1 immune response with increased hepatic and splenic expression of IFN-γ, IL-2, IL-12, and TNF-α [141, 142], a response that is associated with control of L. donovani infection in mice. The paradoxical expression of IFN-γ in the face of progressive infection is similar to the findings in human VL. However, concomitant with the type 1 response, there was also increased splenic expression of IL-4, IL-13, IL-10, IL-21, and TGF-β [136, 141]. The roles of these cytokines in the pathogenesis of progressive VL have not been defined.
In striking contrast to mouse MΦs, IFN-γ-activated hamster MΦs expressed minimal NOS2 and did not generate detectable NO; they were unable to restrict the replication of intracellular L. donovani [136, 142]. The reduced transcription of NOS2 mRNA in response to Leishmania infection was related to a IFN-γ-hyporesponsive promoter (similar to what was described for the human NOS2 promoter) and was in part due to the absence of a cis-element for NF-IL6 (C/EBPβ), which is a member of a CCAAT-enhancer binding protein family of transcription factors, in the hamster NOS2 promoter [143]. The inability to control parasite replication in VL was not only related to ineffective classical MΦ activation (low NOS2) but also parasite-induced, STAT6-dependent alternative MΦ activation with dominant arginase 1 expression and polyamine production [136]. Selective knockdown of either arginase 1 or STAT6 led to a reduced parasite burden in this model. Interestingly, the expression of arg1 and activation of STAT6 required the de novo synthesis of protein, implying that additional co-activators and/or pathways contribute to STAT6-dependent, L. donovani-induced arg1 expression. Recently, it was found that IL-10 expressed in the spleens of mice infected with L. donovani induced the upregulation of IL-4Rα, which was required for arg1 expression [144]. Thus, synergy between the IL-4/STAT6 and IL-10/STAT3 pathways may play a central role in the pathogenesis of VL.
Subversion of macrophage function as a contributor to non-resolving and progressive L. donovani infection
It is well described that Leishmania parasites can alter the signaling pathways in mouse and human DC and MΦs (reviewed in [145, 146], as marked in black in Fig. 1). These alterations may play a role in human VL, by subverting the innate immune response and rendering the infected cells less responsive to activating stimuli. For the most part, however, corroborative studies of MΦs from the site of infection, especially in human VL, are lacking. There are a number of mechanisms by which L. donovani escapes MΦ effector activity (see Table 1). Most notably, L. donovani inhibits protein kinase C (PKC) and members of the MAP kinase families, and impairs IFN-γ-mediated MΦ activation, largely, but not exclusively, due to broad activation of cellular protein tyrosine phosphatases (PTPs). Several recent findings deserve to be highlighted. Efforts to illuminate the mechanisms of Leishmania-mediated activation of cellular PTPs revealed that several Leishmania proteins, including EF-1α [147, 148], fructose-1,6-bisphosphate aldolase [149], and GP63 [150] are exported from the phagolysosome into the cytosol and activate PTPs (reviewed in [146]). Impairment of PKC signaling is known to be critical for L. donovani survival in MΦs (reviewed in [151]). Recently, the role of PKC isoforms in the regulation of cytosolic phosphatases and downstream MAP kinase signaling and cytokine production was defined [152]. Infection of mouse MΦs with L. donovani led to upregulation of uncoupling protein 2 (UCP2), a mitochondrial membrane protein that is a negative regulator of ROS generation [153]. Functional knockdown of UCP2 led to enhanced ROS generation and ROS-mediated inhibition of protein tyrosine phosphatases [153], which are known to subvert MΦ activation pathways that lead to generation of NO and parasite killing [154]. L. donovani infection of human MΦs led to phosphorylation of CREB and inactivation of glycogen synthase kinase-3beta (GSK-3β), which resulted in IL-10 production [155] and parasite replication. Since IFN-γ expression in infected tissues is characteristic of VL, it is of considerable interest to understand why this response is ineffective in curbing parasite replication. In L. donovani-infected murine MΦs, IFN-γ receptor expression and receptor–ligand interaction were unaltered; however, co-localization of the two IFN-γ receptor subunits was impaired due to infection-mediated increase in membrane fluidity and cholesterol quenching [156]. IFN-γ signaling and parasite killing could be recovered by delivery of cholesterol to the MΦ membrane [156].
Concluding remarks
The emerging evidence from recent studies has uncovered the complex host–Leishmania interactions that contribute to delay in healing or non-healing lesions (summarized in Fig. 1). At the early stages of the infection, host, parasite, or vector factors that promote sustained neutrophil influx and altered neutrophil functions can facilitate promastigote infection in the host and parasite spread to other target cells [157, 158]. At the subsequent stages, multiple and complex mechanisms of immune dysregulation act alone or in combination, resulting in persistent infection and/or tissue damage, depending on the involving parasite species.
Firstly, IL-17-producing T cells, as well as IL-17-inducing cytokines (IL-1β, IL-6, IL-23, and TGF-β), seem to have complex and dual roles, depending on the infection stages and involving parasite species. Their protective roles are likely to be in conjunction with Th1 cell activation. Their detrimental roles are mediated via the regulation of additional waves of neutrophil recruitment, promoting lesion progression and tissue damage, as elegantly illustrated in L. major-susceptible mice [159, 160] and suggested in the above-mentioned human infections with L. braziliensis. Secondly, host factors that trigger MΦ alternative activation (IL-4, IL-10, IL-13, and TGF-β insulin-like growth factor) or MΦ suboptimal activation (low levels of IFN-γ and TNF-α) can create a microenvironment in favor of amastigote replication [46, 63]. Parasite growth within these MΦs can be mediated via host arginase-dependent and -independent mechanisms, as illustrated by mouse models of L. amazonensis and L. mexicana infection and hamster models of L. donovani infection [136]. Similarly, parasite-encoded arginase and arginine transporters can serve as virulence factors, subverting MΦ microbicidal activity [70, 161]. Thirdly, host or parasite factors that repress NO or ROS production by infected neutrophils or MΦs, or repress the activation of DC and T cells, will delay parasite clearance and lesion control [46]. In this regard, recent studies of NO-resistant L. amazonensis and L. braziliensis isolated from patient lesions have offered new insights into non-healing CL and non-responsiveness of patients to antimony therapy [162–164].
It is clear that hyper- and hypo-immune responses both contribute to non-healing American CL and severe VL, and that the magnitude of these responses are regulated by DC and Treg cells. The major challenge is to define the host and parasite factors that lead to immune dysregulation at early versus late stages of infection. It is particularly important that the function of leukocyte populations be defined within the tissue environment of the infection site to avoid the limitations of in vitro models of infection/response. A better understanding of how different species and stages of Leishmania parasites can selectively utilize host innate defense machinery and adoptive immunity for immune evasion, intracellular growth, and immunopathogenesis will lead to the rational design of control strategies for this and other related infections.
References
Banuls AL, Hide M, Prugnolle F (2007) Leishmania and the leishmaniases: a parasite genetic update and advances in taxonomy, epidemiology and pathogenicity in humans. Adv Parasitol 64:1–109
Guerra JA, Coelho LI, Pereira FR, Siqueira AM, Ribeiro RL et al (2011) American tegumentary leishmaniasis and HIV-AIDS association in a tertiary care center in the Brazilian Amazon. AmJTrop Med Hyg 85:524–527
Alvar J, Aparicio P, Aseffa A, Den Boer M, Canavate C et al (2008) The relationship between leishmaniasis and AIDS: the second 10 years. Clin Microbiol Rev 21:334–359, table of contents
Lodge R, Ouellet M, Barat C, Andreani G, Kumar P et al (2012) HIV-1 promotes intake of Leishmania parasites by enhancing phosphatidylserine-mediated, CD91/LRP-1-dependent phagocytosis in human macrophages. PLoS One 7:e32761
Tacchini-Cottier F, Weinkopff T, Launois P (2012) Does T helper differentation correlate with resistance or susceptibility to infection with L. major? Some insights form the murine model. Frontiers Immunol 3:1–9
Van Assche T, Deschacht M, da Luz RA, Maes L, Cos P (2011) Leishmania-macrophage interactions: insights into the redox biology. Free Radic Biol Med 51:337–351
McMahon-Pratt D, Alexander J (2004) Does the Leishmania major paradigm of pathogenesis and protection hold for New World cutaneous leishmaniases or the visceral disease? Immunol Rev 201:206–224
Cua DJ, Tato CM (2010) Innate IL-17-producing cells: the sentinels of the immune system. Nat Rev Immunol 10:479–489
Ghoreschi K, Laurence A, Yang XP, Tato CM, McGeachy MJ et al (2010) Generation of pathogenic TH17 cells in the absence of TGF-beta signalling. Nature 467:967–971
Hirota K, Ahlfors H, Duarte JH, Stockinger B (2012) Regulation and function of innate and adaptive interleukin-17-producing cells. EMBO Rep 13:113–120
Hirota K, Duarte JH, Veldhoen M, Hornsby E, Li Y et al (2011) Fate mapping of IL-17-producing T cells in inflammatory responses. Nat Immunol 12:255–263
Kaye P, Scott P (2011) Leishmaniasis: complexity at the host-pathogen interface. Nat Rev Microbiol 9:604–615
Jirmanus L, Glesby MJ, Guimaraes LH, Lago E, Rosa ME et al (2012) Epidemiological and clinical changes in American tegumentary leishmaniasis in an area of Leishmania (Viannia) braziliensis transmission over a 20-year period. AmJTrop Med Hyg 86:426–433
Guerra JA, Prestes SR, Silveira H, Coelho LI, Gama P et al (2011) Mucosal leishmaniasis caused by Leishmania (Viannia) braziliensis and Leishmania (Viannia) guyanensis in the Brazilian Amazon. PLoS Negl Trop Dis 5:e980
Reithinger R, Dujardin JC, Louzir H, Pirmez C, Alexander B et al (2007) Cutaneous leishmaniasis. Lancet Infect Dis 7:581–596
Miranda A, Carrasco R, Paz H, Pascale JM, Samudio F et al (2009) Molecular epidemiology of American tegumentary leishmaniasis in Panama. AmJTrop Med Hyg 81:565–571
Silveira FT, Lainson R, De Castro Gomes CM, Laurenti MD, Corbett CE (2009) Immunopathogenic competences of Leishmania (V.) braziliensis and L. (L.) amazonensis in American cutaneous leishmaniasis. Parasite Immunol 31:423–431
Sinha S, Fernandez G, Kapila R, Lambert WC, Schwartz RA (2008) Diffuse cutaneous leishmaniasis associated with the immune reconstitution inflammatory syndrome. Int J Dermatol 47:1263–1270
Castellucci L, Menezes E, Oliveira J, Magalhaes A, Guimaraes LH et al (2006) IL6–174 G/C promoter polymorphism influences susceptibility to mucosal but not localized cutaneous leishmaniasis in Brazil. J Infect Dis 194:519–527
Ramasawmy R, Menezes E, Magalhaes A, Oliveira J, Castellucci L et al (2010) The −2518 bp promoter polymorphism at CCL2/MCP1 influences susceptibility to mucosal but not localized cutaneous leishmaniasis in Brazil. Infect Genet Evol 10:607–613
Geddes K, Rubino SJ, Magalhaes JG, Streutker C, Le Bourhis L et al (2011) Identification of an innate T helper type 17 response to intestinal bacterial pathogens. Nat Med 17:837–844
Elshafie AI, Hlin E, Hakansson LD, Elghazali G, Safi SH et al (2011) Activity and turnover of eosinophil and neutrophil granulocytes are altered in visceral leishmaniasis. Int J Parasitol 41:463–469
Pitta MG, Romano A, Cabantous S, Henri S, Hammad A et al (2009) IL-17 and IL-22 are associated with protection against human kala azar caused by Leishmania donovani. J Clin Invest 119:2379–2387
Bacellar O, Faria D, Nascimento M, Cardoso TM, Gollob KJ et al (2009) Interleukin 17 production among patients with American cutaneous leishmaniasis. J Infect Dis 200:75–78
Novoa R, Bacellar O, Nascimento M, Cardoso TM, Ramasawmy R et al (2011) IL-17 and regulatory cytokines (IL-10 and IL-27) in L. braziliensis infection. Parasite Immunol 33:132–136
Boaventura VS, Santos CS, Cardoso CR, de Andrade J, Dos Santos WL et al (2010) Human mucosal leishmaniasis: neutrophils infiltrate areas of tissue damage that express high levels of Th17-related cytokines. Eur J Immunol 40:2830–2836
Li X, Yuan FL, Lu WG, Zhao YQ, Li CW et al (2010) The role of interleukin-17 in mediating joint destruction in rheumatoid arthritis. Biochem Biophys Res Commun 397:131–135
Sato K, Suematsu A, Okamoto K, Yamaguchi A, Morishita Y et al (2006) Th17 functions as an osteoclastogenic helper T cell subset that links T cell activation and bone destruction. J Exp Med 203:2673–2682
Castellano LR, Llaguno M, Silva MV, Machado JR, Correia D et al (2011) Immunophenotyping of circulating T cells in a mucosal leishmaniasis patient coinfected with HIV. Rev Soc Bras Med Trop 44:520–521
Faria DR, Gollob KJ, Barbosa J Jr, Schriefer A, Machado PR et al (2005) Decreased in situ expression of interleukin-10 receptor is correlated with the exacerbated inflammatory and cytotoxic responses observed in mucosal leishmaniasis. Infect Immun 73:7853–7859
Stillie R, Farooq SM, Gordon JR, Stadnyk AW (2009) The functional significance behind expressing two IL-8 receptor types on PMN. J Leukoc Biol 86:529–543
Castellucci L, Jamieson SE, Miller EN, Menezes E, Oliveira J et al (2010) CXCR1 and SLC11A1 polymorphisms affect susceptibility to cutaneous leishmaniasis in Brazil: a case–control and family-based study. BMC Med Genet 11:10
Pravica V, Perrey C, Stevens A, Lee JH, Hutchinson IV (2000) A single nucleotide polymorphism in the first intron of the human IFN-gamma gene: absolute correlation with a polymorphic CA microsatellite marker of high IFN-gamma production. Hum Immunol 61:863–866
Cabrera M, Shaw MA, Sharples C, Williams H, Castes M et al (1995) Polymorphism in tumor necrosis factor genes associated with mucocutaneous leishmaniasis. J Exp Med 182:1259–1264
Matos GI, Covas Cde J, Bittar Rde C, Gomes-Silva A, Marques F et al (2007) IFNG +874 T/A polymorphism is not associated with American tegumentary leishmaniasis susceptibility but can influence Leishmania induced IFN-gamma production. BMC Infect Dis 7:33
Vargas-Inchaustegui DA, Hogg AE, Tulliano G, Llanos-Cuentas A, Arevalo J et al (2010) CXCL10 production by human monocytes in response to Leishmania braziliensis infection. Infect Immun 78:301–308
Lee EY, Lee ZH, Song YW (2009) CXCL10 and autoimmune diseases. Autoimmun Rev 8:379–383
Machado PR, Rosa ME, Costa D, Mignac M, Silva JS et al (2011) Reappraisal of the immunopathogenesis of disseminated leishmaniasis: in situ and systemic immune response. Trans R Soc Trop Med Hyg 105:438–444
Silveira FT, Lainson R, Corbett CE (2004) Clinical and immunopathological spectrum of American cutaneous leishmaniasis with special reference to the disease in Amazonian Brazil: a review. Mem Inst Oswaldo Cruz 99:239–251
Khandelwal K, Bumb RA, Mehta RD, Kaushal H, Lezama-Davila C et al (2011) A patient presenting with diffuse cutaneous leishmaniasis (DCL) as a first indicator of HIV infection in India. AmJTrop Med Hyg 85:64–65
Niamba P, Goumbri-Lompo O, Traore A, Barro-Traore F, Soudre RT (2007) Diffuse cutaneous leishmaniasis in an HIV-positive patient in western Africa. Australas J Dermatol 48:32–34
Soong L (2008) Modulation of dendritic cell function by Leishmania parasites. J Immunol 180:4355–4360
Mukbel RM, Patten C Jr, Gibson K, Ghosh M, Petersen C et al (2007) Macrophage killing of Leishmania amazonensis amastigotes requires both nitric oxide and superoxide. AmJTrop Med Hyg 76:669–675
Wang Y, Chen Y, Xin L, Beverley SM, Carlsen ED et al (2011) Differential microbicidal effects of human histone proteins H2A and H2B on Leishmania promastigotes and amastigotes. Infect Immun 79:1124–1133
Bhardwaj S, Srivastava N, Sudan R, Saha B (2010) Leishmania interferes with host cell signaling to devise a survival strategy. J Biomed Biotechnol 2010:109189
McConville MJ, Naderer T (2011) Metabolic pathways required for the intracellular survival of Leishmania. Annu Rev Microbiol 65:543–561
Bosetto MC, Giorgio S (2007) Leishmania amazonensis: multiple receptor-ligand interactions are involved in amastigote infection of human dendritic cells. Exp Parasitol 116:306–310
Boggiatto PM, Jie F, Ghosh M, Gibson-Corley KN, Ramer-Tait AE et al (2009) Altered dendritic cell phenotype in response to Leishmania amazonensis amastigote infection is mediated by MAP kinase, ERK. Am J Pathol 174:1818–1826
Wanderley JL, Moreira ME, Benjamin A, Bonomo AC, Barcinski MA (2006) Mimicry of apoptotic cells by exposing phosphatidylserine participates in the establishment of amastigotes of Leishmania (L) amazonensis in mammalian hosts. J Immunol 176:1834–1839
Wanderley JL, Barcinski MA (2010) Apoptosis and apoptotic mimicry: the Leishmania connection. Cell Mol Life Sci 67:1653–1659
Dos Santos TA, Portes Jde A, Damasceno-Sa JC, Caldas LA, de Souza W et al (2011) Phosphatidylserine exposure by Toxoplasma gondii is fundamental to balance the immune response granting survival of the parasite and of the host. PLoS One 6:e27867
Thanawastien A, Montor WR, Labaer J, Mekalanos JJ, Yoon SS (2009) Vibrio cholerae proteome-wide screen for immunostimulatory proteins identifies phosphatidylserine decarboxylase as a novel Toll-like receptor 4 agonist. PLoS Pathog 5:e1000556
Campanelli AP, Brodskyn CI, Boaventura V, Silva C, Roselino AM et al (2010) Chemokines and chemokine receptors coordinate the inflammatory immune response in human cutaneous leishmaniasis. Hum Immunol 71:1220–1227
Carrada G, Caneda C, Salaiza N, Delgado J, Ruiz A et al (2007) Monocyte cytokine and costimulatory molecule expression in patients infected with Leishmania mexicana. Parasite Immunol 29:117–126
Macedo AB, Sanchez-Arcila JC, Schubach AO, Mendonca SC, Marins-Dos-Santos A et al (2012) Multifunctional CD4 T cells in patients with American cutaneous leishmaniasis. Clin Exp Immunol 167:505–513
Hernandez-Ruiz J, Salaiza-Suazo N, Carrada G, Escoto S, Ruiz-Remigio A et al (2010) CD8 cells of patients with diffuse cutaneous leishmaniasis display functional exhaustion: the latter is reversed, in vitro, by TLR2 agonists. PLoS Negl Trop Dis 4:e871
Salaiza-Suazo N, Volkow P, Tamayo R, Moll H, Gillitzer R et al (1999) Treatment of two patients with diffuse cutaneous leishmaniasis caused by Leishmania mexicana modifies the immunohistological profile but not the disease outcome. Trop Med Int Health 4:801–811
Castilho TM, Goldsmith-Pestana K, Lozano C, Valderrama L, Saravia NG et al (2010) Murine model of chronic L. (Viannia) panamensis infection: role of IL-13 in disease. Eur J Immunol 40:2816–2829
Martinez JE, Valderrama L, Gama V, Leiby DA, Saravia NG (2000) Clonal diversity in the expression and stability of the metastatic capability of Leishmania guyanensis in the golden hamster. J Parasitol 86:792–799
Pereira BA, Alves CR (2008) Immunological characteristics of experimental murine infection with Leishmania (Leishmania) amazonensis. Vet Parasitol 158:239–255
Soong L, Chang CH, Sun J, Longley BJ Jr, Ruddle NH et al (1997) Role of CD4+ T cells in pathogenesis associated with Leishmania amazonensis infection. J Immunol 158:5374–5383
Wanasen N, Xin L, Soong L (2008) Pathogenic role of B cells and antibodies in murine Leishmania amazonensis infection. Int J Parasitol 38:417–429
Soong L (2012) Subversion and utilization of host innate defense by Leishmania amazonensis. Frontiers Immunol 3:1–7
Novais FO, Santiago RC, Bafica A, Khouri R, Afonso L et al (2009) Neutrophils and macrophages cooperate in host resistance against Leishmania braziliensis infection. J Immunol 183:8088–8098
Vargas-Inchaustegui DA, Xin L, Soong L (2008) Leishmania braziliensis infection induces dendritic cell activation, ISG15 transcription, and the generation of protective immune responses. J Immunol 180:7537–7545
Melby PC, Chandrasekar B, Zhao W, Coe JE (2001) The hamster as a model of human visceral leishmaniasis: progressive disease and impaired generation of nitric oxide in the face of a prominent Th1-like cytokine response. J Immunol 166:1912–1920
Silveira FT, Lainson R, Corbett CE (2005) Further observations on clinical, histopathological, and immunological features of borderline disseminated cutaneous leishmaniasis caused by Leishmania (Leishmania) amazonensis. Mem Inst Oswaldo Cruz 100:525–534
Xin L, Li Y, Soong L (2007) Role of interleukin-1β in activating the CD11chigh CD45RB− dendritic cell subset and priming Leishmania amazonensis-specific CD4+ T cells in vitro and in vivo. Infect Immun 75:5018–5026
Xin L, Wanderley JL, Wang Y, Vargas-Inchaustegui DA, Soong L (2011) The magnitude of CD4+ T-cell activation rather than TCR diversity determines the outcome of Leishmania infection in mice. Parasite Immunol 33:170–180
Castilho-Martins EA, Laranjeira da Silva MF, dos Santos MG, Muxel SM, Floeter-Winter LM (2011) Axenic Leishmania amazonensis promastigotes sense both the external and internal arginine pool distinctly regulating the two transporter-coding genes. PLoS One 6:e27818
Crescente JA, Silveira FT, Lainson R, Gomes CM, Laurenti MD et al (2009) A cross-sectional study on the clinical and immunological spectrum of human Leishmania (L.) infantum chagasi infection in the Brazilian Amazon region. Trans R Soc Trop Med Hyg 103:1250–1256
Silveira FT, Lainson R, Crescente JA, de Souza AA, Campos MB et al (2010) A prospective study on the dynamics of the clinical and immunological evolution of human Leishmania (L.) infantum chagasi infection in the Brazilian Amazon region. Trans R Soc Trop Med Hyg 104:529–535
Hailu A, Gramiccia M, Kager PA (2009) Visceral leishmaniasis in Aba-Roba, south-western Ethiopia: prevalence and incidence of active and subclinical infections. Ann Trop Med Parasitol 103:659–670
Hailu A, van Baarle D, Knol GJ, Berhe N, Miedema F et al (2005) T cell subset and cytokine profiles in human visceral leishmaniasis during active and asymptomatic or sub-clinical infection with Leishmania donovani. Clin Immunol 117:182–191
Hailu A, van der Poll T, Berhe N, Kager PA (2004) Elevated plasma levels of interferon (IFN)-gamma, IFN-gamma inducing cytokines, and IFN-gamma inducible CXC chemokines in visceral leishmaniasis. AmJTrop Med Hyg 71:561–567
Ghalib HW, Piuvezam MR, Skeiky YA, Siddig M, Hashim FA et al (1993) Interleukin 10 production correlates with pathology in human Leishmania donovani infections. J Clin Invest 92:324–329
Kenney RT, Sacks DL, Gam AA, Murray HW, Sundar S (1998) Splenic cytokine responses in Indian kala-azar before and after treatment. J Infect Dis 177:815–818
Karp CL, el-Safi SH, Wynn TA, Satti MM, Kordofani AM et al (1993) In vivo cytokine profiles in patients with kala-azar. Marked elevation of both interleukin-10 and interferon-gamma [see comments]. J Clin Invest 91:1644–1648
Gidwani K, Jones S, Kumar R, Boelaert M, Sundar S (2011) Interferon-gamma release assay (modified QuantiFERON) as a potential marker of infection for Leishmania donovani, a proof of concept study. PLoS Negl Trop Dis 5:e1042
Melby PC, Valencia-Pacheco G, Andrade-Narvaez F (1996) Induction of macrophage killing of Leishmania donovani by human CD4+ T cell clones. Arch Med Res 27:473–479
Khader SA, Gopal R (2010) IL-17 in protective immunity to intracellular pathogens. Virulence 1:423–427
Nylen S, Sacks D (2007) Interleukin-10 and the pathogenesis of human visceral leishmaniasis. Trends Immunol 28:378–384
Wilson ME, Jeronimo SM, Pearson RD (2005) Immunopathogenesis of infection with the visceralizing Leishmania species. Microb Pathog 38:147–160
Sacks D, Noben-Trauth N (2002) The immunology of susceptibility and resistance to Leishmania major in mice. Nat Rev Immunol 2:845–858
Nylen S, Maurya R, Eidsmo L, Manandhar KD, Sundar S et al (2007) Splenic accumulation of IL-10 mRNA in T cells distinct from CD4+CD25+ (Foxp3) regulatory T cells in human visceral leishmaniasis. J Exp Med 204:805–817
Ansari NA, Saluja S, Salotra P (2006) Elevated levels of interferon-gamma, interleukin-10, and interleukin-6 during active disease in Indian kala azar. Clin Immunol 119:339–345
Kurkjian KM, Mahmutovic AJ, Kellar KL, Haque R, Bern C et al (2006) Multiplex analysis of circulating cytokines in the sera of patients with different clinical forms of visceral leishmaniasis. Cytometry A 69:353–358
Caldas A, Favali C, Aquino D, Vinhas V, van Weyenbergh J et al (2005) Balance of IL-10 and interferon-gamma plasma levels in human visceral leishmaniasis: implications in the pathogenesis. BMC Infect Dis 5:113
Verma S, Kumar R, Katara GK, Singh LC, Negi NS et al (2010) Quantification of parasite load in clinical samples of leishmaniasis patients: IL-10 level correlates with parasite load in visceral leishmaniasis. PLoS One 5:e10107
Gautam S, Kumar R, Maurya R, Nylen S, Ansari N et al (2011) IL-10 neutralization promotes parasite clearance in splenic aspirate cells from patients with visceral leishmaniasis. J Infect Dis 204:1134–1137
Ansari NA, Kumar R, Gautam S, Nylen S, Singh OP et al (2011) IL-27 and IL-21 are associated with T cell IL-10 responses in human visceral leishmaniasis. J Immunol 186:3977–3985
Santos-Oliveira JR, Regis EG, Leal CR, Cunha RV, Bozza PT et al (2011) Evidence that lipopolysaccharide may contribute to the cytokine storm and cellular activation in patients with visceral leishmaniasis. PLoS Negl Trop Dis 5:e1198
Belkaid Y, Piccirillo CA, Mendez S, Shevach EM, Sacks DL (2002) CD4+CD25+ regulatory T cells control Leishmania major persistence and immunity. Nature 420:502–507
Rodrigues OR, Marques C, Soares-Clemente M, Ferronha MH, Santos-Gomes GM (2009) Identification of regulatory T cells during experimental Leishmania infantum infection. Immunobiology 214:101–111
Saha S, Mondal S, Ravindran R, Bhowmick S, Modak D et al (2007) IL-10- and TGF-beta-mediated susceptibility in kala-azar and post-kala-azar dermal leishmaniasis: the significance of amphotericin B in the control of Leishmania donovani infection in India. J Immunol 179:5592–5603
Maurya R, Kumar R, Prajapati VK, Manandhar KD, Sacks D et al (2010) Human visceral leishmaniasis is not associated with expansion or accumulation of Foxp3+ CD4 cells in blood or spleen. Parasite Immunol 32:479–483
Rai AK, Thakur CP, Singh A, Seth T, Srivastava SK et al (2012) Regulatory T cells suppress T cell activation at the pathologic site of human visceral leishmaniasis. PLoS One 7:e31551
Katara GK, Ansari NA, Verma S, Ramesh V, Salotra P (2011) Foxp3 and IL-10 expression correlates with parasite burden in lesional tissues of post kala azar dermal leishmaniasis (PKDL) patients. PLoS Negl Trop Dis 5:e1171
Malafaia G (2009) Protein-energy malnutrition as a risk factor for visceral leishmaniasis: a review. Parasite Immunol 31:587–596
Collin S, Davidson R, Ritmeijer K, Keus K, Melaku Y et al (2004) Conflict and kala-azar: determinants of adverse outcomes of kala-azar among patients in southern Sudan. Clin Infect Dis 38:612–619
Kolaczinski JH, Hope A, Ruiz JA, Rumunu J, Richer M et al (2008) Kala-azar epidemiology and control, southern Sudan. Emerg Infect Dis 14:664–666
Marlet MV, Sang DK, Ritmeijer K, Muga RO, Onsongo J et al (2003) Emergence or re-emergence of visceral leishmaniasis in areas of Somalia, north-eastern Kenya, and south-eastern Ethiopia in 2000–01. Trans R Soc Trop Med Hyg 97:515–518
Maciel BL, Lacerda HG, Queiroz JW, Galvao J, Pontes NN et al (2008) Association of nutritional status with the response to infection with Leishmania chagasi. AmJTrop Med Hyg 79:591–598
Anstead GM, Chandrasekar B, Zhang Q, Melby PC (2003) Multinutrient undernutrition dysregulates the resident macrophage proinflammatory cytokine network, nuclear factor-kappaB activation, and nitric oxide production. J Leukoc Biol 74:982–991
Anstead GM, Chandrasekar B, Zhao W, Yang J, Perez LE et al (2001) Malnutrition alters the innate immune response and increases early visceralization following Leishmania donovani infection. Infect Immun 69:4709–4718
Anstead GM, Zhang Q, Melby PC (2009) Malnutrition promotes prostaglandin over leukotriene production and dysregulates eicosanoid-cytokine crosstalk in activated resident macrophages. Prostaglandins Leukot Essent Fatty Acids 81:41–51
Malafaia G, Serafim TD, Silva ME, Pedrosa ML, Rezende SA (2009) Protein-energy malnutrition decreases immune response to Leishmania chagasi vaccine in BALB/c mice. Parasite Immunol 31:41–49
Cota GF, de Sousa MR, Rabello A (2011) Predictors of visceral leishmaniasis relapse in HIV-infected patients: a systematic review. PLoS Negl Trop Dis 5:e1153
Zhao C, Cantin R, Breton M, Papadopoulou B, Tremblay MJ (2005) DC-SIGN-mediated transfer of HIV-1 is compromised by the ability of Leishmania infantum to exploit DC-SIGN as a ligand. J Infect Dis 191:1665–1669
Zhao C, Papadopoulou B, Tremblay MJ (2004) Leishmania infantum enhances human immunodeficiency virus type-1 replication in primary human macrophages through a complex cytokine network. Clin Immunol 113:81–88
Zhao C, Papadopoulou B, Tremblay MJ (2004) Leishmania infantum promotes replication of HIV type 1 in human lymphoid tissue cultured ex vivo by inducing secretion of the proinflammatory cytokines TNF-alpha and IL-1 alpha. J Immunol 172:3086–3093
Garg R, Barat C, Ouellet M, Lodge R, Tremblay MJ (2009) Leishmania infantum amastigotes enhance HIV-1 production in cocultures of human dendritic cells and CD4 T cells by inducing secretion of IL-6 and TNF-alpha. PLoS Negl Trop Dis 3:e441
Bossolasco S, Gaiera G, Olchini D, Gulletta M, Martello L et al (2003) Real-time PCR assay for clinical management of human immunodeficiency virus-infected patients with visceral leishmaniasis. J Clin Microbiol 41:5080–5084
Santos-Oliveira JR, Giacoia-Gripp CB, Alexandrino de Oliveira P, Amato VS, Lindoso JA et al (2010) High levels of T lymphocyte activation in Leishmania-HIV-1 co-infected individuals despite low HIV viral load. BMC Infect Dis 10:358
Stanley AC, Engwerda CR (2007) Balancing immunity and pathology in visceral leishmaniasis. Immunol Cell Biol 85:138–147
Kaye PM, Svensson M, Ato M, Maroof A, Polley R et al (2004) The immunopathology of experimental visceral leishmaniasis. Immunol Rev 201:239–253
Rosas LE, Snider HM, Barbi J, Satoskar AA, Lugo-Villarino G et al (2006) Cutting edge: STAT1 and T-bet play distinct roles in determining outcome of visceral leishmaniasis caused by Leishmania donovani. J Immunol 177:22–25
Beattie L, Phillips R, Brown N, Owens BM, Chauhan N et al (2011) Interferon regulatory factor 7 contributes to the control of Leishmania donovani in the mouse liver. Infect Immun 79:1057–1066
Paun A, Bankoti R, Joshi T, Pitha PM, Stager S (2011) Critical role of IRF-5 in the development of T helper 1 responses to Leishmania donovani infection. PLoS Pathog 7:e1001246
Ato M, Maroof A, Zubairi S, Nakano H, Kakiuchi T et al (2006) Loss of dendritic cell migration and impaired resistance to Leishmania donovani infection in mice deficient in CCL19 and CCL21. J Immunol 176:5486–5493
McFarlane E, Perez C, Charmoy M, Allenbach C, Carter KC et al (2008) Neutrophils contribute to development of a protective immune response during onset of infection with Leishmania donovani. Infect Immun 76:532–541
Murray HW, Nathan CF (1999) Macrophage microbicidal mechanisms in vivo: reactive nitrogen versus oxygen intermediates in the killing of intracellular visceral Leishmania donovani. J Exp Med 189:741–746
Murray HW, Xiang Z, Ma X (2006) Responses to Leishmania donovani in mice deficient in both phagocyte oxidase and inducible nitric oxide synthase. AmJTrop Med Hyg 74:1013–1015
Murray HW (2001) Tissue granuloma structure-function in experimental visceral leishmaniasis. Int J Exp Pathol 82:249–267
McFarlane E, Carter KC, McKenzie AN, Kaye PM, Brombacher F et al (2011) Endogenous IL-13 plays a crucial role in liver granuloma maturation during Leishmania donovani infection, independent of IL-4Ralpha-responsive macrophages and neutrophils. J Infect Dis 204:36–43
Stager S, Alexander J, Carter KC, Brombacher F, Kaye PM (2003) Both interleukin-4 (IL-4) and IL-4 receptor alpha signaling contribute to the development of hepatic granulomas with optimal antileishmanial activity. Infect Immun 71:4804–4807
Murphy ML, Wille U, Villegas EN, Hunter CA, Farrell JP (2001) IL-10 mediates susceptibility to Leishmania donovani infection. Eur J Immunol 31:2848–2856
Murray HW, Moreira AL, Lu CM, DeVecchio JL, Matsuhashi M et al (2003) Determinants of response to interleukin-10 receptor blockade immunotherapy in experimental visceral leishmaniasis. J Infect Dis 188:458–464
Engwerda CR, Ato M, Cotterell SE, Mynott TL, Tschannerl A et al (2002) A role for tumor necrosis factor-alpha in remodeling the splenic marginal zone during Leishmania donovani infection. Am J Pathol 161:429–437
Ato M, Stager S, Engwerda CR, Kaye PM (2002) Defective CCR7 expression on dendritic cells contributes to the development of visceral leishmaniasis. Nat Immunol 3:1185–1191
Mebius RE, Kraal G (2005) Structure and function of the spleen. Nat Rev Immunol 5:606–616
Dalton JE, Maroof A, Owens BM, Narang P, Johnson K et al (2010) Inhibition of receptor tyrosine kinases restores immunocompetence and improves immune-dependent chemotherapy against experimental leishmaniasis in mice. J Clin Invest 120:1204–1216
Yurdakul P, Dalton J, Beattie L, Brown N, Erguven S et al (2011) Compartment-specific remodeling of splenic micro-architecture during experimental visceral leishmaniasis. Am J Pathol 179:23–29
Cotterell SE, Engwerda CR, Kaye PM (2000) Enhanced hematopoietic activity accompanies parasite expansion in the spleen and bone marrow of mice infected with Leishmania donovani. Infect Immun 68:1840–1848
Cotterell SE, Engwerda CR, Kaye PM (2000) Leishmania donovani infection of bone marrow stromal macrophages selectively enhances myelopoiesis, by a mechanism involving GM-CSF and TNF-alpha. Blood 95:1642–1651
Osorio EY, Zhao W, Espitia C, Saldarriaga O, Hawel L et al (2012) Progressive visceral leishmaniasis is driven by dominant parasite-induced STAT6 activation and STAT6-dependent host arginase 1 expression. PLoS Pathog 8:e1002417
Osorio Y, Travi BL, Renslo AR, Peniche AG, Melby PC (2011) Identification of small molecule lead compounds for visceral leishmaniasis using a novel ex vivo splenic explant model system. PLoS Negl Trop Dis 5:e962
Nieto A, Dominguez-Bernal G, Orden JA, De La Fuente R, Madrid-Elena N et al (2011) Mechanisms of resistance and susceptibility to experimental visceral leishmaniosis: BALB/c mouse versus Syrian hamster model. Vet Res 42:39
Gifawesen C, Farrell JP (1989) Comparison of T-cell responses in self-limiting versus progressive visceral Leishmania donovani infections in golden hamsters. Infect Immun 57:3091–3096
Banerjee R, Kumar S, Sen A, Mookerjee A, Mukherjee P et al (2011) TGF-beta-regulated tyrosine phosphatases induce lymphocyte apoptosis in Leishmania donovani-infected hamsters. Immunol Cell Biol 89:466–474
Melby PC, Chandrasekar B, Zhao W, Coe JE (2001) The hamster as a model of human visceral leishmaniasis: progressive disease and impaired generation of nitric oxide in the face of a prominent Th1-like response. J Immunol 166:1912–1920
Perez LE, Chandrasekar B, Saldarriaga OA, Zhao W, Arteaga LT et al (2006) Reduced nitric oxide synthase 2 (NOS2) promoter activity in the Syrian hamster renders the animal functionally deficient in NOS2 activity and unable to control an intracellular pathogen. J Immunol 176:5519–5528
Saldarriaga OA, Travi BL, Ghosh Choudhury G, Melby PC (2012) Identification of hamster inducible Nitric Oxide Synthase (iNOS) promoter sequences that influence basal and inducible iNOS expression. J Leukoc Biol 92:205–218
Biswas A, Bhattacharya A, Kar S, Das PK (2011) Expression of IL-10-triggered STAT3-dependent IL-4Ralpha is required for induction of arginase 1 in visceral leishmaniasis. Eur J Immunol 41:992–1003
Olivier M, Gregory DJ, Forget G (2005) Subversion mechanisms by which Leishmania parasites can escape the host immune response: a signaling point of view. Clin Microbiol Rev 18:293–305
Lambertz U, Silverman JM, Nandan D, McMaster WR, Clos J et al (2012) Secreted virulence factors and immune evasion in visceral leishmaniasis. J Leukoc Biol 91:887–899
Nandan D, Reiner NE (2005) Leishmania donovani engages in regulatory interference by targeting macrophage protein tyrosine phosphatase SHP-1. Clin Immunol 114:266–277
Nandan D, Yi T, Lopez M, Lai C, Reiner NE (2002) Leishmania EF-1alpha activates the Src homology 2 domain containing tyrosine phosphatase SHP-1 leading to macrophage deactivation. J Biol Chem 277:50190–50197
Nandan D, Tran T, Trinh E, Silverman JM, Lopez M (2007) Identification of Leishmania fructose-1,6-bisphosphate aldolase as a novel activator of host macrophage Src homology 2 domain containing protein tyrosine phosphatase SHP-1. Biochem Biophys Res Commun 364:601–607
Gomez MA, Contreras I, Halle M, Tremblay ML, McMaster RW et al (2009) Leishmania GP63 alters host signaling through cleavage-activated protein tyrosine phosphatases. Sci Signal 2:ra58
Shadab M, Ali N (2011) Evasion of host defence by Leishmania donovani: subversion of signaling pathways. Mol Biol Int 2011:343961
Kar S, Ukil A, Sharma G, Das PK (2010) MAPK-directed phosphatases preferentially regulate pro- and anti-inflammatory cytokines in experimental visceral leishmaniasis: involvement of distinct protein kinase C isoforms. J Leukoc Biol 88:9–20
Basu Ball W, Kar S, Mukherjee M, Chande AG, Mukhopadhyaya R et al (2011) Uncoupling protein 2 negatively regulates mitochondrial reactive oxygen species generation and induces phosphatase-mediated anti-inflammatory response in experimental visceral leishmaniasis. J Immunol 187:1322–1332
Forget G, Gregory DJ, Whitcombe LA, Olivier M (2006) Role of host protein tyrosine phosphatase SHP-1 in Leishmania donovani-induced inhibition of nitric oxide production. Infect Immun 74:6272–6279
Nandan D, Camargo de Oliveira C, Moeenrezakhanlou A, Lopez M, Silverman JM et al (2012) Myeloid cell IL-10 production in response to Leishmania involves inactivation of glycogen synthase kinase-3beta downstream of phosphatidylinositol-3 kinase. J Immunol 188:367–378
Sen S, Roy K, Mukherjee S, Mukhopadhyay R, Roy S (2011) Restoration of IFNgammaR subunit assembly, IFNgamma signaling and parasite clearance in Leishmania donovani infected macrophages: role of membrane cholesterol. PLoS Pathog 7:e1002229
Peters NC, Egen JG, Secundino N, Debrabant A, Kimblin N et al (2008) In vivo imaging reveals an essential role for neutrophils in leishmaniasis transmitted by sand flies. Science 321:970–974
Ribeiro-Gomes FL, Peters NC, Debrabant A, Sacks DL (2012) Efficient capture of infected neutrophils by dendritic cells in the skin inhibits the early anti-Leishmania response. PLoS Pathog 8:e1002536
Kautz-Neu K, Kostka SL, Dinges S, Iwakura Y, Udey MC et al (2011) IL-1 signalling is dispensable for protective immunity in Leishmania-resistant mice. Exp Dermatol 20:76–78
Kautz-Neu K, Kostka SL, Dinges S, Iwakura Y, Udey MC et al (2011) A role for leukocyte-derived IL-1RA in DC homeostasis revealed by increased susceptibility of IL-1RA-deficient mice to cutaneous leishmaniasis. J Invest Dermatol 131:1650–1659
Gaur U, Roberts SC, Dalvi RP, Corraliza I, Ullman B et al (2007) An effect of parasite-encoded arginase on the outcome of murine cutaneous leishmaniasis. J Immunol 179:8446–8453
Giudice A, Camada I, Leopoldo PT, Pereira JM, Riley LW et al (2007) Resistance of Leishmania (Leishmania) amazonensis and Leishmania (Viannia) braziliensis to nitric oxide correlates with disease severity in tegumentary leishmaniasis. BMC Infect Dis 7:7
Souza AS, Giudice A, Pereira JM, Guimaraes LH, de Jesus AR et al (2010) Resistance of Leishmania (Viannia) braziliensis to nitric oxide: correlation with antimony therapy and TNF-alpha production. BMC Infect Dis 10:209
Sarkar A, Ghosh S, Pakrashi S, Roy D, Sen S et al (2012) Leishmania strains causing self-healing cutaneous leishmaniasis have greater susceptibility towards oxidative stress. Free Radic Res 46:665–673
Nandan D, Lo R, Reiner NE (1999) Activation of phosphotyrosine phosphatase activity attenuates mitogen-activated protein kinase signaling and inhibits c-FOS and nitric oxide synthase expression in macrophages infected with Leishmania donovani. Infect Immun 67:4055–4063
Prive C, Descoteaux A (2000) Leishmania donovani promastigotes evade the activation of mitogen-activated protein kinases p38, c-Jun N-terminal kinase, and extracellular signal-regulated kinase-1/2 during infection of naive macrophages. Eur J Immunol 30:2235–2244
Ghosh S, Bhattacharyya S, Das S, Raha S, Maulik N et al (2001) Generation of ceramide in murine macrophages infected with Leishmania donovani alters macrophage signaling events and aids intracellular parasitic survival. Mol Cell Biochem 223:47–60
Chandra D, Naik S (2008) Leishmania donovani infection down-regulates TLR2-stimulated IL-12p40 and activates IL-10 in cells of macrophage/monocytic lineage by modulating MAPK pathways through a contact-dependent mechanism. Clin Exp Immunol 154:224–234
Ghosh S, Bhattacharyya S, Sirkar M, Sa GS, Das T et al (2002) Leishmania donovani suppresses activated protein 1 and NF-kappaB activation in host macrophages via ceramide generation: involvement of extracellular signal-regulated kinase. Infect Immun 70:6828–6838
Ray M, Gam AA, Boykins RA, Kenney RT (2000) Inhibition of interferon-gamma signaling by Leishmania donovani. J Infect Dis 181:1121–1128
Matte C, Descoteaux A (2010) Leishmania donovani amastigotes impair gamma interferon-induced STAT1alpha nuclear translocation by blocking the interaction between STAT1alpha and importin-alpha5. Infect Immun 78:3736–3743
Forget G, Gregory DJ, Olivier M (2005) Proteasome-mediated degradation of STAT1alpha following infection of macrophages with Leishmania donovani. J Biol Chem 280:30542–30549
Blanchette J, Racette N, Faure R, Siminovitch KA, Olivier M (1999) Leishmania-induced increases in activation of macrophage SHP-1 tyrosine phosphatase are associated with impaired IFN-gamma-triggered JAK2 activation. Eur J Immunol 29:3737–3744
Holm A, Tejle K, Gunnarsson T, Magnusson KE, Descoteaux A et al (2003) Role of protein kinase C alpha for uptake of unopsonized prey and phagosomal maturation in macrophages. Biochem Biophys Res Commun 302:653–658
Dey R, Majumder N, Bhattacharjee S, Majumdar SB, Banerjee R et al (2007) Leishmania donovani-induced ceramide as the key mediator of Akt dephosphorylation in murine macrophages: role of protein kinase Czeta and phosphatase. Infect Immun 75:2136–2142
Dey R, Sarkar A, Majumder N, Bhattacharyya Majumdar S, Roychoudhury K et al (2005) Regulation of impaired protein kinase C signaling by chemokines in murine macrophages during visceral leishmaniasis. Infect Immun 73:8334–8344
Bhattacharyya S, Ghosh S, Sen P, Roy S, Majumdar S (2001) Selective impairment of protein kinase C isotypes in murine macrophage by Leishmania donovani. Mol Cell Biochem 216:47–57
Chan MM, Adapala N, Chen C (2012) Peroxisome proliferator-activated receptor-gamma-mediated polarization of macrophages in Leishmania infection. PPAR Res 2012:796235
Cheekatla SS, Aggarwal A, Naik S (2012) mTOR signaling pathway regulates the IL-12/IL-10 axis in Leishmania donovani infection. Med Microbiol Immunol 201:37–46
Acknowledgments
The authors thank Mardelle Susman for proofreading this article. This work was supported by NIH grants AI043003 and AI076849 (to L.S.), and NIH grant AI061624 (to P.C.M.). C.A.H. is supported by a NIH T32 postdoctoral training grant (AI00753613).
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is a contribution to the special issue on Immunoparasitology—Guest Editor: Miguel Stadecker
Rights and permissions
About this article
Cite this article
Soong, L., Henard, C.A. & Melby, P.C. Immunopathogenesis of non-healing American cutaneous leishmaniasis and progressive visceral leishmaniasis. Semin Immunopathol 34, 735–751 (2012). https://doi.org/10.1007/s00281-012-0350-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00281-012-0350-8