
Abstract
Purpose
This study was conducted to examine the absorption and tissue distribution characteristics of paclitaxel-loaded DHP 107, a Cremophor EL-free, mucoadhesive lipid oral dosage form.
Methods
DHP 107 was orally administered to mice at 10, 20 and 40 mg/kg doses. For comparison purposes, Taxol was i.v. injected at 5, 10 and 20 mg/kg doses. Drug levels were determined in plasma and tissues by validated HPLC assays. The absolute bioavailability and the relative distribution to various tissues were calculated as a function of dose.
Results
The dose-normalized plasma AUCDHP 107/AUCTaxol ratios calculated at comparable AUC values ranged from 14.6 to 29.0%. In contrast, relative tissue distribution ratios calculated as the dose-normalized AUCDHP 107/AUCTaxol were as high as 342.0, 139.0, 112.9 and 108.2% for stomach, small intestine, large intestine and ovary, respectively.
Conclusions
Oral administration of DHP 107 provided a substantial systemic absorption of paclitaxel. Furthermore, the relative distribution ratios of DHP 107 at doses of 20 and 40 mg/kg were higher for stomach, small intestine, large intestine, and ovary than the systemic bioavailability, providing a basis for therapeutic advantages.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Paclitaxel is an anticancer drug widely used for the treatment of various tumors, including lung, ovarian and breast cancers [1, 2]. The anticancer activity of paclitaxel is known to be mediated by binding to tubulin, stabilization of microtubules, blockade of cell cycling at the G2-phase and induction of apoptosis [3–5]. Being practically insoluble (<1 μg/ml), paclitaxel is commercially formulated in a mixture of Cremophor EL and dehydrated ethanol (1:1, v/v) (Taxol, paclitaxel 6 mg/ml, Bristol-Myers Squibb Co., Princeton, NJ, USA). Cremophor EL is known to cause various biological responses, including the histamine release, hypersensitivity reactions and alterations in the pharmacokinetics of paclitaxel [6–8]. To date, Cremophor EL-free i.v. formulations such as albumin-bound nanoparticles (Abraxane, American Bioscience, Inc., Santa Monica, CA, USA) and lyophilized polymeric micelles (Genexol-PM, Samyang Co. Seoul, Korea) have been developed to avoid toxicities associated with this solvent, [9–11].
When given orally, paclitaxel is poorly absorbed primarily due to a pre-systemic metabolism and P-glycoprotein-mediated efflux across the mucosal cells of the small intestine [12–14]. The absolute bioavailability of paclitaxel is low, e.g., 2.0 and 4.6% after oral administration of Taxol and a microemulsion preparation, respectively [15, 16]. Attempts have been made to develop various oral dosage forms to increase the systemic absorption of paclitaxel, including microemulsions [15, 17], nanoemulsions [18, 19], lipid suspension [20] and micelles [21, 22]. DHP 107 is a novel paclitaxel-loaded oral mucoadhesive lipid dosage form free of Cremophor EL (PCT WO 2004/009075 A1). The antitumor activity of DHP 107 has been reported in non-small cell lung carcinoma-bearing mice after oral administration [23]. Upon oral administration to mice, DHP 107 is spontaneously changed to <100 μm droplets and micelles in the intestine, adhered to mucoepithelial cells and systemically absorbed via a lipid uptake mechanism [23]. This novel oral dosage form is currently under clinical investigation in patients with metastatic cancers.
The present study reports the systemic absorption and tissue distribution characteristics of DHP 107 in mice following oral administration at 10, 20 and 40 mg/kg doses. For comparison purposes, Taxol was intravenously injected at 5, 10 and 20 mg/kg doses. Discussions are provided on the effect of dose size on the plasma pharmacokinetics and the relative extent of drug distribution to various tissues.
Materials and methods
Chemicals
Paclitaxel, Taxol (paclitaxel 6 mg/ml) (Bristol-Myers Squibb Pharmaceutical Group, Montreal, Quebec, Canada) and DHP107 (paclitaxel 10 mg/ml) were provided by Dae Hwa Pharm. Co. (Seoul, Korea). Triethylamine and p-hydroxy benzoic acid n-butyl ester (butyl paraben) were purchased from Sigma Chemical Co. (St. Louis, MO, USA). Methanol, acetonitrile, t-butyl methyl ether and distilled water (all HPLC grades) were purchased from Mallinckrodt Baker, Inc. (Phillipsburg, NJ, USA). Phosphoric acid and saline were purchased from Aldrich Chemical Co. (Milwaukee, WI, USA) and Choong Wae Pharma Co. (Seoul, Korea), respectively.
Animals
Female ICR-mice (28–35 g) (Samtako Co., Osan, Korea) were used in the study. The animals were cared for in accordance with the National Institutes of Health (NIH) guidelines for the Care and Use of Laboratory Animals (NIH publication 85-23, revised 1985), and the animal protocol was approved by the Institutional Animal Care and Use Committee of Sungkyunkwan University. The mice were kept in plastic cages with free access to standard mouse diet (Superfeed Co., Wonjoo, Korea) and water. The animals were maintained in an animal facility at a temperature of 23 ± 2°C with a 12 h of light/dark cycle and relative humidity of 50 ± 10%.
Drug administration and sample preparation
A total of 192 mice were divided into 6 groups (n = 32 per group). Three groups of mice received DHP 107 (paclitaxel 10 mg/ml) by oral gavages at 10, 20 and 40 mg/kg doses. Immediately prior to administration, DHP 107 (melting point 33–35°C) was pre-warmed by holding briefly in hand to change the semisolid wax to a liquid state. The other three groups of mice received Taxol by tail vein injection at 5, 10 and 20 mg/kg doses. To minimize the pharmacokinetic variability resulting from interaction between Cremophor EL and paclitaxel, the volume of Cremophor EL was kept constant by diluting Taxol with isotonic saline to 1, 2 and 4 mg/ml concentrations for 5, 10 and 20 mg/kg doses, respectively. Blood samples were taken by cardiac puncture under light anesthesia with ether at 0, 1, 2, 4, 6, 8, 12 and 24 h after oral administration of DHP 107 and 0, 0.5, 1, 2, 3, 6, 12 and 24 h after i.v. injection of Taxol (n = 4 per each sampling time). Plasma samples were obtained by centrifugation of collected blood at 7,000 rpm (3,500×g) for 10 min (MicroV centrifuge, Fisher Scientific Co., Pittsburgh, PA, USA) and kept at −70°C until drug analysis. After collection of blood samples from mice, stomach, small intestine, large intestine, liver, kidney, spleen, lung and ovary were excised (n = 4 per each sampling time). The stomach, small intestine and large intestine were emptied and rinsed thoroughly 3 times with saline. All excised tissues were blot dried, weighed and homogenized (Tissue Tearor, Biospec Co., Bartlesville, OK, USA) with appropriate volumes of saline, e.g., 5 ml for small intestine, large intestine and liver, 1.5 ml for stomach and kidney, 1 ml for lung and spleen, and 0.5 ml for ovary. Obtained tissue homogenates were kept at −70°C until drug analysis.
Preparation of stock solutions
Stock solutions of paclitaxel and butyl paraben (internal standard) were prepared in methanol at 100 μg/ml concentrations. Working standard solutions of paclitaxel were prepared by dilution of the stock solution with methanol at 1,00000, 50,000, 10,000, 5,000, 1,000, 500, 100 ng/ml. The internal standard stock solution (100 μg/ml) was used in tissue drug analysis, and a further diluted solution (25 μg/ml) was used in plasma drug analysis.
Extraction procedures
For drug analysis in plasma, standard curves were constructed by spiking 10 μl of working stock solutions to blank plasma (100 μl each) to provide paclitaxel concentrations at 10,000, 5,000, 1,000, 500, 100, 50 and 10 ng/ml. The plasma was spiked with 10 μl of the internal standard solution and 3 ml of t-butyl methyl ether, mixed on a vortex mixer for 10 min and centrifuged for 10 min at 4,000 rpm (3700×g) (Union 32R plus, Hanil Science Industrial Co., Inchon, Korea). The upper organic layer was transferred to a glass test tube and evaporated at 40°C under a gentle stream of nitrogen. The residue was reconstituted with 100 μl of the mobile phase consisting of acetonitrile and 0.1% triethylamine in distilled water with pH modified to 3.0 by phosphoric acid (54:46). The reconstituted solution was mixed on a vortex mixer for 10 min, centrifuged for 10 min at 4,000 rpm (3,700×g), and a portion (60 μl) was injected into HPLC.
For drug analysis in tissues, standard curves were constructed by spiking 10 μl of working stock solutions to blank tissue homogenates (100 μl each) to provide paclitaxel concentrations of 10,000, 5,000, 1,000, 500, 100, 50 and 10 ng/ml for stomach, large intestine, kidney, spleen and ovary, 10,000, 5,000, 1,000, 500, 100, 50 and 20 ng/ml for liver, and 10,000, 5,000, 1,000, 500, 100 and 50 ng/ml for small intestine. Stomach, small intestine, kidney and lung homogenates were extracted with t-butyl methyl ether after addition of 20 μl of 0.5% formic acid, liver extracted with t-butyl methyl ether after addition of 20 μl of 1N HCl, and large intestine, spleen and ovary extracted without pH modification. Otherwise, the extraction procedures were the same as described for plasma.
HPLC analytical conditions
The Waters 2690 separation module and the Waters 2487 dual λ absorbance detector (Waters, Milford, MA, USA) were used with a gradient elution. Chromatographic separations were achieved with a Phenomenex Luna C18 analytical column (4.6 × 250 mm, 5 μm) and a SecurityGuard C18 cartridge (3 × 4 mm) (Phenomenex, Torrance, CA, USA). The mobile phase A was acetonitrile, and the mobile phase B was 0.1% triethylamine in distilled water with pH adjusted to 3.0 by addition of phosphoric acid. A gradient elution was applied by increasing the mobile phase A from 54 to 80% directly at 8.5 min through 12 min and then slowly decreasing to 54% during 12–15 min. The flow rate was 1.2 ml/min and the oven temperature was 40°C. The UV detection wavelength was set at 227 nm.
Assay validation
The calibration curves were constructed by the weighted regression method (1/x) by plotting the peak area ratios of drug to internal standard vs. actual concentration. The lower limit of quantification (LLOQ) was defined as the lowest drug concentration that yielded a signal-to-noise (S/N) ratio >10, with acceptable accuracy and precision. The precision was expressed as the coefficient of variance of each concentration, and the accuracy was expressed as the percentage of mean calculated vs. actual concentrations. For plasma, the intra- and inter-day assay variability was determined by assaying LLOQ (10 ng/ml), low quality control (QC) (40 ng/ml), medium QC (2,000 ng/ml) and high QC (9,000 ng/ml) samples on 3 consecutive days with 3 replicate samples of each day. For tissues, the intra- and inter-day assay variability was determined by assaying LLOQ (10 ng/ml for stomach, large intestine, kidney, spleen and ovary, 20 ng/ml for liver, and 50 ng/ml for small intestine and lung), low QC (90 ng/ml), medium QC (2,000 ng/ml) and high QC (9,000 ng/ml) samples on 3 consecutive days with 3 replicate samples of each day.
Data analysis
The plasma drug concentration vs. time data were subjected to a non-compartmental analysis using the nonlinear least-squares regression program WinNonlin (Pharsight, Cary, NC, USA). The area under the plasma drug concentration vs. time curve (AUC) and the area under the first moment curve (AUMC) were calculated using the trapezoidal rule extrapolated to infinite time. The extrapolation of AUC and AUMC to infinite time was obtained by adding C n/λ z to AUC and \( t_{\text{n}} C_{\text{n}} /\lambda_{\text{z}} + C_{\text{n}} /\lambda_{\text{z}}^{2} \) to AUMC, where C n is the concentration of the last sampling time (t n). The terminal elimination half-life \( (t_{{1/2,\lambda_{\text{z}} }} ) \) was calculated as 0.693/λ z. The t max was the time to reach the maximum drug concentration (C max). The apparent oral systemic clearance (Cls/F), volume of distribution (V d/F) and mean residence time (MRT) were calculated as Dose/AUC, Dose.AUMC/AUC2 and AUMC/AUC, respectively. The absolute bioavailability was calculated as DoseTaxol .AUCDHP 107/DoseDHP 107 .AUCTaxol. Similarly, tissue distribution ratios were calculated using the AUC values determined for each tissue. All data were expressed as the mean ± SD.
Results
In this study, validated HPLC assays were utilized to determine paclitaxel concentrations in plasma and various tissue samples. The chromatographic retention times were 7.8 and 6.4 min for paclitaxel and the internal standard, respectively. A linearity was achieved over a concentration range from 10 to 10,000 ng/ml for plasma, stomach, large intestine, kidney, spleen and ovary, 20–10,000 ng/ml for liver, and 50–10,000 ng/ml for small intestine and lung (r 2 ≥ 0.989). The intra- and inter-day accuracy ranged from 80.9 to 120.0% and 82.0–116.0%, respectively, with their respective %CV being ≥18.2% and ≤18.7% for plasma and all tissues. The LLOQ was 10 ng/ml for plasma, stomach, large intestine, kidney, spleen and ovary, 20 ng/ml for liver, and 50 ng/ml for small intestine and lung.
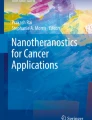
Figure 1 shows the plasma paclitaxel concentration-time profiles obtained after i.v. injection of 5, 10 and 20 mg/kg doses of Taxol and oral administration of 10, 20 and 40 mg/kg doses of DHP 107. Upon i.v. injection, plasma drug concentrations decreased mono-exponentially. After oral administration, a distinct absorption phase was observed followed by a mono-exponential decay in plasma drug concentrations. There was a tendency of a greater inter-animal variability in measured drug concentrations after oral administration (Fig. 1). Table 1 summarizes the plasma pharmacokinetic parameters obtained after i.v. and oral drug administration. Following i.v. injection, there were reductions in Cls (1.5 → 0.2 l/h/kg) and V z (4.1 → 0.5 l/kg) as the dose was increased from 5 to 20 mg/kg. The initial plasma concentration (C 0) and the area under the curve (AUC) were non-proportionally increased as the dose was increased (Table 1). The terminal elimination half-life, however, remained unaltered (range 1.1–1.9 h) as a result of simultaneous reductions in Cls and Vz. Following oral administration, the maximum concentration (C max) was achieved over 1–2 h. As with i.v. injection, the apparent clearance (Cls/F) and volume (V z/F) were reduced, and C max and AUC were nonlinearly increased with increasing the dose. The terminal elimination half-life (1.5–2.1 h) was comparable to that found after i.v. injection. Values for the absolute oral bioavailability of DHP 107 determined at various doses are shown in Table 2. When plasma AUCDHP 107 was compared with AUCTaxol at an i.v. dose of 5 mg/kg, the highest bioavailability (29.0%) was observed with the 40 mg/kg oral dose and decreased to 14.6 and 11.9% as the oral dose was reduced to 20 and 10 mg/kg. Similarly, when AUCDHP 107 was compared with AUCTaxol at higher i.v. doses of 10 or 20 mg/kg, the absolute bioavailability was decreased as the oral dose was reduced (Table 2).

Average plasma concentration-time profiles of paclitaxel after i.v. injection of 5 (open circle), 10 (open square) and 20 (open triangle) mg/kg doses of Taxol and oral administration of 10 (filled circle), 20 (filled square) and 40 (filled triangle) mg/kg doses of DHP 107 in mice (n = 4 per sampling time)
Figure 2 shows the drug concentration-time profiles for individual tissues following oral administration of DHP 107 and i.v. injection of Taxol at different doses. The C max, t max and AUC values determined for each tissue are summarized in Table 3. Upon i.v. injection, paclitaxel was rapidly distributed to all tissues, with maximum drug concentrations observed at the first sampling time (0.5 h). The AUC values for these tissues were at least comparable or greater than corresponding plasma AUC values. Of all tissues tested, the liver showed the highest C max and AUC. Following oral administration of DHP 107, t max was achieved at 1–2 h in liver, kidney, spleen, lung and ovary, but was generally reached at later times in the gastrointestinal tissues. There was a preferential drug distribution to the gastrointestinal tissues as well as the liver (Table 3). Table 4 shows the extent of relative drug distribution to individual tissues calculated as the dose-normalized AUCDHP 107/AUCTaxol ratio. The range for the relative tissue distribution ratio was highest for the stomach (63.2–342.0%) followed by small intestine (74.7–139.0%), large intestine (23.4–112.9%) and ovary (3.6–108.2%). These relative tissue distribution ratios were greater than the systemic bioavailability of DHP 107 (range 1.6–29.0%). The relative tissue distribution ratios were less for liver (27.3–42.4%), kidney (15.8–28.5%), spleen (11.9–21.0%) and lung (8.5–26.6%).

Average tissue concentration-time profiles of paclitaxel after i.v. injection of 5 (open circle), 10 (open square) and 20 (open triangle) mg/kg doses of Taxol and oral administration of 10 (filled cirlce), 20 (filled square) and 40 (filled triangle) mg/kg doses of DHP 107 in mice (n = 4 per sampling time)
Discussion
DHP 107 is a lipid-based oral dosage form containing paclitaxel (10 mg/ml) formulated in a mixture of monoolein, tricarprylin and Tween 80 (1:0.5:0.3, v/v). Being a semisolid wax (m.p. 33–35°C), this oral paclitaxel dosage form needs to be warmed to body temperature prior to administration. When given orally to mice, DHP 107 is reduced to micronized particles (>5 μm) and micelles in the jejunum and a lipid absorption is found in the cytosols of enterocytes [23]. This formulation is free of Cremophor EL and does not require premedications to alleviate adverse hypersensitivity reactions associated with this solvent [6, 8] or concomitant administration of P-glycoprotein inhibitors often needed to enhance the systemic absorption of paclitaxel [24–26].
In this study, the absolute bioavailability was determined for DHP 107 after oral administration at 10, 20 and 40 mg/kg doses. For comparison purposes, Taxol was intravenously injected at 5, 10 and 20 mg/kg doses. The oral bioavailability calculated at the same i.v. and oral doses was 3.5 and 2.0% at 10 and 20 mg/kg doses, respectively. As with previous findings [7, 27], Taxol exhibited dose-dependent plasma pharmacokinetics as evidenced by altered Cls and V z and non-proportional increases in C 0 and AUC as a function of dose (range 5–20 mg/kg) (Table 1). The dose-dependent pharmacokinetics could not be explained by the presence of Cremophor EL only because its content was fixed constant for all i.v. doses. It may be possible that the dose-dependent pharmacokinetics is caused by saturable first-pass metabolism or P-glycoprotein-mediated efflux system [14, 28]. The oral administration of DHP 107 (doses range 10–40 mg/kg) also resulted in nonlinear increases in plasma C max and AUC, although this was not evident up to an oral dose of 20 mg/kg (Table 1). This observation may be explained by the low oral bioavailability, i.e., the plasma AUCDHP at doses up to 20 mg/kg doses (<2,008μg h/l) were less than that the plasma AUCTaxol found at a 5 mg/kg dose (3,438 μg h/l). Given the dose-nonlinear pharmacokinetic nature of paclitaxel, it may be more appropriate to calculate the oral bioavailability of DHP 107 at comparable AUC values between i.v. and oral administration. Consequently, the dose-normalized plasma AUCDHP 107/AUCTaxol ratios determined between 5 mg/kg i.v. dose and 20 or 40 mg/kg oral dose may more appropriately represent the absolute bioavailability of DHP 107 (14.6–29.0%). Ho et al. [29] reported that the absolute oral bioavailability of paclitaxel was higher (7.8 vs. 2.5%) in mice when it was given in a dosing vehicle consisting of D-α-tocopheryl polyethylene glycol 400 succinate (TPGS 400) and ethanol (1:1 v/v) than in the Taxol formulation (Cremophor EL: ethanol, 1:1 v/v) given orally. It is interesting to note that AUC found for the Cremophor EL-free, TPGS 400 formulation given at a paclitaxel dose of 100 mg/kg (499 ± 42 min μg/ml) is comparable to AUC found for the oral DPH 107 at a paclitaxel dose of 40 mg/kg (7,793 μg h/l, Table 1) in the present study. A caution should be, however, exercised when comparing these AUC values due to the dose-dependent nature of paclitaxel pharmacokinetics.
After i.v. injection of Taxol, AUC values for all tissues were higher than corresponding plasma AUC values (Tables 1 and 3), with the highest AUC observed for the liver. The distribution of paclitaxel was comparable among other tissues (Table 3). It is worth noting that, unlike the dose-nonlinear plasma pharmacokinetics, AUC values for individual tissues were linearly increased with increasing the i.v. dose. As with the i.v. injection study, following oral administration of DHP 107, AUC values for all tissues were higher than corresponding plasma AUC values (Tables 1 and 3). In addition, there was a preferential drug distribution to the gastrointestinal tissues of stomach, small intestine and large intestine (Tables 3 and 4). Since DHP 107 is a lipid-based oral dosage form, it may be possible that micronized particles and micelles may still be adhered to the gut luminal surface after rinsing the tissues (3 cycles), resulting in overestimation in the gastrointestinal tissue distribution. To examine this possibility, the rinsing efficiency was determined in a separate study. Four mice were administered with DHP 107 at a dose of 40 mg/kg, and stomach, small intestine and large intestine were taken at 2 h. Each tissue was cut longitudinally into two parts, and one part washed 3 times and the other part washed 10 times with saline. The average drug concentrations measured in these tissues were comparable to those found earlier. In addition, there was no statistical difference in drug concentrations between 3 and 10 washing cycles. Therefore, the preferential drug distribution to the gastrointestinal tissues found after oral administration of DHP 107 appears to be a result of drug transport across the gastrointestinal membranes [23]. The extent of tissue distribution of DHP 107 was compared with Taxol. At a fixed i.v. dose of 5, 10 or 20 mg/kg, the relative tissue AUCDHP 107/AUCTaxol ratios did not increase with increasing the oral dose for all tissues but stomach. Similarly, at a fixed oral dose of 10, 20 or 40 mg/kg, the relative tissue AUCDHP 107/AUCTaxol ratios appear unaltered for all tissues with increasing the i.v. dose (Table 4). It is worth noting that, compared with the absolute bioavailability (range 1.6–29.0%), the relative tissue distribution ratios of DHP 107 were greater for stomach (63.2–342.9%), small intestine (74.7–139.0%), large intestine (23.4–112.9%) and ovary (3.6–108.2%). The relative tissue distribution ratios appear similar or greater for other tissues of liver (27.3–42.4%), kidney (15.8–28.5%), spleen (11.9–21.0%) and lung (8.5–26.6%).
In conclusion, paclitaxel was systemically absorbed after oral administration of DHP 107, with the absolute bioavailability determined at comparable oral and i.v. AUC values being 14.6–29.0%. Furthermore, the relative tissue distribution of DHP 107 calculated as the dose-normalized tissue AUCDHP 107/AUCTaxol ratio was greater than the plasma AUCDHP 107/AUCTaxol ratios (systemic bioavailability), especially for the gastrointestinal tissues and ovary. Further clinical studies are warranted to examine the therapeutic implications of orally administering DHP 107 to cancer patients.
References
Holmes FA, Walters RS, Theriault RL, Forman AD, Newton LK, Raber MN, Buzdar AU, Frye DK, Hortobagyi GN (1991) Phase II trial of Taxol, an active drug in the treatment of metastatic breast cancer. J Natl Cancer Inst 83:1797–1805
Murphy WK, Fossella FV, Winn RJ, Shin DM, Hynes HE, Gross HM, Davilla E, Leimert J, Dhingra H, Raber MN (1993) Phase II study of Taxol in patients with untreated advanced non-small-cell lung cancer. J Natl Cancer Inst 85:384–388
Schiff PB, Horwitz SB (1980) Taxol stabilizes microtubules in mouse fibroblast cells. Proc Natl Acad Sci USA 77:1561–1565
Rowinsky EK, Cazenave LA, Donehower RC (1990) Taxol: a novel investigational antimicrotubule agent. J Natl Cancer Inst 82:1247–1259
Mekhail TM, Markman M (2002) Paclitaxel in cancer therapy. Expert Opin Pharmacother 3:755–766
Weiss RB, Donehower RC, Wiernik PH, Ohnuma T, Gralla RJ, Trump DL, Baker JR Jr, Van Echo DA, Von Hoff DD, Leyland-Jones B (1990) Hypersensitivity reactions from Taxol. J Clin Oncol 8:1263–1268
Sparreboom A, van Tellingen O, Nooijen WJ, Beijnen JH (1996) Nonlinear pharmacokinetics of paclitaxel in mice results from the pharmaceutical vehicle Cremophor EL. Cancer Res 56:2112–2115
Gelderblom H, Verweij J, Nooter K, Sparreboom A (2001) Cremophor EL: the drawbacks and advantages of vehicle selection for drug formulation. Eur J Cancer 37:1590–1598
Kim TY, Kim DW, Chung JY, Shin SG, Kim SC, Heo DS, Kim NK, Bang YJ (2004) Phase I and pharmacokinetic study of Genexol-PM, a Cremophor-free, polymeric micelle-formulated paclitaxel, in patients with advanced malignancies. Clin Cancer Res 10:3708–3716
Sparreboom A, Scripture CD, Trieu V, Williams PJ, De T, Yang A, Beals B, Figg WD, Hawkins M, Desai N (2005) Comparative preclinical and clinical pharmacokinetics of a Cremophor-free, nanoparticle albumin-bound paclitaxel (ABI-007) and paclitaxel formulated in Cremophor (Taxol). Clin Cancer Res 11:4136–4143
Kim DW, Kim SY, Kim HK, Kim SW, Shin SW, Kim JS, Park K, Lee MY, Heo DS (2007) Multicenter phase II trial of Genexol-PM, a novel Cremophor-free, polymeric micelle formulation of paclitaxel, with cisplatin in patients with advanced non-small-cell lung cancer. Ann Oncol 18:2009–2014
Eiseman JL, Eddington ND, Leslie J, MacAuley C, Sentz DL, Zuhowski M, Kujawa JM, Young D, Egorin MJ (1994) Plasma pharmacokinetics and tissue distribution of paclitaxel in CD2F1 mice. Cancer Chemother Pharmacol 34:465–471
Wacher VJ, Salphati L, Benet LZ (2001) Active secretion and enterocytic drug metabolism barriers to drug absorption. Adv Drug Deliv Rev 46:89–102
Sparreboom A, van Asperen J, Mayer U, Schinkel AH, Smit JW, Meijer DK, Borst P, Nooijen WJ, Beijnen JH, van Tellingen O (1997) Limited oral bioavailability and active epithelial excretion of paclitaxel (Taxol) caused by P-glycoprotein in the intestine. Proc Natl Acad Sci USA 94:2031–2035
Gao P, Rush BD, Pfund WP, Huang T, Bauer JM, Morozowich W, Kuo MS, Hageman MJ (2003) Development of a supersaturable SEDDS (S-SEDDS) formulation of paclitaxel with improved oral bioavailability. J Pharm Sci 92:2386–2398
Woo JS, Lee CH, Shim CK, Hwang SJ (2003) Enhanced oral bioavailability of paclitaxel by coadministration of the P-glycoprotein inhibitor KR30031. Pharm Res 20:24–30
Yang S, Gursoy RN, Lambert G, Benita S (2004) Enhanced oral absorption of paclitaxel in a novel self-microemulsifying drug delivery system with or without concomitant use of P-glycoprotein inhibitors. Pharm Res 21:261–270
Tiwari SB, Amiji MM (2006) Improved oral delivery of paclitaxel following administration in nanoemulsion formulations. J Nanosci Nanotechnol 6:3215–3221
Khandavilli S, Panchagnula R (2007) Nanoemulsions as versatile formulations for paclitaxel delivery: peroral and dermal delivery studies in rats. J Invest Dermatol 127:154–162
Peltier S, Oger JM, Lagarce F, Couet W, Benoît JP (2006) Enhanced oral paclitaxel bioavailability after administration of paclitaxel-loaded lipid nanocapsules. Pharm Res 23:1243–1250
Zhang X, Burt HM, Von Hoff D, Dexter D, Mangold G, Degen D, Oktaba AM, Hunter WL (1997) An investigation of the antitumour activity and biodistribution of polymeric micellar paclitaxel. Cancer Chemother Pharmacol 40:81–86
Zhang C, Qu G, Sun Y, Wu X, Yao Z, Guo Q, Ding Q, Yuan S, Shen Z, Ping Q, Zhou H (2008) Pharmacokinetics, biodistribution, efficacy and safety of N-octyl-O-sulfate chitosan micelles loaded with paclitaxel. Biomaterials 29:1233–1241
Hong JW, Lee IH, Kwak YH, Park YT, Sung HC, Kwon IC, Chung H (2007) Efficacy and tissue distribution of DHP107, an oral paclitaxel formulation. Mol Cancer Ther 6:3239–3247
van Asperen J, van Tellingen O, Sparreboom A, Schinkel AH, Borst P, Nooijen WJ, Beijnen JH (1997) Enhanced oral bioavailability of paclitaxel in mice treated with the P-glycoprotein blocker SDZ PSC 833. Br J Cancer 76:1181–1183
Bardelmeijer HA, Ouwehand M, Beijnen JH, Schellens JH, van Tellingen O (2004) Efficacy of novel P-glycoprotein inhibitors to increase the oral uptake of paclitaxel in mice. Invest New Drugs 22:219–229
Varma MV, Panchagnula R (2005) Enhanced oral paclitaxel absorption with vitamin E-TPGS: effect on solubility and permeability in vitro, in situ and in vivo. Eur J Pharm Sci 25:445–453
Gianni L, Kearns CM, Giani A, Capri G, Viganó L, Lacatelli A, Bonadonna G, Egorin MJ (1995) Nonlinear pharmacokinetics and metabolism of paclitaxel and its pharmacokinetic/pharmacodynamic relationships in humans. J Clin Oncol 13:180–190
Gallo JM, Li S, Guo P, Reed K, Ma J (2003) The effect of P-glycoprotein on paclitaxel brain and brain tumor distribution in mice. Cancer Res 63:5114–5117
Ho PY, Yeh TK, Yao HT, Lin HL, Wu HY, Lo YK, Chang YW, Chiang TH, Wu SHW, Chao YS, Chen CT (2008) Enhanced oral bioavailability of paclitaxel by D-α-tocopheryl polyethylene glycol 400 succinate in mice. Int J Pharm 359:174–181
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s00280-009-0952-6
Rights and permissions
About this article
Cite this article
Shin, B.S., Kim, H.J., Hong, S.H. et al. Enhanced absorption and tissue distribution of paclitaxel following oral administration of DHP 107, a novel mucoadhesive lipid dosage form. Cancer Chemother Pharmacol 64, 87–94 (2009). https://doi.org/10.1007/s00280-008-0849-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-008-0849-9