
Abstract
The non linear relationship between calcitriol (1,25-D3) dose and AUC in cancer patients suggests that the commercially available caplet 1,25-D3 formulation (Rocaltrol) cannot achieve the high systemic exposure associated with antitumor activity in animal models. The primary objective of this analysis was to determine whether a liquid 1,25-D3 formulation had a more favorable pharmacokinetic profile. This analysis was based on the results obtained in 2 phase I clinical studies seeking to determine the maximum tolerated dose of 1,25-D3 administered in combination with either dexamethasone or paclitaxel daily for three consecutive days weekly. Data were available for 12 patients treated with the caplet formulation at doses ranging from 12 μg to 21 μg, and for 16 patients treated with the liquid formulation at doses ranging from 13 μg to 36 μg; data for 19 patients were available at doses for which both formulations were used. There were no differences in Cmax and AUC0–24h between the two formulations (P>0.17) As was noted with the caplet formulation, dose-related proportional increases in Cmax and AUC0–24h were not observed with liquid 1,25-D3 at doses ≥ 13 μg (P>0.83). We conclude that the commercially available liquid 1,25-D3 formulation offers no PK advantage over caplet formulation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Calcitriol, 1,25-dihydroxycholecalciferol (1,25-D3), a secosteroid hormone, has potent antiproliferative, differentiating and apoptotic effects in vitro [1–5], and antitumor activity against murine squamous cell carcinoma (SCC), Dunning rat metastatic prostate adenocarcinoma (MLL) and xenografts of human prostate and colorectal carcinomas in immune compromised mice [5–8]. Molecular mechanisms of 1,25-D3 antitumor activity are not fully understood. However, 1,25-D3 induces G0/G1 arrest mediated by cyclin-dependent kinase p27kipi and p21waf1/cipI [8–10], inhibits MEK- and Akt-mediated survival signaling pathways and up-regulates pro-apoptotic signaling pathways [11–14].
In preclinical models, high 1,25-D3 doses are required to elicit antitumor activity. Continuous daily administration of these doses causes dose-limiting hypercalcemia in preclinical models and humans. However, in our models which utilize an intermittent dosing schedule of 1,25-D3, hypercalcemia is not dose-limiting [15]. Our preclinical studies have also demonstrated that dexamethasone (DEX) administration decreases 1,25-D3-induced hypercalcemia and enhances 1,25-D3 antitumor activity. We have shown that the biochemical mechanisms by which DEX modulates 1,25-D3 include DEX-mediated up-regulation of vitamin D3 nuclear receptors (VDR) in tumor tissue and the down-regulation of VDR ligand binding in intestinal mucosa [15].
The most often prescribed commercially available oral preparation of 1,25-D3 is a caplet formulation (0.5 μg/caplet, Rocaltrol, Hoffmann-La Roche Ltd). Previous studies using this 1,25-D3 formulation in cancer patients revealed no limiting hypercalcemia at doses as high as 38 μg QDx3 weekly and 2.8 μg/kg QDx1 weekly. The studies showed substantial inter-patient variability in serum 1,25-D3 Cmax and AUC and a non-linear relationship between 1,25-D3 dose and AUC [16–18]. Although the mechanism underlying this nonlinear relationship remains to be established, we speculated that decreased oral bioavailability of 1,25-D3 at high doses might result from unfavorable pharmaceutical conditions in the intestine associated with the ingestion of the large number of 1,25-D3 caplets required to achieve high doses. We hypothesized that the bioavailability of oral 1,25-D3 might be improved by using a liquid formulation 1,25-D3. In this study, we investigated the serum PK of high dose caplet and liquid 1,25-D3 formulations.
Materials and methods
Study population
Patients in this analysis were enrolled in one of the two phase I studies in which the dose of 1,25-D3 was escalated: study A was a study of 1,25-D3 + paclitaxel in patients with advanced solid tumors; study B was a study of 1,25-D3±DEX in patients with androgen independent prostate cancer (AIPC). Patients were eligible for the studies if no standard therapy was available and if they had adequate bone marrow, kidney and liver function, as evidenced by WBC ≥4,000/ μl, platelets ≥100,000/μl, serum creatinine ≤1.5 mg/dl, bilirubin ≤ 2 mg/dl and SGOT ≤ 75 mIU. Patients were required to have albumin-corrected serum calcium ≤10.5 mg/dl and no past medical history of renal stones. This protocol was approved by the Biomedical Institutional Review Board of the University of Pittsburgh, and all patients signed the written informed consent before participation.
Drug administration
Two oral 1,25-D3 formulations were studied: a soft gel caplet (0.5 μg/caplet, Rocaltrol) and the liquid (Rocaltrol, 1.0 μg/ml); both were kindly provided by Hoffman-Roche. Liquid Rocaltrol solution, which contains butylated hydroxyanisole, butylated hydroxytoluene and medium chain triglycerides, is commercially available as a clear, colorless to slightly yellowish oily liquid.
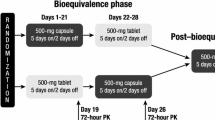
During the conduct of these two studies, the loss of a linear relationship between dose and serum 1,25-D3AUC was recognized. Consequently re-escalation of 1,25-D3 in liquid form was pursued to determine whether the liquid formulation provided better systemic exposure. This analysis compares the PK of the liquid and caplet 1,25-D3 formulations at similar doses. Table 1 displays the doses of formulations studied. The drug administration schedule for study A was 1,25-D3 QDx3 (day l–3) + paclitaxel 80 mg/m2 on day 3; that for study B was 1,25-D3 alone QDx3 (days 1–3) on week 1, and in subsequent weeks, 1,25-D3 QDx3 (days 1–3) and dexamethasone QDx4 (days 0–3). In both studies, oral ingestion of both caplet and liquid 1,25-D3 formulations was supervised by the nursing staff of General Clinical Research Center (GCRC). At least three patients were treated at each dose level, and no intra-patient calcitriol dose escalation was allowed. Treatment was continued until disease progression or occurence of dose-limiting toxicity. Serum calcium, phosphorus, creatinine, BUN, albumin and glucose were determined weekly.
Pharmacokinetic blood sampling
In study A, PK blood samples for 1,25-D3 PK were collected on day 1. In study B, blood samples were collected on day 3 and/or on day 17. In both studies, samples were obtained before and 0.5, 1, 2, 3, 4, 6, 8, 10, 12, 16, 18, 20, 22, and 24 h after the dose of 1,25-D3. Blood samples for PK studies were collected, processed and assayed for 1,25-D3 concentrations using 1,25-dihydroxyvitamin D3- [I125] RIA kits as previously described [17].
Dose-limiting toxicity
Dose-limiting hypercalcemia was defined as symptoms of hypercalcemia at any serum calcium level >11 mg/dl or two consecutive calcium levels ≥12 mg/dl, even if the patient was asymptomatic. All serum calcium levels used for the determination of toxicity were corrected for serum albumin using the formula: Ca2+corrected=Ca2+measured + (0.8) (3.2 − albumin). Serum albumin was measured in mg/dl. Dose-limiting toxicity other than hypercalcemia was defined as any grade 3 or greater non-hematological toxicity. Dose-limiting toxicity associated with short-term use of dexamethasone is primarily hyperglycemia.
Pharmacokinetic data analysis
Serum 1,25-D3 Cmax and time to Cmax (Tmax) were determined by visual inspection of the plots of serum calcitriol concentrations versus time. Serum 1,25-D3 AUC0–24h was calculated using the trapezoidal rule without subtraction of baseline 1,25-D3 concentrations. All pharmacokinetic parameters were calculated using a PHARM/PCS computer program [19]. Statistical tests used to analyse the data are identified in the appropriate results section.
Results
Effect of prior 1,25-D3 treatment on subsequent pre-dosing serum 1,25-D3concentrations
The mean day 1 pretreatment serum concentration of 1,25-D3 was 38.4±21.5 pg/ml for cancer patients enrolled in these trials. In study B, the pretreatment means on days 3 and 17 were 223.6±106.6 and 103±39.3 pg/ml, respectively, indicating substantial carry-over of 1,25-D3from administration during the previous 2 days.
Relationship between liquid 1,25-D3dose and AUC
For the liquid formulation, there was much inter-patient variability in serum 1,25-D3 concentrations; Fig. 1 illustrates this with concentration-time profiles for the six patients treated at the two highest dose levels of liquid 1,25-D3 formulation. Figure 2 shows the difference between day 3 and day 17 AUC for the 6 patients receiving caplet 1,25-D3 at 12 and 16 μg doses; the difference is not significant (p=0.44, Wilcoxon signed-ranks test). Figure 2 also indicates that the difference in the 2 sampling periods (day 3 and 17) is small compared to the observed inter-patient variability). Plots of Cmax and AUC against dose for all patients receiving liquid 1,25-D3 show no increase in exposure with increased dose (Fig. 3). The P-value for the null hypothesis that there is no dose-response effect is 0.96 for Cmax and 0.83 for AUC (Jonckheere-Terpstra test).

Individual patient serum 1,25-D3 concentration versus time curves after 28 μg (solid circles) and 36 μg (open squares) of liquid 1,25-D3 administration showing substantial inter-patient variability in serum 1,25-D3 levels achieved

Day 3 (closed circles) and day 17 (open circles) serum AUC results for 6 patients receiving 12 (pt#1–3) and 16 μg (pt#4–6) doses of caplet 1,25-D3formulation. The difference between day 3 and 17 is not significant

Scatter plots of serum 1,25-D3 Cmax (a) and AUC0–24h (b) against liquid 1,25-D3 dose, with regression lines superimposed. Trends suggesting progressive decreases in both PK parameters are not significant. Symbols used to indicate the timing of PK study: open triangle=day 1, closed circles=day 3, and open circles=day 17
Liquid versus caplet 1,25-D 3 formulation serum PK
There was no difference in the observed Cmax and calculated AUC between the liquid and caplet formulated 1,25-D3 administered at the same dose. There are data for both formulations at doses of 13, 16 and 21 μg; (Fig. 4). The P-values for no difference between liquid and caplet are 0.71 for Cmax and 0.17 for AUC (Wilcoxon test, stratified by dose). If the systematic difference in AUC between the liquid and capsule formulations exceeded the inter-patient standard deviation at a fixed dose, there would be roughly 80% power to observe a P-value of 0.1, or less. Thus, the observed P-values suggest that the difference between the two formulations is less than the inter-patient standard deviation.

Scatter plots of serum 1,25-D3 Cmax (a) and AUC0–24h (b) for caplet (closed circles) and liquid (open circles) 1,25-D3formulations at the 13, 16 and 21 μg dose levels. There are no significant differences in these PK parameters
Adverse events associated with liquid 1,25-D3formulation
Transient diarrhea was experienced by all patients within 12 h of receiving liquid 1,25-D3 formulation; oral ingestion of caplet 1,25-D3has not been associated with diarrhea. As was previously noted with the caplet formulation, grade 1 and 2 nausea, anorexia, vomiting, constipation, fatigue and weakness were the most frequent reported adverse effects following liquid 1,25-D3 ingestion. Hypercalcemia was not a dose-limiting toxicity.
Discussion
We have previously suggested that bioavailability, a pharmacokinetic issue, and not hypercalcemia may compromise the clinical utility of high-dose 1,25-D3 as an antitumor agent [16]. We suggested that decreased oral bioavailability of 1,25-D3 at high doses could result from unfavorable pharmaceutical conditions in the intestine associated with the ingestion of the large number of caplets required to deliver high doses of 1,25-D3. We speculated that the administration of liquid 1,25-D3 formulation could overcome the bioavailability issue. Although the sample size is small, the results of this study clearly indicate that liquid 1,25-D3 formulation will not reliably achieve serum 1,25-D3 Cmax and AUC values associated with antitumor activity in animal tumor models [20]. These results further demonstrate that the commercially available liquid 1,25-D3 formulation offered no advantage in bioavailability or PK over the caplet formulation. In addition, the ingestion of large volumes (16–38 ml) of oily liquid 1,25-D3 formulation at one time has the disadvantage of causing transient episodes of diarrhea. These results point to the need for new approaches to solve 1,25-D3 bioavailability problems. Although intravenous administration of 1,25-D3 is the most direct approach to resolving the bioavailability issue, an alternative approach is to develop new oral 1,25-D3 formulations. The early results of the ongoing pharmacokinetics and bioavailability studies in cancer patients using DN101, a new 1,25-D3 caplet formulation, are encouraging [21].
In addition to confirming the previous observation that hypercalcemia is not dose-limiting when 1,25-D3 is administered on QDx3 weekly intermittent schedule, our present results demonstrate significant serum 1,25-D3 carry-over to the third day from administration on the previous 2 days on the QDx3 schedule; this suggests a potential for achieving higher 1,25-D3 systemic exposure on the QDx3 than on the QDx1 weekly schedule. However, therapeutic efficacy of both QDx1 and QDx3 weekly administration of 1,25-D3 in combination with docetaxel or dexamethasone has been documented in patients with androgen independent prostate cancer [22, 23].
In summary, our results show that the clinical use of liquid formulation to deliver high doses of 1,25-D3 is associated with transient episode diarrhea and offers no pharmacokinetic or bioavailability advantage over use of the caplet formulation. We confirm our previous results that hypercalcemia is not the dose-limiting toxicity on a QDx3 weekly intermittent 1,25-D3 treatment schedule.
References
Colston K, Colston MJ, Feldman D (1981) 1,25-dihydroxyvitamin D3 and malignant melanoma: the presence of receptors and inhibition of cell growth in culture. Endocrinol 108:1083–1086
Chouvet C, Vicard E, Devonec M, Saez S (1986) 1,25-dihydroxyvitamin D3inhibitory effect on the growth of two human breast cancer cell lines (MCF-7, BT-20). J Steroid Biochem 24:373–376
Cross HS, Pavelka M, Slavik J, Peterlik M (1992) Growth control of human colon cancer cells by vitamin D and calcium in vitro. J Natl Cancer Inst 84:1355–1357
Peehl DM, Skowronski RJ, Leung GK, Wong ST, Stamey TA, Feldman D (1994) Antiproliferative effects of 1,25-dihydroxyvitamin D3 on primary cultures of human prostatic cells. Cancer Res 54:805–810
McElwain MC, Dettelbach MA, Modzelewski RA, Russell DM, Uskokovic MR, Smith DC et al (1995) Anti-proliferative effects in vitro and in vivo of 1,25-dihydroxyvitamin D3 and vitamin D3 analogue in a squamous cell carcinoma model system. Mol Cell Differ 3:31–50
Eisman JA, Barkla DH, Tutton PJM (1987) Suppression of in vivo growth of human cancer solid tumor xenografts by 1,25-dihydroxyvitamin D3. Cancer Res 47:21– 25
Getzenberg RH, Light BW, Lapco PE, Konety BR, Nangia AK, Acierno JS Jr et al (1997) Vitamin D inhibition of prostate adenocarcinoma growth and metastasis in the Dunning rat prostate model system. Urol 50:999–1006
Hershberger PA, Modzelewski RA, Shurin ZR, Rueger RM, Trump DL, Johnson CS (1999) 1,25-dihydroxycholecalciferal (1,25-D3) inhibits the growth of squamous cell carcinoma and down-modulates p21 (waf1/Cip1) in vitro and in vivo, Cancer Res 59:2644–2649
Lui M, Lee M, Cohen M, Bommakanti M, Freedman LP (1996) Transcriptional activation of the CDK inhibitor, p21 by vitamin D3 leads to induced differentiation of myelomonocytic cell line U937. Gene Dev 10:142–153
Wang QM, Jones JB, Studzinski GP (1996) Cyclin–dependent kinase inhibitor p27, as a mediator of G1-S phase block induced by 1,25-dihydroxyvitamin D3 in HL60 cells. Cancer Res 56:264–267
McGuire TF, Trump DL, Johnson CS (2001) Vitamin D3-induced apoptosis of murine squamous cell carcinoma cells: Selective induction of caspase-dependent MEK cleavage and up-regulation of MEKK-1. J Biol Chem 276:26365–26373
Bernardi RJ, Trump DL, Yu WD, McGuire TF, Hershberger PA, Johnson CS (2001) Combination of 1α,25-dihydroxyvitamin D3 with dexamethasone enhances cell cycle arrest and apoptosis: Role of nuclear receptor cross-talk and Erk/Akt signaling. Clin Cancer Res 7:4164–4173
Hershberger PA, McGuire TF, Yu WD, Zuhowski EG, Schellens JH, Egorin MJ et al (2002) Cisplatin potentiates 1,25-dihydroxyvitamin D3-induced apoptosis in association with increased mitogen-activated protein kinase kinase kinase 1 (MEKK-1) expression. Mol Cancer Ther 10:821– 829
Wang X, Studzinski GP (2001) Activation of extracellular signal-regulated kinases (ERKs) defines the first phase of 1,25-dihydroxyvitamin D3-induced differentiation of HL60 cells. J Cell Biochem 80:471– 82
Yu WD, McElwain MC, Modzelewski RA, Russell DM, Smith DC, Trump DL et al (1998) Enhancement of 1,25-dihydroxyvitamin D3-untreated antitumor activity with dexamethasone. J Natl Cancer Inst 90:134–141
Muindi JR, Peng Y, Potter DM, Hershberger PA, Tauch JS, Capozzoli MJ et al (2002) Pharmacokinetics of high dose calcitriol: results obtained during a phase one trial of calcitriol and paclitaxel. Cancer Pharmacol Ther 72:648–659
Smith, DC, Johnson CS, Freeman CC, Muindi J, Wilson JW, Trump DL (1999) A phase I trial of Calcitriol (1,25-dihydroxycholecalciferal) in patients with advanced malignancy. Clin Cancer Res 5:1339–1345
Beer TM, Munar M, Henner WD (2001) A Phase I trial of pulse calcitriol in patients with refractory malignancies: pulse dosing permits substantial dose escalation. Cancer 91:2431–2439
Tallarida RJ, Murray RB (1986) Manual of pharmacologic calculation with computer programs. Springer, Berlin Heidelberg New York, pp 197–291
Muindi JR, Modezlewski RA, Peng Y, Trump DL, Johnson CS (2004) Pharmacokinetics of 1α, 25-dihydroxycholecalciferol pharmacokinetics in normal mice after systemic exposure to effective and safe antitumor doses. Oncology 66:62–66
Beer TM, Javle M, Henner WD, Trump DL (2004) Pharmacokinetics (PK) and tolerability of DN-101, a new formulation of calcitriol. Proc Am Assoc Cancer 95:404
Beer TM, Lemmon D, Lowe BA, Henner WD (2003) High-dose weekly oral calcitriol in patients with a rising PSA after prostatectomy or radiation for prostate carcinoma. Cancer 97:1217–1224
Trump DL, Serafine S, Brufsky J et al (2000) High dose calcitriol (1,25(OH)2vitamin D3) + dexamethasone in androgen independent prostate cancer (AIPC). Am Soc Clin Oncol 19:337a
Acknowledgements
Supported by Grants NCI RO1 CA 67267, CA 85142, P30 CA 47904, MO1-RR00056-40 and CaPCURE Award.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Muindi, J.R., Potter, D.M., Peng, Y. et al. Pharmacokinetics of liquid calcitriol formulation in advanced solid tumor patients: comparison with caplet formulation. Cancer Chemother Pharmacol 56, 492–496 (2005). https://doi.org/10.1007/s00280-005-1015-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00280-005-1015-2