
Abstract
Hereditary spherocytosis (HS) is the most frequently observed chronic non-immune hemolytic disorder caused by altered red cell membrane function. SPTB gene mutation is one of the most common causes of HS, but pathogenicity analyses and pathogenesis research on these mutations have not been widely conducted. In this study, a novel heterozygous mutation of the SPTB gene (c.1509_1518del; p.K503Nfs*67) was identified in a Chinese family with HS by whole-exome sequencing (WES) and was then confirmed by Sanger sequencing. Next, the pathogenicity and pathogenesis of this mutation were studied using peripheral blood. We found that this mutation disrupted the synthesis and localization of β-spectrin and weakened the interaction between β-spectrin and ankyrin, which may be caused by the nonsense-mediated mRNA degradation pathway. These changes lead to the transformation of discoid erythrocytes into spherocytes, resulting in hemolytic anemia. Therefore, we classified this novel mutation as a pathogenic mutation leading to loss-of-function of β-spectrin. It would be insightful to perform the same mutation test and to provide genetic counseling to other relatives of the proband. Our study increases the current understanding of the molecular mechanisms related to mutations in SPTB.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Hereditary spherocytosis (HS), the most frequent inherited chronic non-immune hemolytic disorder caused by altered red cell membrane function, is characterized by the presence of spherical-shaped red blood cells (RBCs) on peripheral blood smears. HS is prevalent worldwide, with a high incidence in the Northern European population (approximately 1:2000) [1,2,3], and the prevalence in China is approximately 1 in 100,000 people [4]. Individuals affected with HS exhibit variable clinical manifestations, ranging from nearly asymptomatic to transfusion-dependent or severe life-threatening anemia. Typical HS patients present anemia, splenomegaly, jaundice, and reticulocytosis [2, 3]. In most cases, HS can be diagnosed by family history, physical examination, and hematological parameter tests [3, 5]. Molecular detection is very helpful in the diagnosis of atypical HS patients [6].
The defects of RBC membrane components in HS are caused by their corresponding gene mutations. Mutations associated with HS include those in ANK1, EPB42, SLC4A1, SPTA1, and SPTB genes encoding ankyrin, protein 4.2, band 3 protein, α-spectrin, and β-spectrin, respectively [7]. These proteins are essential for maintaining the morphology of RBCs, and the absence of any of the above proteins will disrupt the vertical linkage between the phospholipid bilayer and the membrane skeleton, leading to a loss of erythrocyte membrane surface area. Discoid erythrocytes become spherocytes with decreased deformability and are easily prematurely destroyed by the spleen, consequently resulting in hemolytic anemia [1, 8, 9]. The majority (approximately 75%) of HS cases are inherited in an autosomal dominant pattern, although autosomal recessive inheritance and de novo mutation are also described in a subset of patients [9, 10]. Mutations in the ANK1 gene are the major cause of HS followed by mutations in the SPTB, SLC4A1, and SPTA1 genes [11, 12]. EPB42 gene mutations are generally found in the Japanese population [3].
The SPTB gene is located at 14q23.3 and contains 38 exons that encode β-spectrin with 2137 amino acids (GenBank accession no. NP_001342366.1). It consists of an N-terminal actin-binding domain and 17 spectrin repeats that contain a dimerization domain, parts of spectrin repeats, an ankyrin binding domain, and a tetramerization domain [13]. Spectrin is the major constituent of the membrane skeletal network and plays key roles in regulating membrane deformability and membrane mechanical stability [1]. To date, a total of 206 SPTB mutations have been reported in the Human Gene Mutation Database (HGMD, http://www.hgmd.cf.ac.uk/ac/index.php, last accessed 26 March 2021), 161 of which are associated with HS. Although mutations in SPTB are common in HS, the pathogenesis of SPTB mutations is not completely understood.
In this study, a novel mutation of SPTB was found in a Chinese family with HS and was predicted to be disease-causing. Then, we used the patient’s peripheral blood to further study the pathogenicity and pathogenesis of this mutation.
Subjects and methods
Participants and ethics statement
A Chinese nuclear family with HS was recruited for this study (Fig. 1A). After obtaining written informed consents, peripheral blood samples were obtained from 3 family members for mutation analysis. This study was formally approved by the Ethics Committee of The First Hospital of Lanzhou University. All procedures were performed by the approved guidelines.

Chinese family with HS-associated SPTB mutation. A Two-generation pedigree of the family with two affected individuals (I: 1 and II: 1). Filled symbols indicate individuals affected with HS, open symbols indicate unaffected individuals, and the black arrow indicates the proband. B Spherocytes were observed in the peripheral blood smears of two patients, which are indicated by black arrows. C Sanger sequencing revealed a novel heterozygous SPTB mutation (black arrows indicate the mutation sites) that was detected in the proband and his father (I: 1 and II: 1), whereas the wild-type SPTB allele was observed in his mother (I: 2). D RT-PCR showed that the mutant transcript of SPTB was undetected in both patients, and the wild-type transcript was reduced compared with control and I: 2
Whole-exome sequencing (WES) and mutation validation
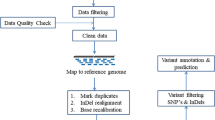
Genomic DNA of the proband was extracted from peripheral blood using the QIAamp DNA Mini Kit (Qiagen, Germany) following the manufacturer’s protocols. Whole-exome sequencing services were provided by Basecare Medical Device Co., Ltd. (Suzhou, China). Exomes were captured by an Agilent Human All Exon 60 M Kit, and the captured fragments were amplified and sequenced using an Illumina NovaSeq 6000 in 2 × 150-bp paired-end mode. The sequencing reads from WES were aligned to the human genome (NCBI Build37/hg19) with the Burrows-Wheeler Aligner (BWA) [14]. The strategies of data filtering were based on published documents [15]. WES identified a novel mutation in SPTB in the proband, which was verified using Sanger sequencing in the proband and parental DNA samples. The primers are as follows: forward 5′-CTAGCACTGGTTCTGAAGGGA G-3′, reverse 5′-CCCACCTTGATCTCATCCATCC-3′. Sanger sequencing was performed on an ABI 3730xl DNA Analyzer at Sangon Biotech, Shanghai, China.
Pathogenicity prediction
MutationTaster software was used to predict the pathogenicity of novel mutations [16]. SPTB protein structural changes caused by the mutation were predicted and analyzed by SWISS-MODEL (http://swissmodel.expasy.org) [17]. The predicted template was Protein Data Bank ID number 1sjj.1.A.
RNA extraction, RT-PCR, qPCR, western blot, immunofluorescence, and co-immunoprecipitation
A detailed description of the methods are given in Supplementary file1.
Results
Pedigree and clinical characteristics
The proband (II: 1), an 18-year-old boy, developed anemia, jaundice, and splenomegaly when he was 7 years old. At that time, blood and serum biochemical test results revealed that the number of RBCs and hemoglobin was lower than normal standards, while levels of bilirubin, RBC volume distribution width, and reticulocytes were all higher than health standards. Ultrasound showed splenomegaly. Bone marrow smear analysis showed hyperplasia with an erythroid preponderance (myeloid cells were 16%, and erythroid cell was 69%), increase of middle and late erythroblast, and spherocytes that were approximately 60%. His father (I: 1) shared similar clinical symptoms and laboratory results (Table 1), but jaundice and splenomegaly were more serious. Father’s ultrasound showed extreme splenomegaly. Notably, his father had previously been misdiagnosed with ferritin deposition (ferritin: 1966 ng/ml) in another hospital. Their RBC size showed disparity, and spherocytes were observed in the peripheral blood smear (Fig. 1B). Their red cell osmotic fragility showed elevated. No aberrant changes were identified in the direct antiglobulin test and glucose-6-phosphate dehydrogenase (G6PD) activity assay. The folic acid and vitamin B12 were within normal ranges. According to family history, clinical features, and laboratory tests, the proband and his father were diagnosed with spherocytosis in our hospital. The MCHC of both of our patients is in the normal range or even lower, which is different from most HS patients, probably due to interference from other factors such as high reticulocytes and high RBC volume distribution width. Six years later, his father underwent splenectomy due to the aggravation of anemia after cold and anemia heart disease, with a spleen size of approximately 26 cm × 18 cm × 10 cm. After splenectomy, the clinical symptoms of the father of the proband were improved.
As the proband grew older, his jaundice and splenomegaly became more and more serious and began to affect his daily life. So when he was 18 years old (after the college entrance examination), his parents took him to our hospital to ask for a splenectomy. On admission, the proband’s sclerae and skin were icteric, splenomegaly, and accompanied by easy fatigability. Because the spleen squeezed the stomach, the proband had a very poor diet, with a BMI of 16.3. The relevant laboratory results are summarized in Table 1. Then, he underwent total splenectomy under general anesthesia, with a spleen size of approximately 20 cm × 15 cm × 8 cm. The pathomorphological results support chronic congestive splenomegaly.
Characterization of a novel SPTB mutation in a family with HS
A novel heterozygous mutation in SPTB (NM_001355436.2, c.1509_1518del GGACAATATA, p.K503Nfs*67) was detected in the proband and his father (II: 1 and I: 1), while his mother had wild-type SPTB alleles (Fig. 1C). Bioinformatics prediction using MutationTaster software revealed that this mutation was disease-causing (Table 2). This frameshift mutation, located in exon 12 of the SPTB gene, resulted in a premature termination codon (PTC) within exon 13. PTC might be degraded by nonsense-mediated mRNA decay (NMD), leading to spectrin haploinsufficiency, or may skip one or more exons through nonsense-mediated altered splicing (NAS), which has the potential to rescue the function of spectrin or possible to produce an N-terminal truncated protein with an actin-binding domain, a shortened dimerization domain, and no ankyrin-binding domain as well as tetramerization domain (Supplementary file1) [18]. Compared with the tertiary structure of the wild-type protein, the truncated protein triggered the loss of the subsequent α-spiral and loop regions (Supplementary file1), which might influence the combination of β-spectrin and ankyrin. The above assumptions require further experimental verification.
RT-PCR showed no mutant SPTB transcript present
RT-PCR and subsequent cDNA sequencing revealed the presence of only wild-type SPTB transcript, and no mutant SPTB transcript was observed in the patients. This indicated that the mutant mRNA did not reach detectable levels, which was probably degraded by the NMD pathway. In addition, the wild-type mRNA products of the patients were reduced compared with unaffected members (Fig. 1D). Meanwhile, RT-PCR excluded NAS that may exist in patients.
mRNA and protein expression levels of the SPTB gene were decreased in HS patients
The mRNA expression levels of wild-type SPTB in the proband and his father were decreased by half compared with his mother and normal control (Fig. 2A). Similarly, western blot analyses revealed that the amounts of β-spectrin present in the red cell membranes of the proband and his father were approximately about 70% those in his mother and the normal control and no truncated protein was produced (Fig. 2B). Therefore, this nonsense mutation resulted in monoallelic expression of wild-type SPTB mRNA, which led to insufficient synthesis of β-spectrin on the erythrocyte membrane. This result further confirmed that the mutated mRNA might be degraded by NMD.

A qPCR revealed that this mutation reduced the mRNA expression of the SPTB gene by half. B Western blot analysis indicated that this mutation reduced the β-spectrin amount by approximately 30% and no truncated protein (65 KDa) was produced. C Co-immunoprecipitation (Co-IP) of β-spectrin and ankyrin in erythrocyte membrane proteins in the normal control and proband. Compared with the normal control, the interaction of β-spectrin with ankyrin in the proband was significantly weakened, and only approximately 70% ankyrin was captured by β-spectrin. Semi-quantitative analysis of the captured amount of ankyrin relative to the amount of immunoprecipitated β-spectrin was performed by greyscale scanning of strips
Decrease in β-spectrin located on the erythrocyte membrane in HS patients
Immunofluorescence was performed to determine the localization of β-spectrin. The results showed that the distribution of β-spectrin on most erythrocyte membrane of the proband and his father was significantly less than that of the normal control and his mother (Fig. 3), which further indicated that this mutation affected the synthesis of β-spectrin, resulting in the decrease of β-spectrin targeted to the erythrocyte membrane. Thus, the membrane skeletons of some RBCs in the patients were incomplete.

Green fluorescent signal represents β-spectrin. The β-spectrin on the erythrocyte membranes of normal people showed a circle of green fluorescence, while some erythrocytes of the patient only had a few fluorescence points, suggesting the decrease of β-spectrin targeted to erythrocyte membrane. A Normal control. B I: 1. C II: 1. D I: 2
Mutation weakens the interaction between β-spectrin and ankyrin
Some β-spectrin failed to target the erythrocyte membrane, indicating that its binding to ankyrin might be impaired. Thus, we detected the interaction between ankyrin and β-spectrin on the erythrocyte membrane by co-immunoprecipitation. The biochemical interaction between ankyrin and β-spectrin in the proband was weaker than that of the normal control (Fig. 2C). Therefore, this mutation weakens the interaction between ankyrin and β-spectrin.
Discussion
In this report, we reported a Chinese family with two members affected by HS and identified a novel mutation of SPTB in the patient by WES, which is confirmed by Sanger sequencing. This mutation leads to a premature termination codon within exon 13, resulting in a nonsense mutation (p.K503Nfs*67). Then, we performed a series of pathogenicity studies using peripheral blood to identify the pathogenesis of this novel mutation. The results indicated that this mutation disrupted the synthesis and localization of β-spectrin and weakened the interaction between β-spectrin and ankyrin, which may be caused by the nonsense-mediated mRNA degradation pathway. These changes led to the transformation of discoid erythrocytes into becoming spherocytes, resulting in hemolytic anemia.
At present, the clinical diagnosis of HS mainly relies on clinical presentation, family history, and peripheral blood smear results [3]. The eosin-5-maleimide binding test and osmotic gradient ektacytometry are also started for auxiliary diagnosis of HS [19,20,21]. However, these routine tests may be inconclusive, particularly in no family history, newborn infants, or different testing results are not consistent [6, 22]. Molecular genetic testing is an effective method to further determine the diagnosis of HS, and it can help reduce the incidence of misdiagnosis and shed new light on HS clinical management and genetic counseling of the family [6]. In our study, patient I: 1 was misdiagnosed as ferritin deposition disease in another hospital. It was not until his son came to our hospital for jaundice and fatigue at the age of 7 years that he was diagnosed with HS. Our molecular genetic testing further confirmed the diagnosis of HS, identified the genetic cause of HS, and ruled out Gilbert syndrome. Patients with combined HS and GS have been reported, but their coexistence is often underdiagnosed, which may be attributed to one condition masking another. The possibility of coexistence should be considered when serum bilirubin levels are discordant with the degree of hemolysis. Molecular genetic testing was crucial to confirm the diagnosis and to avoid underdiagnosis [23,24,25].
SPTB gene mutation is the second most common cause of HS. SPTB encodes β-spectrin protein, which is the rate-limiting protein of α2β2-tetramerization network formation and plays a key role in the formation of the erythrocyte membrane skeleton [1, 7, 8]. With the development of molecular genetic testing technology, an increasing number of SPTB mutations causing HS have been identified. Previously reported hereditary spherocytosis cases with SPTB mutations were summarized in Supplementary file1 and 2. In the dimerization domain, at least eleven mutations, p.K379Nfs*12, p.Q357*, p.Q417*, p.W437*, p.A455Qfs*24, p.T471M, p.Q442*, p.K463*, p.Q514*, p.Y474*, and p.R498Pfs*72, have been identified in HS patients, but the pathogenesis of these mutations has seldom been studied. Among the discovered SPTB mutations, about 70% are nonsense or frameshift mutations that can produce PTC, suggesting that NMD [26, 27], NAS [28], or the production of truncated protein [29] may play an important role in the pathogenesis of HS. In our study, we used the patient’s peripheral blood to further study the pathogenicity and pathogenesis of the p.K503Nfs*67 mutation. We found that this mutation resulted in a halving of mRNA expression of the SPTB gene, a reduction in β-spectrin expression of approximately 30%, no truncated protein production, and no detectable levels of mutated mRNA. Thus, we speculated that the mRNA produced by this mutation is degraded by the nonsense-mediated mRNA decay pathway, resulting in β-spectrin haploinsufficiency. Next, we found that the distribution of β-spectrin on most erythrocytes of patients was less than that of normal control, which further indicated insufficient synthesis of β-spectrin on the patient’s erythrocyte membrane. Furthermore, it was confirmed by co-immunoprecipitation that this mutation led to the weakening of the interaction between ankyrin and β-spectrin; the above evidence indicated that most of the erythrocytes in the patients could not form a complete α2β2-tetramerization network structure, which affected the reversible deformation ability of RBCs and led to the premature destruction of erythrocytes by the spleen. Therefore, it is certain that the mutation is a pathogenic mutation leading to loss-of-function of β-spectrin.
Here, we report a novel mutation in the SPTB gene in a Chinese family. We also provided powerful evidence for the pathogenicity of this mutation. It is meaningful to conduct the same mutation test and provide genetic counseling to other relatives of the proband, which can identify other asymptomatic mutation carriers in the family and carry out appropriate life or medical management in advance. More generally, our study expands the spectrum of SPTB mutations, especially in the Chinese population, and increases the current understanding of the molecular mechanisms related to frameshift mutations in SPTB. Moreover, our study also provided an example of using peripheral blood to research the pathogenicity of novel mutations found in HS patients.
Availability of data and material
All data used in this study are available from the corresponding authors for request.
Code availability
Not applicable.
References
Mohandas N, Gallagher PG (2008) Red cell membrane: past, present, and future. Blood 112(10):3939–3948. https://doi.org/10.1182/blood-2008-07-161166
Perrotta S, Gallagher PG, Mohandas N (2008) Hereditary spherocytosis. Lancet 372(9647):1411–1426. https://doi.org/10.1016/s0140-6736(08)61588-3
Bolton-Maggs PH, Langer JC, Iolascon A, Tittensor P, King MJ (2012) Guidelines for the diagnosis and management of hereditary spherocytosis–2011 update. Br J Haematol 156(1):37–49. https://doi.org/10.1111/j.1365-2141.2011.08921.x
Wang C, Cui Y, Li Y, Liu X, Han J (2015) A systematic review of hereditary spherocytosis reported in Chinese biomedical journals from 1978 to 2013 and estimation of the prevalence of the disease using a disease model. Intractable Rare Dis Res 4(2):76–81. https://doi.org/10.5582/irdr.2015.01002
Barcellini W, Bianchi P, Fermo E, Imperiali FG, Marcello AP, Vercellati C et al (2011) Hereditary red cell membrane defects: diagnostic and clinical aspects. Blood Transfus 9(3):274–277. https://doi.org/10.2450/2011.0086-10
Agarwal AM, Nussenzveig RH, Reading NS, Patel JL, Sangle N, Salama ME et al (2016) Clinical utility of next-generation sequencing in the diagnosis of hereditary haemolytic anaemias. Br J Haematol 174(5):806–814. https://doi.org/10.1111/bjh.14131
Delaunay J (2007) The molecular basis of hereditary red cell membrane disorders. Blood Rev 21(1):1–20. https://doi.org/10.1016/j.blre.2006.03.005
Da Costa L, Galimand J, Fenneteau O, Mohandas N (2013) Hereditary spherocytosis, elliptocytosis, and other red cell membrane disorders. Blood Rev 27(4):167–178. https://doi.org/10.1016/j.blre.2013.04.003
An X, Mohandas N (2008) Disorders of red cell membrane. Br J Haematol 141(3):367–375. https://doi.org/10.1111/j.1365-2141.2008.07091.x
Narla J, Mohandas N (2017) Red cell membrane disorders. Int J Lab Hematol 39(Suppl 1):47–52. https://doi.org/10.1111/ijlh.12657
Tole S, Dhir P, Pugi J, Drury LJ, Butchart S, Fantauzzi M et al (2020) Genotype-phenotype correlation in children with hereditary spherocytosis. Br J Haematol 191(3):486–496. https://doi.org/10.1111/bjh.16750
He BJ, Liao L, Deng ZF, Tao YF, Xu YC, Lin FQ (2018) Molecular genetic mechanisms of hereditary spherocytosis: current perspectives. Acta Haematol 139(1):60–66. https://doi.org/10.1159/000486229
Park J, Jeong DC, Yoo J, Jang W, Chae H, Kim J et al (2016) Mutational characteristics of ANK1 and SPTB genes in hereditary spherocytosis. Clin Genet 90(1):69–78. https://doi.org/10.1111/cge.12749
Li H, Durbin R (2010) Fast and accurate long-read alignment with Burrows-Wheeler transform. Bioinformatics 26(5):589–595. https://doi.org/10.1093/bioinformatics/btp698
Zhu Q, Ni Y, Wang J, Yin H, Zhang Q, Zhang L et al (2018) Identification of pathways and genes associated with cerebral palsy. Genes Genomics 40(12):1339–1349. https://doi.org/10.1007/s13258-018-0729-6
Schwarz JM, Cooper DN, Schuelke M, Seelow D (2014) MutationTaster2: mutation prediction for the deep-sequencing age. Nat Methods 11(4):361–362. https://doi.org/10.1038/nmeth.2890
Waterhouse A, Bertoni M, Bienert S, Studer G, Tauriello G, Gumienny R et al (2018) SWISS-MODEL: homology modelling of protein structures and complexes. Nucleic Acids Res 46(W1):W296-w303. https://doi.org/10.1093/nar/gky427
Liu W, Xie Y, Ma J, Luo X, Nie P, Zuo Z et al (2015) IBS: an illustrator for the presentation and visualization of biological sequences. Bioinformatics 31(20):3359–3361. https://doi.org/10.1093/bioinformatics/btv362
Llaudet-Planas E, Vives-Corrons JL, Rizzuto V, Gómez-Ramírez P, Sevilla Navarro J, Coll Sibina MT et al (2018) Osmotic gradient ektacytometry: a valuable screening test for hereditary spherocytosis and other red blood cell membrane disorders. Int J Lab Hematol 40(1):94–102. https://doi.org/10.1111/ijlh.12746
Park SH, Park CJ, Lee BR, Cho YU, Jang S, Kim N et al (2014) Comparison study of the eosin-5’-maleimide binding test, flow cytometric osmotic fragility test, and cryohemolysis test in the diagnosis of hereditary spherocytosis. Am J Clin Pathol 142(4):474–484. https://doi.org/10.1309/ajcpo7v4ogxliipp
Vives-Corrons JL, Krishnevskaya E, Rodriguez IH, Ancochea A (2021) Characterization of hereditary red blood cell membranopathies using combined targeted next-generation sequencing and osmotic gradient ektacytometry. Int J Hematol 113(2):163–174. https://doi.org/10.1007/s12185-020-03010-9
King MJ, Garçon L, Hoyer JD, Iolascon A, Picard V, Stewart G et al (2015) ICSH guidelines for the laboratory diagnosis of nonimmune hereditary red cell membrane disorders. Int J Lab Hematol 37(3):304–325. https://doi.org/10.1111/ijlh.12335
Aggarwal A, Jamwal M, Sharma P, Sachdeva MUS, Bansal D, Malhotra P et al (2020) Deciphering molecular heterogeneity of Indian families with hereditary spherocytosis using targeted next-generation sequencing: first South Asian study. Br J Haematol 188(5):784–795. https://doi.org/10.1111/bjh.16244
Lee JH, Moon KR (2014) Coexistence of gilbert syndrome and hereditary spherocytosis in a child presenting with extreme jaundice. Pediatric Gastroenterol Hepatol Nutr 17(4):266–269. https://doi.org/10.5223/pghn.2014.17.4.266
Yi Y, Dang X, Li Y, Zhao C, Tang H, Shi X (2018) Genetic diagnosis and pathogenic analysis of an atypical hereditary spherocytosis combined with UGT1A1 partial deficiency: a case report. Mol Med Rep 17(1):382–387. https://doi.org/10.3892/mmr.2017.7867
Lindeboom RGH, Vermeulen M, Lehner B, Supek F (2019) The impact of nonsense-mediated mRNA decay on genetic disease, gene editing and cancer immunotherapy. Nat Genet 51(11):1645–1651. https://doi.org/10.1038/s41588-019-0517-5
Mort M, Ivanov D, Cooper DN, Chuzhanova NA (2008) A meta-analysis of nonsense mutations causing human genetic disease. Hum Mutat 29(8):1037–1047. https://doi.org/10.1002/humu.20763
Liu HX, Cartegni L, Zhang MQ, Krainer AR (2001) A mechanism for exon skipping caused by nonsense or missense mutations in BRCA1 and other genes. Nat Genet 27(1):55–58. https://doi.org/10.1038/83762
Perrotta S, Della Ragione F, Rossi F, Avvisati RA, Di Pinto D, De Mieri G et al (2009) Beta-spectrin Bari: a truncated beta-chain responsible for dominant hereditary spherocytosis. Haematologica 94(12):1753–1757. https://doi.org/10.3324/haematol.2009.010124
Acknowledgements
The authors are grateful to the proband and his family for their participation.
Funding
The study was supported by the Gansu Key Laboratory of Genetics Study of Hematopathy (20JR10RA714) and the internal fund from The First Hospital of Lanzhou University (ldyyn2018-69 and ldyyn2020-17).
Author information
Authors and Affiliations
Contributions
Shan Li, Leyuan Mi, Kewang Xi, and Ting Liu performed the research, analyzed the results, and wrote the manuscript. Ping Guo, Xiaojing Chai, Li Lu, and Juan Li designed the study and substantively revised the manuscript. In addition, they intermediated the communication with the proband and his family and conducted a follow-up of two patients. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Ethics approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Consent to participate
Informed consent was obtained from all individual participants included in the study.
Consent for publication
The participant has consented to the submission of the article to the journal.
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Li, S., Guo, P., Mi, L. et al. A novel SPTB mutation causes hereditary spherocytosis via loss-of-function of β-spectrin. Ann Hematol 101, 731–738 (2022). https://doi.org/10.1007/s00277-022-04773-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-022-04773-3