
Abstract
The association between iron overload indices and pathology of the heart and liver in transfusion-dependent patients with β thalassemia major (TM) has been extensively studied. Nonetheless, data on endocrine disease remains limited. This was a cross-sectional study of 382 TM patients treated with regular transfusions and desferrioxamine at the Thalassemia Center in Dubai, UAE. Retrieved data included demographics, splenectomy status, steady-state serum ferritin levels, and the presence of endocrinopathies (diabetes mellitus, hypothyroidism, hypoparathyroidism, and hypogonadism). Multivariate logistic regression analyses were used to determine which variables were independently associated with the occurrence of each endocrinopathy. The mean age of patients was 15.4 ± 7.6 years, with an equal sex distribution. The mean serum ferritin level was 2597.2 ± 1976.8 μg/l. The frequencies of specific endocrinopathies were diabetes mellitus (10.5%), hypothyroidism (6.3%), hypoparathyroidism (10.5%), and hypogonadism (25.9%). On multivariate logistic regression analysis, patients with a serum ferritin level >2,500 μg/l, but not >1,000–2,500 μg/l, were 3.53 times (95% CI 1.09–11.40) more likely to have diabetes mellitus, 3.25 times (95% CI 1.07–10.90) more likely to have hypothyroidism, 3.27 times (95% CI 1.27–8.39) more likely to have hypoparathyroidism, and 2.75 times (95% CI 1.38–5.49) more likely to have hypogonadism compared to patients with a serum ferritin level ≤1,000 μg/l. However, splenectomized patients with serum ferritin levels ≤2,500 μg/l had comparably high rates of all endocrinopathies as patients with serum ferritin levels >2,500 μg/l. Endocrinopathy is common in TM patients treated with desferrioxamine therapy, especially in patients with serum ferritin levels >2,500 μg/l or those splenectomized.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In patients with β thalassemia major (TM), long-term transfusion therapy for the correction of anemia results in toxic iron overload. The level of iron overload is generally proportional to the number of transfused units and is cumulative [1, 2]. Uncontrolled iron overload has serious clinical consequences resulting in significant morbidity and mortality. Frequent manifestations include liver damage, cardiac disease, and endocrine dysfunction. Iron overload can also result in arthropathy, neurodegenerative disorders, hyperpigmentation, pulmonary hypertension, and carcinogenesis [1, 3]. Cardiac disease caused by transfusional iron overload remains the principal cause of death in patients with TM over the past 25 years, which was largely attributed to poor compliance with the subcutaneous iron chelator desferrioxamine [4–6]. Studies have identified a significantly lower risk of cardiac disease and death in at least two thirds of cases where serum ferritin levels have been maintained below 2,500 μg/l over a period of a decade or more [4]. Observations with larger patient numbers show that maintenance of an even lower serum ferritin of 1,000 μg/l may be associated with additional advantages [7]. Nonetheless, with the advent of orally active chelating drugs and novel imaging techniques for the detection of iron overload in the heart (T2* magnetic resonance imaging [MRI]), the relative risk of death from iron-induced cardiomyopathy continues to fall [8]. The case with other organs, like the endocrine glands, has not been extensively evaluated. Such study remains essential to be able to provide holistic management to patients with TM, by aiming to prevent morbidity as well as mortality. In this study, we evaluate the rate of endocrine complications in a group of TM patients medically treated with regular transfusions and desferrioxamine. Association between the occurrence of endocrinopathy and serum ferritin levels is also determined.
Materials and methods
This was a cross-sectional study of all living transfusion-dependent TM patients registered at the Thalassemia Center in Dubai, UAE, until the end of 2006 (n = 382). Diagnosis of TM was based on clinical history and laboratory confirmation by hemoglobin electrophoresis and DNA testing. The mean age at diagnosis was 10.1 months (range 2–40 months). All patients were treated with the same protocol at the center. Following diagnosis, regular transfusions are administered every 3–4-week intervals with the aim of maintaining a pretransfusion hemoglobin level of 90–95 g/l. The mean age at the start of transfusion therapy was 17.4 months (range 2–60 months). Iron chelation therapy is initiated after 1 year of regular transfusion therapy and when serum ferritin level reaches around 1,000 μg/l, using subcutaneous desferrioxamine at an average dose of 40 mg/kg/day used for 5–6 nights per week over 10–12 h.
For this analysis, retrieved data included demographics (age and sex), splenectomy status, and steady-state serum ferritin levels. Data was also retrieved for the presence of each of four endocrinopathies: 1. diabetes mellitus: a fasting blood sugar level ≥126 mg/dl, or 2-h postprandial blood sugar level ≥200 mg/dl, or symptoms of hyperglycemia and a casual (random) plasma glucose level ≥200 mg/dl [9]; 2. hypothyroidism: a thyroid stimulating hormone level >4.7 μU/l and a free T4 level <0.8 ng/dl [10]; 3. hypoparathyroidism: normal or inappropriately low intact parathyroid hormone level in a patient with subnormal serum albumin corrected total or ionized calcium values, after hypomagnesemia has been ruled out (evaluation for vitamin D deficiency was not a common practice at the time of diagnosis) [11]; 4. hypogonadism: absence of breast development in girls by the age of 15 years and absence of testicular enlargement in boys by the age of 17 years [7].
For each specific endocrinopathy, patients were divided as cases and controls. For cases, the retrieved age was that at diagnosis of the endocrinopathy, and the retrieved steady-state serum ferritin level was the mean of all available serial laboratory records in the 2 years prior to the diagnosis of the endocrinopathy. For controls, retrieved age was that at the time of analysis and retrieved steady-state serum ferritin level was the mean of all available serial laboratory records of the 2 years prior to analysis.
Statistical analysis
Descriptive statistics are expressed as means ± standard deviation (SD) or percentages. Bivariate analysis was performed to determine the association between serum ferritin levels and study variables using the independent-samples t-test (for sex and splenectomy status) and the Pearson’s correlation coefficient (for age). Differences in serum ferritin levels and other study variables between cases and controls for each endocrinopathy were evaluated by the independent-samples t-test and the chi-square test. Multivariate logistic regression analyses were used to determine which variables were significantly and independently associated with each endocrinopathy. The modifying effect of splenectomy on the association between serum ferritin level and the rate of endocrinopathies was evaluated by the chi-square and Fisher’s exact tests. All P-values are two sided with the level of significance set at <0.05.
Results
Patients characteristics
A total of 382 patients were included in this analysis. The mean age of patients was 15.4 ± 7.6 years (range 2–37 years), with 192 patients (50.3%) being males. Thirty patients (7.9%) were splenectomized. The mean serum ferritin level for the whole sample at the time of study was 2597.2 ± 1976.8 μg/l (range 175–12,788 μg/l), with 41 patients (10.7%) having serum ferritin levels ≤1,000 μg/l, 207 patients (54.2%) having serum ferritin levels >1,000–2,500 μg/l, and 134 patients (35.1%) having serum ferritin levels >2,500 μg/l. There was a significant positive correlation between serum ferritin level and age but with poor linearity (r = 0.416, P < 0.001). Serum ferritin levels were comparable between males and females (P = 0.697).
A total of 122 patients (31.9%) had at least one endocrinopathy and 53 patients (13.9%) had multiple endocrinopathies. The frequencies of specific endocrinopathies were as follows: diabetes mellitus (n = 40, 10.5%), hypothyroidism (n = 24, 6.3%), hypoparathyroidism (n = 40, 10.5%), and hypogonadism (n = 99, 25.9%).
Serum ferritin levels vs. endocrinopathy
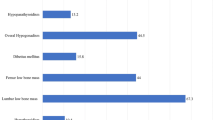
Mean serum ferritin levels were significantly higher in patients with diabetes mellitus, hypothyroidism, hypoparathyroidsim, and hypogonadism compared to patients without these endocrinopathies (Fig. 1). Bivariate associations between other study parameters and the specific endocrinopathies are summarized in Table 1. On multivariate logistic regression analysis, and after adjusting for age, sex, and splenectomy status, patients with a serum ferritin level >2,500 μg/l, but not >1,000–2,500 μg/l, were 3.53 times (95% confidence interval [CI] 1.09–11.40) more likely to have diabetes mellitus, 3.25 times (95% CI 1.07–10.90) more likely to have hypothyroidism, 3.27 times (95% CI 1.27–8.39) more likely to have hypoparathyroidism, and 2.75 times (95% CI 1.38–5.49) more likely to have hypogonadism compared to patients with a serum ferritin level ≤1,000 μg/l (Table 2). Splenectomy was also independently and significantly associated with higher adjusted odds of all endocrinopathies.

Comparison of mean serum ferritin levels in patients with and without endocrinopathy. Data presented as means (squares) and standard deviations (whiskers)
A closer look at the effect of splenectomy
The mean age at splenectomy was 8.3 ± 5.3 years (range 4–21 years) which preceded the patients current analysis by 16.6 ± 6.7 years (range 3–25 years). The indication for splenectomy was hypersplenism in 14 (46.6%) patients and hypersplenism with splenomegaly in 16 (53.4%) patients. All patients were already on regular transfusion therapy at the time of splenectomy, and the mean serum ferritin level was significantly higher in splenectomized compared to non-splenectomized patients (3,392 ± 2599.3 vs. 2529.5 ± 1903.9 μg/l, P = 0.022).
Splenectomy significantly increased the rates of all endocrinopathies in both patients with serum ferritin levels ≤ and >2,500 μg/l (Fig. 2). However, the significantly increased rate of endocrinopathies observed in patients with serum ferritin levels >2,500 μg/l compared to patients with ≤2,500 μg/l was only evident in the non-splenectomized group. Splenectomized patients with serum ferritin levels ≤2,500 μg/l had comparably high rates of all endocrinopathies as patients with serum ferritin levels >2,500 μg/l (Fig. 2).

Flow diagrams showing the modifying effect of splenectomy on the association between serum ferritin levels and the rate of a diabetes mellitus, b hypothyroidism, c hypoparathyroidism, and d hypogonadism. Data analyzed through the chi-square and Fisher’s exact tests
Discussion
In this study, we demonstrated that endocrinopathy is common in TM patients treated with subcutaneous desferrioxamine therapy and is most probably attributed to poor compliance with therapy as reflected by high levels of serum ferritin. Moreover, we identified a good association between serum ferritin levels and the occurrence of endocrinopathy. Patients with serum ferritin levels >2,500 μg/l, but not >1,000–2,500 μg/l, had higher odds of endocrine morbidity compared to patients with levels ≤1,000 μg/l. Interestingly, splenectomy was also strongly associated with the occurrence of endocrine disease.
The rate of endocrinopathy in our cohort is similar to previously published reports from western countries, evaluating TM patients maintained on desferrioxamine therapy [7, 12, 13]. Based on the findings in this report, one cannot determine if this is attributed to suboptimal efficacy of desferrioxamine in chelating iron from endocrine organs or to poor compliance with therapy. However, noting the high mean serum ferritin level in our patients despite adequate dosing, it seems more likely that poor compliance is the major factor. Although desferrioxamine has served TM patients for more than four decades, the burden of prolonged and regular subcutaneous infusions reflected negatively on patients’ psychosocial stability and quality of life [14]. Patients with TM are surviving longer and thus given the opportunity to interact more deeply with society, which could substantially accentuate compliance issues [15]. Thus, novel advances in oral iron chelation therapy became the highlight of TM management for the past two decades. The two available oral chelators, deferiprone and deferasirox, have been extensively evaluated for their efficacy and safety in removing cardiac and hepatic iron [16–18]. Nonetheless, data on the efficacy and safety of the two agents in preventing or managing iron toxicity and dysfunction in endocrine glands are limited, and more studies are awaited [19–23].
We found a significant association between serum ferritin levels and the rate of endocrinopathy, in agreement with previous studies [20, 24–26]. Serum ferritin measurement has traditionally been the method of choice within the clinic as it is easy to assess, inexpensive, and provides repeat serial measures that are useful for monitoring chelation therapy. Several studies have shown an association between the level of serum ferritin, especially in serial measurements, and prognosis in TM patients [4, 6, 27, 28]. A lower risk of cardiac disease and death were observed in patients with serum ferritin levels maintained below 2,500 μg/l over a period of a decade or more [4]. Maintenance of an even lower serum ferritin (< 1,000 μg/l) was associated with additional protection from cardiac disease and death [7]. Our study adds to these established thresholds by showing that patients with serum ferritin >2,500 μg/l are also at increased risk of endocrine morbidity. This level is similar to that reported in the few studies that tried to establish practical thresholds [20, 25]. This finding remains essential in light of recent advances in the management of cardiac siderosis in TM, where the incidence of cardiac death is expected to decline [8]. However, several limitations exist concerning the use of serum ferritin. It represents an indirect measurement of iron burden and fluctuates in response to inflammation, abnormal liver function, and ascorbate deficiency. Radiological techniques are gradually becoming the new standard for iron overload quantification in target organs. Hepatic (R2 and T2*) and cardiac (T2*) MRI relaxation time techniques have been calibrated against biopsy specimens, and results achieved international reproducibility [29–33]. MRI evaluation of iron content for some endocrine glands, mainly the pancreas and pituitary, also appears to be feasible [34–38]. However, MRI techniques are not always available, especially in developing countries with limited health care resources, where serum ferritin measurement is the only available option. Results on the relationship between serum ferritin levels and MRI-derived iron content in target organs are either lacking or conflicting [29–38]. Evaluation of the utility of serial ferritin measurement, as well as specific markers of dysfunction, to predict tissue iron content and morbidity remains essential.
Similar to other studies, splenectomy was associated with higher occurrence of endocrinopathy [20, 24, 39]. This may, again, be attributed to iron overload reflected by higher serum ferritin levels in splenectomized compared to non-splenectomized patients. The intact spleen may be a reservoir of excess iron and may have a possible scavenging effect on iron free fractions including non-transferrin-bound iron [40]. A role for splenectomy in increased cardiac siderosis has recently been suggested [41]. Nonetheless, splenectomy was also associated with higher rates of endocrinopathy in patients with low serum ferritin levels, suggesting that other contributing factors may be involved. The need for splenectomy has been traditionally regarded as marker of severe disease (ineffective erythropoiesis), and splenectomised patients show higher levels of hemolyzed, prothrombotic red blood cells and subsequent thrombin generation [42–44]. These factors have been implicated in the pathogenesis of several morbidities in thalassemia patients [45–48]; whether they contribute to the mechanism of endocrine in this patient population disease merits further study.
The main limitation of our study is the lack of objective assessment of compliance. Such evaluation is essential to be able to confirm the reason behind failure of desferrioxamine therapy to prevent iron-related complications.
Our study should raise awareness to the high occurrence of endocrine disease in TM patients non-compliant to desferrioxamine therapy. It also highlights that serum ferritin measurement associates well with the rate of endocrinopathy and may be used to tailor chelation therapy targeted towards prevention of these complications. Further prospective studies are needed to confirm these findings.
References
Hershko C (2010) Pathogenesis and management of iron toxicity in thalassemia. Ann N Y Acad Sci 1202:1–9
Cohen AR, Glimm E, Porter JB (2008) Effect of transfusional iron intake on response to chelation therapy in beta-thalassemia major. Blood 111:583–587
Taher AT, Musallam KM, Inati A (2009) Iron overload: consequences, assessment, and monitoring. Hemoglobin 33(Suppl 1):S46–S57
Olivieri NF, Nathan DG, MacMillan JH, Wayne AS, Liu PP, McGee A, Martin M, Koren G, Cohen AR (1994) Survival in medically treated patients with homozygous beta-thalassemia. N Engl J Med 331:574–578
Borgna-Pignatti C, Rugolotto S, De Stefano P, Piga A, Di Gregorio F, Gamberini MR, Sabato V, Melevendi C, Cappellini MD, Verlato G (1998) Survival and disease complications in thalassemia major. Ann N Y Acad Sci 850:227–231
Gabutti V, Piga A (1996) Results of long-term iron-chelating therapy. Acta Haematol 95:26–36
Borgna-Pignatti C, Rugolotto S, De Stefano P, Zhao H, Cappellini MD, Del Vecchio GC, Romeo MA, Forni GL, Gamberini MR, Ghilardi R, Piga A, Cnaan A (2004) Survival and complications in patients with thalassemia major treated with transfusion and deferoxamine. Haematologica 89:1187–1193
Modell B, Khan M, Darlison M, Westwood MA, Ingram D, Pennell DJ (2008) Improved survival of thalassaemia major in the UK and relation to T2* cardiovascular magnetic resonance. J Cardiovasc Magn Reson 10:42
Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, Zinman B (2009) Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 32:193–203
Baskin HJ, Cobin RH, Duick DS, Gharib H, Guttler RB, Kaplan MM, Segal RL (2002) American Association of Clinical Endocrinologists medical guidelines for clinical practice for the evaluation and treatment of hyperthyroidism and hypothyroidism. Endocr Pract 8:457–469
Shoback D (2008) Clinical practice. Hypoparathyroidism. N Engl J Med 359:391–403
Thuret I, Pondarre C, Loundou A, Steschenko D, Girot R, Bachir D, Rose C, Barlogis V, Donadieu J, de Montalembert M, Hagege I, Pegourie B, Berger C, Micheau M, Bernaudin F, Leblanc T, Lutz L, Galacteros F, Simeoni MC, Badens C (2010) Complications and treatment of patients with beta-thalassemia in France: results of the National Registry. Haematologica 95:724–729
Cunningham MJ, Macklin EA, Neufeld EJ, Cohen AR (2004) Complications of beta-thalassemia major in North America. Blood 104:34–39
Delea TE, Edelsberg J, Sofrygin O, Thomas SK, Baladi JF, Phatak PD, Coates TD (2007) Consequences and costs of noncompliance with iron chelation therapy in patients with transfusion-dependent thalassemia: a literature review. Transfusion 47:1919–1929
Musallam K, Cappellini MD, Taher A (2008) Challenges associated with prolonged survival of patients with thalassemia: transitioning from childhood to adulthood. Pediatrics 121:e1426–e1429
Piga A, Roggero S, Salussolia I, Massano D, Serra M, Longo F (2010) Deferiprone. Ann N Y Acad Sci 1202:75–78
Galanello R, Agus A, Campus S, Danjou F, Giardina PJ, Grady RW (2010) Combined iron chelation therapy. Ann N Y Acad Sci 1202:79–86
Brittenham GM (2011) Iron-chelating therapy for transfusional iron overload. N Engl J Med 364:146–156
Farmaki K, Tzoumari I, Pappa C (2011) Oral chelators in transfusion-dependent thalassemia major patients may prevent or reverse iron overload complications. Blood Cells Mol Dis 47:33–40
Gamberini MR, De Sanctis V, Gilli G (2008) Hypogonadism, diabetes mellitus, hypothyroidism, hypoparathyroidism: incidence and prevalence related to iron overload and chelation therapy in patients with thalassaemia major followed from 1980 to 2007 in the Ferrara Centre. Pediatr Endocrinol Rev 6(Suppl 1):158–169
Farmaki K, Tzoumari I, Pappa C, Chouliaras G, Berdoukas V (2010) Normalisation of total body iron load with very intensive combined chelation reverses cardiac and endocrine complications of thalassaemia major. Br J Haematol 148:466–475
Wang CH, Wu KH, Tsai FJ, Peng CT, Tsai CH (2006) Comparison of oral and subcutaneous iron chelation therapies in the prevention of major endocrinopathies in beta-thalassemia major patients. Hemoglobin 30:257–262
Platis O, Anagnostopoulos G, Farmaki K, Posantzis M, Gotsis E, Tolis G (2004) Glucose metabolism disorders improvement in patients with thalassaemia major after 24–36 months of intensive chelation therapy. Pediatr Endocrinol Rev 2(Suppl 2):279–281
Jaruratanasirikul S, Chareonmuang R, Wongcharnchailert M, Laosombat V, Sangsupavanich P, Leetanaporn K (2008) Prevalence of impaired glucose metabolism in beta-thalassemic children receiving hypertransfusions with a suboptimal dosage of iron-chelating therapy. Eur J Pediatr 167:873–876
Shalitin S, Carmi D, Weintrob N, Phillip M, Miskin H, Kornreich L, Zilber R, Yaniv I, Tamary H (2005) Serum ferritin level as a predictor of impaired growth and puberty in thalassemia major patients. Eur J Haematol 74:93–100
Jensen CE, Tuck SM, Old J, Morris RW, Yardumian A, De Sanctis V, Hoffbrand AV, Wonke B (1997) Incidence of endocrine complications and clinical disease severity related to genotype analysis and iron overload in patients with beta-thalassaemia. Eur J Haematol 59:76–81
Telfer PT, Prestcott E, Holden S, Walker M, Hoffbrand AV, Wonke B (2000) Hepatic iron concentration combined with long-term monitoring of serum ferritin to predict complications of iron overload in thalassaemia major. Br J Haematol 110:971–977
Davis BA, O’Sullivan C, Jarritt PH, Porter JB (2004) Value of sequential monitoring of left ventricular ejection fraction in the management of thalassemia major. Blood 104:263–269
Carpenter JP, He T, Kirk P, Roughton M, Anderson LJ, de Noronha SV, Sheppard MN, Porter JB, Walker JM, Wood JC, Galanello R, Forni G, Catani G, Matta G, Fucharoen S, Fleming A, House MJ, Black G, Firmin DN, St Pierre TG, Pennell DJ (2011) On T2* magnetic resonance and cardiac iron. Circulation 123:1519–1528
St Pierre TG, Clark PR, Chua-anusorn W, Fleming AJ, Jeffrey GP, Olynyk JK, Pootrakul P, Robins E, Lindeman R (2005) Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood 105:855–861
Wood JC, Enriquez C, Ghugre N, Tyzka JM, Carson S, Nelson MD, Coates TD (2005) MRI R2 and R2* mapping accurately estimates hepatic iron concentration in transfusion-dependent thalassemia and sickle cell disease patients. Blood 106:1460–1465
Kirk P, He T, Anderson LJ, Roughton M, Tanner MA, Lam WW, Au WY, Chu WC, Chan G, Galanello R, Matta G, Fogel M, Cohen AR, Tan RS, Chen K, Ng I, Lai A, Fucharoen S, Laothamata J, Chuncharunee S, Jongjirasiri S, Firmin DN, Smith GC, Pennell DJ (2010) International reproducibility of single breathhold T2* MR for cardiac and liver iron assessment among five thalassemia centers. J Magn Reson Imaging 32:315–319
Anderson LJ, Holden S, Davis B, Prescott E, Charrier CC, Bunce NH, Firmin DN, Wonke B, Porter J, Walker JM, Pennell DJ (2001) Cardiovascular T2-star (T2*) magnetic resonance for the early diagnosis of myocardial iron overload. Eur Heart J 22:2171–2179
de Assis RA, Ribeiro AA, Kay FU, Rosemberg LA, Nomura CH, Loggetto SR, Araujo AS, Fabron Junior A, de Almeida Verissimo MP, Baldanzi GR, Esposito BP, Baroni RH, Wood JC, Hamerschlak N (2011) Pancreatic iron stores assessed by magnetic resonance imaging (MRI) in beta thalassemic patients. Eur J Radiol
Restaino G, Meloni A, Positano V, Missere M, Rossi G, Calandriello L, Keilberg P, Mattioni O, Maggio A, Lombardi M, Sallustio G, Pepe A (2011) Regional and global pancreatic T*2 MRI for iron overload assessment in a large cohort of healthy subjects: normal values and correlation with age and gender. Magn Reson Med 65:764–769
Au WY, Lam WW, Chu W, Tam S, Wong WK, Liang R, Ha SY (2008) A T2* magnetic resonance imaging study of pancreatic iron overload in thalassemia major. Haematologica 93:116–119
Noetzli LJ, Papudesi J, Coates TD, Wood JC (2009) Pancreatic iron loading predicts cardiac iron loading in thalassemia major. Blood 114:4021–4026
Wood JC, Noetzl L, Hyderi A, Joukar M, Coates T, Mittelman S (2010) Predicting pituitary iron and endocrine dysfunction. Ann N Y Acad Sci 1202:123–128
Skordis N, Michaelidou M, Savva SC, Ioannou Y, Rousounides A, Kleanthous M, Skordos G, Christou S (2006) The impact of genotype on endocrine complications in thalassaemia major. Eur J Haematol 77:150–156
Tavazzi D, Duca L, Graziadei G, Comino A, Fiorelli G, Cappellini MD (2001) Membrane-bound iron contributes to oxidative damage of beta-thalassaemia intermedia erythrocytes. Br J Haematol 112:48–50
Aydinok Y, Bayraktaroglu S, Yildiz D, Alper H (2011) Myocardial iron loading in patients with thalassemia major in Turkey and the potential role of splenectomy in myocardial siderosis. J Pediatr Hematol Oncol 33:374–378
Eldor A, Rachmilewitz EA (2002) The hypercoagulable state in thalassemia. Blood 99:36–43
Rund D, Rachmilewitz E (2005) Beta-thalassemia. N Engl J Med 353:1135–1146
Cappellini MD, Motta I, Musallam KM, Taher AT (2010) Redefining thalassemia as a hypercoagulable state. Ann N Y Acad Sci 1202:231–236
Atichartakarn V, Likittanasombat K, Chuncharunee S, Chandanamattha P, Worapongpaiboon S, Angchaisuksiri P, Aryurachai K (2003) Pulmonary arterial hypertension in previously splenectomized patients with beta-thalassemic disorders. Int J Hematol 78:139–145
Crary SE, Buchanan GR (2009) Vascular complications after splenectomy for hematologic disorders. Blood 114:2861–2868
Phrommintikul A, Sukonthasarn A, Kanjanavanit R, Nawarawong W (2006) Splenectomy: a strong risk factor for pulmonary hypertension in patients with thalassaemia. Heart 92:1467–1472
Aessopos A, Farmakis D, Deftereos S, Tsironi M, Polonifi A, Moyssakis I, Diamanti-Kandaraki E, Papalambros E (2005) Cardiovascular effects of splenomegaly and splenectomy in beta-thalassemia. Ann Hematol 84:353–357
Acknowledgment
This study was supported by the Dubai Health Authority–Thalassemia Centre. Financial support for medical editorial assistance was provided by Novartis Pharmaceuticals.
Conflicts of interest
ATT is a member of Novartis Speakers’ Bureau.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Belhoul, K.M., Bakir, M.L., Saned, MS. et al. Serum ferritin levels and endocrinopathy in medically treated patients with β thalassemia major. Ann Hematol 91, 1107–1114 (2012). https://doi.org/10.1007/s00277-012-1412-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-012-1412-7