
Abstract
Covert brain infarction is an emerging concern in patients with β-thalassemia intermedia (TI). We have recently observed a high prevalence (60%) of silent brain infarction on brain magnetic resonance imaging (MRI) in 30 splenectomized adults with TI. In this work, we further evaluate cerebral involvement in the same 30 patients using fluorodeoxyglucose positron emission tomography–computed tomography (PET-CT) scanning. The median age was 32 years (range, 18–54 years) with a male to female ratio of 13:17. Nineteen patients (63.3%) had evidence of decreased neuronal function on PET-CT. Involvement was mostly left sided, multiple, and most commonly in the temporal and parietal lobes. Elevated liver iron concentration, beyond 15 mg Fe/g dry weight, characterized patients with decreased neuronal function. The concordance rate between brain MRI and PET-CT for the detection of brain abnormality was only 36.7% (Kappa 0.056, P = 0.757), highlighting that both modalities reveal different types of brain pathology. Decreased neuronal function is a common finding in patients with TI and is associated with iron overload. Moreover, the addition of PET-CT to MRI identifies a greater proportion of TI patients with silent neuroimaging abnormalities.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
It is now apparent that β-thalassemia intermedia (TI) carries more complexity than traditionally recognized [1]. Patients with TI have milder anemia compared to patients with β-thalassemia major (TM), usually present later in childhood, and remain largely transfusion independent [2]. However, the diagnosis of TI is now also associated with several serious morbidities like thromboembolic phenomena [3]. Hypercoagulability in TI results from a combination of several factors including a procoagulant activity of hemolyzed circulating red blood cells, increased platelet activation, coagulation factor defects, depletion of antithrombotic factors, endothelial inflammation, among others [3]. Clinically, the risk of thromboembolic events increases with age [4–6] and is much higher in splenectomized and never-transfused patients [5–8] in whom hypercoagulability is thought to be much more prominent [7, 9]. Reported thromboembolic events were most commonly venous [5–8]. Strokes, on the other hand, are less frequent in TI compared to TM patients [6] since patients with TM have several other comorbidities that increase stroke risk like diabetes mellitus, cardiac dysfunction, and arrhythmias [10]. Nevertheless, one study showed that 37.5% of patients with TI have asymptomatic brain damage on magnetic resonance imaging (MRI) [11]. In this line, we conducted a brain MRI study on 30 splenectomized adults with TI who were neurologically intact [12]. The rate of silent brain infarcts was as high as 60%. The occurrence and multiplicity of the detected lesions were associated with older age and transfusion naivety [12]. In this current work and for the first time, we evaluate the results of brain fluorodeoxyglucose (18F-FDG) positron emission tomography–computed tomography (PET-CT) scanning in the same 30 patients to further understand cerebral involvement in this patient population.
Materials and methods
Patients
This was a prospective study conducted on all splenectomized TI patients aged 18 years or older (n = 43) attending the Chronic Care Center (Lebanon) between June and December 2008. All patients were diagnosed with TI based on previously described criteria [13]. None of the patients had Hb S, Hb C, Hb E/β, or δβ-thalassemia, coinheritance of α-thalassemia, or coinheritance of determinants associated with increased γ chain production. Exclusion criteria, actively screened for, are summarized in Table 1. After screening patients for exclusion criteria, 30 patients were found eligible and were recruited in the study. The study was approved by the institutional review board of the center and written consents were obtained from all patients.
Patient charts were reviewed for demographics (age and gender) and any history of transfusion therapy. Blood samples were obtained for the assessment of total hemoglobin level, platelet counts, and steady-state serum ferritin levels. Direct determination of liver iron concentration (LIC) was performed by R2 MRI using established methodology [14]. Brain MRI and PET-CT studies were done for all patients on the same day.
Brain MRI
Brain MRIs were conducted as previously published [12]. In brief, they were performed on a 3.0-T, eight-channel head coil, Achieva Philips Scanner using axial T1-weighted images (repetition time/echo delay time (TR/TE), 450/10), T2-weighted gradient echo images (TR/TE, 731/16), fluid-attenuated inversion recovery (FLAIR) images (TR/TE, 11,000/125), and diffusion-weighted imaging (TR/TE, 2,312/68). Coronal FLAIR images (TR/TE, 11,000/125) as well as coronal and sagittal T2-weighted images (TR/TE, 3,000/80) were also obtained. No contrast material was administered. Two blinded neuroradiologists reviewed the studies, looking for ischemic lesions. Infarction or ischemic lesions were defined as areas of abnormally increased signal intensity on the T2- and FLAIR-weighted sequences and were classified by anatomic location.
PET-CT
Brain PET-CT was done on the same day as MRI for all patients. Before undergoing PET-CT, patients were asked to fast for at least 6 h, although oral hydration with glucose-free water was allowed. After ensuring a normal blood glucose level in the peripheral circulation, the patients received an intravenous injection of 370 MBq (10 mCi) 18F-FDG and allowed to rest for 45 min before undergoing scanning. Scans were acquired with a PET scanner combined with a multisection CT scanner (Biograph 6, Siemens). The axes of the two systems were mechanically aligned such that a patient can be moved from the CT to the PET gantry by moving the examination table. CT scanning of the brain was performed according to a standardized protocol, and immediately afterwards, PET scanning was performed with the identical transverse field of view. The acquisition time for PET in static mode was 30 min. The CT data were resized from a 512 × 512 to a 128 × 128 matrix to match the PET data so that scans can be fused and CT-based transmission maps generated. PET data sets were reconstructed iteratively using an ordered subset expectation maximization algorithm with segmented attenuation correction. Coregistered scans were then displayed on a workstation with commercially available software (e.soft from Siemens). Visual assessment was determined by two blinded nuclear medicine physicians. Visual (qualitative) interpretation was based on the subjective impression of the degree of 18F-FDG uptake. Decreased uptake was defined as the relative decrease in 18F-FDG uptake in a lobe compared to other lobes, which reflects a decrease of neuronal function (glucose utilization). Review was done independently, and in case of disagreement (two cases), the two experts reviewed the images jointly until a consensus was reached.
Statistical analysis
Descriptive data are presented as medians (range) or percentages. Bivariate correlations between PET-CT abnormality and study parameters were evaluated using the Mann–Whitney U test, the Chi-square test, and the Fisher's exact test. A logistic regression analysis was performed to evaluate the probability of a decreased neuronal function on PET-CT, using the variable found to be statistically significant in the bivariate analysis as an independent continuous variable. To determine the optimal variable cutoff for the logistic regression equation that best predicts PET-CT abnormality, receiver operating characteristic (ROC) curve analysis was performed [15]. A concordance Kappa value was calculated for the agreement between brain MRI and PET-CT for the detection of abnormalities. A Kappa value of 1 indicates complete agreement and a value of 0 indicates no agreement at all. All P values were two-sided with the level of significance set at <0.05.
Results
Patients' characteristics
A total of 30 patients were included in the analysis. The median age was 32 years (range, 18–54 years) with a male to female ratio of 13:17. Most patients were transfusion independent (n = 18, 60%) while 12 patients (40%) were occasionally transfused during infections, surgery, or pregnancy. None of the patients were on iron chelation or hydroxyurea therapy. The median total hemoglobin level was 84 g/l (range, 49–131 g/l) and the median platelet count was 789.5 × 109/l (range, 189–1,602 × 109/l). The median serum ferritin level was 1,127.5 μg/l (range, 116–3,158 μg/l) and the median LIC was 10.75 mg Fe/g dry weight (dw) (range, 1–32.1 mg Fe/g dw).
PET-CT
Nineteen patients (63.3%) had evidence of decreased neuronal function on PET-CT. Only 1 patient had bilateral brain involvement while the remaining 18 had left brain involvement. Five (26.3%) out of the 19 patients had single lobe involvement while 14 (73.7%) had multiple lobes involved (11 had two, 3 had three lobes involved). The temporal lobe was most commonly involved (n = 18, 94.7%), followed by the parietal (n = 14, 73.7%) and frontal lobes (n = 3, 15.8%). The occipital lobe was not involved in any patient.
Risk factors for decreased neuronal function
There was no statistically significant correlation between the evidence of decreased neuronal function on PET-CT and any of age, gender, transfusion history, total hemoglobin level, or platelet count. The median serum ferritin level was higher in patients with PET-CT abnormality than those without (1,215 vs. 861.5 μg/l), although the association did not reach statistical significance (P = 0.053). Moreover, the median LIC was significantly higher in patients with evidence of decreased neuronal activity than those without (16.3 vs. 3.4 mg Fe/g dw, P = 0.003). A logistic regression model was also performed to estimate the probability of abnormality on PET-CT using LIC as an independent variable (Fig. 1). The model was significant (P < 0.001) and had a predictive value of 76.7%. On ROC curve analysis, a LIC cutoff of 15 mg Fe/g dw was the best predictor of decreased neuronal function on PET-CT with an area under the curve of 0.828 ± 0.075 (95% confidence interval 0.681–0.975, P = 0.003), a sensitivity of 52.6%, and a specificity of 100%.

Logistic regression curve showing the probability or PET-CT abnormality as a function of LIC
PET-CT vs. brain MRI
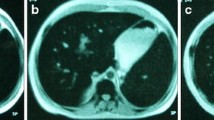
Among the group of 30 patients, 18 (60%) had evidence of silent infarcts on brain MRI, all in the white matter [12]. A total of 11 patients (36.7%) had evidence of brain abnormality on both MRI and PET-CT while 26 patients (86.7%) had evidence of brain abnormality on either MRI or PET-CT (Table 2). The concordance rates between brain MRI and PET-CT were 36.7% for the detection of abnormality (Kappa 0.056, P = 0.757); 23.3% for the detection of multiple abnormalities (Kappa 0.062, P = 0.732); 3.3% for the detection of bilateral brain abnormality (Kappa 0.086, P = 0.245); and 6.7% (Kappa 0.036, P = 0.713), 10% (Kappa 0.164, P = 0.338), 3.3% (Kappa 0.045, P = 0.406), and 0% (Kappa N/A, P = N/A) for the detection of frontal, parietal, temporal, or occipital abnormalities, respectively (Fig. 2).

Example of poor concordance between brain MRI and PET-CT. A 30-year-old female with a two ischemic lesions (<0.5 cm, arrows) in the right frontal and parietal lobes on MRI and b hypometabolism in the left parietal and temporal lobes on PET-CT
Discussion
Unlike MRI, PET-CT imaging does not seem helpful in detecting silent white matter infarcts in patients with TI. Nevertheless, PET-CT imaging revealed that decreased neuronal function is a common finding in this patient population, which is associated with iron overload. Thus, the addition of PET-CT to MRI identifies a greater proportion of TI patients with silent neuroimaging abnormalities and provides additional information on the neurophysiologic status of these patients.
The association of iron overload, evident from the elevated LIC, with decreased neuronal function on PET-CT in our study is the first report of its kind for patients with hemoglobinopathies. Transfusion-independent patients with TI still develop iron overload due to increased intestinal absorption and show considerably high levels of LIC [16, 17], which may explain why both transfused and nontransfused patients had similar rates of PET-CT abnormality in our study. Although cardiac siderosis and disease do not seem to be a consequence of iron overload in this patient population [18–20], an association with other clinical complications in several organ systems has been observed [5]. Although a causal relationship may be hard to confirm, our study adds brain involvement to the growing list of iron overload-related morbidity in TI patients. Iron is an essential element for the multiple functions of the brain. The abnormal distribution of brain iron has been implicated in neuronal injury and death in several neurodegenerative diseases such as Parkinson's disease, Alzheimer's disease, and amyotrophic lateral sclerosis. Multiple iron chelators have been shown to possess neuroprotective and neurorestorative properties in these diseases, suggesting that iron chelation might be promising therapeutics [21]. Whether the same applies for patients with TI merits further evaluation. The risk factors for silent brain infarcts detected on MRI remain different. There is no evidence that iron overload can be associated with cerebral small vessel disease or silent infarcts [12]. In fact, transfusion therapy seems to be protective against the development of these silent white matter lesions [12], probably due to the beneficial role of transfusions in improving hypercoagulability and vascular disease in TI by decreasing the concentrations of damaged red blood cells with thrombogenic potential, among other factors [3]. Although the occurrence and multiplicity of silent brain infarcts increase with age in TI patients [12], such observation was not noted for the decrease in neuronal function detected on PET-CT. In line with our findings, it could be hypothesized that neuronal damage could occur early on with direct iron toxicity, unlike vascular damage where the accumulation of risk factors over time may be necessary.
Most acquired knowledge on cerebral involvement in hemoglobinopathies comes from studies on patients with sickle cell disease (SCD) [22]. The application of PET in SCD subjects was first published in 1988 in a preliminary study on six adults who had no history of neurological events but were found to have significant glucose hypometabolism in the frontal areas of the brain [23]. Our finding that MRI and PET-CT reveal different types of silent brain pathology (thus the low concordance rate) is in agreement with a similar study on patients with SCD [24]. Among 30 patients with no evidence of neurological dysfunction, 13 (43%) patients were found to have silent brain infarcts on MRI. PET identified 12 additional subjects, with normal MRI, to have silent brain abnormality (total = 83%). Two valid questions are (1) why would PET-CT fail to reveal silent brain infarcts detected on MRI and (2) can patients with decreased neuronal function on PET-CT have normal MRI? First, in the aforementioned study on patients with SCD [24], the concordance rate between abnormal PET and MRI scans was 80% for MRI-identified gray matter lesions, dropping to ~50% for white matter lesions [24]. These observations may be partly attributed to the naturally low glucose utilization in the white matter and could explain the low concordance for silent stroke detection between both imaging modalities, especially in our study where all silent MRI lesions were detected in the white matter. Thus, PET imaging cannot replace MRI to identify white matter lesions in the watershed areas [25–28]. Second, the areas of functional abnormality are usually greater than the structural neuronal loss defined by MRI or CT; thus, PET-CT abnormality can be detected with a normal MRI [29]. Moreover, there was a low concordance rate for the location of abnormality between both imaging techniques. Silent infarcts on MRI were bilateral and most commonly involved the frontal and parietal lobes, whereas neuronal dysfunction evident on PET-CT was mainly left sided, involving the parietal and temporal lobes. Although this may be attributed to the aforementioned difference in the type of brain pathology revealed by the two imaging modalities, it still warrants further discussion. The diffuse nature of silent infarcts on brain MRI in our study and their high prevalence in the frontal and parietal white matter is in total agreement with studies on SCD patients [30, 31]. In SCD patients, it was shown that the geographic distribution of the involved small penetrating arteries in the brain is derived from the carotid rather than the vertebrobasilar circulation, as a result of several anatomic and hemodynamic factors [32]. However, PET-CT abnormalities in this study were mostly detected in the temporal and/or parietal lobes. Temporoparietal hypometabolism on 18F-FDG PET is indeed the classic metabolic abnormality associated with Alzheimer's neuronal dysfunction [33], which has been associated with selective iron accumulation and oxidative damage [34, 35]. Whether a similar mechanism applies in patients with TI warrants further pathological investigation. However, the finding that PET-CT abnormalities in patients with TI are mainly confined to the dominant, left hemisphere (all patients in this report were right-handed) is difficult to interpret using the available evidence. Nevertheless, it may still be attributed to chance, considering the small sample size in this study.
The main limitation of our study is the lack of neurocognitive testing. Despite the terminology, “silent infarcts” observed on brain MRI are clinically significant given their association with subsequent overt stroke and neurocognitive deficits, as evident from studies in children and adults with SCD [30, 36–41]. Decreased neuronal function on PET scanning in patients with SCD is also associated with an intelligence quotient lower than the normal mean [24, 28] and a broader region of cerebral dysfunction that may be a prelude to clinical stroke [42, 43]. Whether such correlations exist in patients with TI merits evaluation.
In conclusion, our study demonstrated that decreased neuronal function evident on PET-CT is common in patients with TI, especially those characterized by elevated LIC. Moreover, it seems that the combined use of PET-CT and MRI could better identify splenectomized TI adults at high risk for stroke or functional neurologic deficits by highlighting the extent of physiologic dysfunction alongside the anatomic loss of neuronal tissue. However, larger studies are needed to confirm these findings before recommendations for screening can be made and to avoid unnecessary radiation exposure. More importantly, the exact mechanisms behind these abnormalities should be understood and their correlation with neurocognitive and long-term sequelae should be prospectively examined, thus allowing for optimal risk classification and timely preventive intervention.
References
Taher AT, Musallam KM, Cappellini MD, Weatherall DJ (2011) Optimal management of β thalassaemia intermedia. Br J Haematol 152:512–523
Steinberg MH, Forget BG, Higgs DR, Weatherall DJ (2009) Disorders of hemoglobin: genetics pathophysiology, and clinical management, 2nd edn. Cambridge University Press, Cambridge
Cappellini MD, Motta I, Musallam KM, Taher AT (2010) Redefining thalassemia as a hypercoagulable state. Ann N Y Acad Sci 1202:231–236
Taher AT, Musallam KM, El-Beshlawy A, Karimi M, Daar S, Belhoul K, Saned MS, Graziadei G, Cappellini MD (2010) Age-related complications in treatment-naive patients with thalassaemia intermedia. Br J Haematol 150:486–489
Taher AT, Musallam KM, Karimi M, El-Beshlawy A, Belhoul K, Daar S, Saned MS, El-Chafic AH, Fasulo MR, Cappellini MD (2010) Overview on practices in thalassemia intermedia management aiming for lowering complication rates across a region of endemicity: the OPTIMAL CARE study. Blood 115:1886–1892
Taher A, Isma'eel H, Mehio G, Bignamini D, Kattamis A, Rachmilewitz EA, Cappellini MD (2006) Prevalence of thromboembolic events among 8,860 patients with thalassaemia major and intermedia in the Mediterranean area and Iran. Thromb Haemost 96:488–491
Cappellini MD, Robbiolo L, Bottasso BM, Coppola R, Fiorelli G, Mannucci AP (2000) Venous thromboembolism and hypercoagulability in splenectomized patients with thalassaemia intermedia. Br J Haematol 111:467–473
Taher AT, Musallam KM, Karimi M, El-Beshlawy A, Belhoul K, Daar S, Saned M, Cesaretti C, Cappellini MD (2010) Splenectomy and thrombosis: the case of thalassemia intermedia. J Thromb Haemost 8:2152–2158
Atichartakarn V, Angchaisuksiri P, Aryurachai K, Onpun S, Chuncharunee S, Thakkinstian A, Atamasirikul K (2002) Relationship between hypercoagulable state and erythrocyte phosphatidylserine exposure in splenectomized haemoglobin E/beta-thalassaemic patients. Br J Haematol 118:893–898
Rund D, Rachmilewitz E (2005) Beta-thalassemia. N Engl J Med 353:1135–1146
Manfre L, Giarratano E, Maggio A, Banco A, Vaccaro G, Lagalla R (1999) MR imaging of the brain: findings in asymptomatic patients with thalassemia intermedia and sickle cell-thalassemia disease. AJR Am J Roentgenol 173:1477–1480
Taher AT, Musallam KM, Nasreddine W, Hourani R, Inati A, Beydoun A (2010) Asymptomatic brain magnetic resonance imaging abnormalities in splenectomized adults with thalassemia intermedia. J Thromb Haemost 8:54–59
Camaschella C, Cappellini MD (1995) Thalassemia intermedia. Haematologica 80:58–68
St Pierre TG, Clark PR, Chua-anusorn W, Fleming AJ, Jeffrey GP, Olynyk JK, Pootrakul P, Robins E, Lindeman R (2005) Noninvasive measurement and imaging of liver iron concentrations using proton magnetic resonance. Blood 105:855–861
Afifi AA, Clark V, May S (2004) Computer-aided multivariate analysis, 4th edn. Chapman & Hall/CRC, New York, p 489
Taher A, Hershko C, Cappellini MD (2009) Iron overload in thalassaemia intermedia: reassessment of iron chelation strategies. Br J Haematol 147:634–640
Taher A, El Rassi F, Isma'eel H, Koussa S, Inati A, Cappellini MD (2008) Correlation of liver iron concentration determined by R2 magnetic resonance imaging with serum ferritin in patients with thalassemia intermedia. Haematologica 93:1584–1586
Roghi A, Cappellini MD, Wood JC, Musallam KM, Patrizia P, Fasulo MR, Cesaretti C, Taher AT (2010) Absence of cardiac siderosis despite hepatic iron overload in Italian patients with thalassemia intermedia: an MRI T2* study. Ann Hematol 89:585–589
Taher AT, Musallam KM, Wood JC, Cappellini MD (2010) Magnetic resonance evaluation of hepatic and myocardial iron deposition in transfusion-independent thalassemia intermedia compared to regularly transfused thalassemia major patients. Am J Hematol 85:288–290
Origa R, Barella S, Argiolas GM, Bina P, Agus A, Galanello R (2008) No evidence of cardiac iron in 20 never- or minimally-transfused patients with thalassemia intermedia. Haematologica 93:1095–1096
Li X, Jankovic J, Le W (2011) Iron chelation and neuroprotection in neurodegenerative diseases. J Neural Transm 118:473–477
Verduzco LA, Nathan DG (2009) Sickle cell disease and stroke. Blood 114:5117–5125
Rodgers GP, Clark CM, Larson SM, Rapoport SI, Nienhuis AW, Schechter AN (1988) Brain glucose metabolism in neurologically normal patients with sickle cell disease. Regional alterations. Arch Neurol 45:78–82
Powars DR, Conti PS, Wong WY, Groncy P, Hyman C, Smith E, Ewing N, Keenan RN, Zee CS, Harold Y, Hiti AL, Teng EL, Chan LS (1999) Cerebral vasculopathy in sickle cell anemia: diagnostic contribution of positron emission tomography. Blood 93:71–79
Herold S, Brozovic M, Gibbs J, Lammertsma AA, Leenders KL, Carr D, Fleming JS, Jones T (1986) Measurement of regional cerebral blood flow, blood volume and oxygen metabolism in patients with sickle cell disease using positron emission tomography. Stroke 17:692–698
Labbe C, Froment JC, Kennedy A, Ashburner J, Cinotti L (1996) Positron emission tomography metabolic data corrected for cortical atrophy using magnetic resonance imaging. Alzheimer Dis Assoc Disord 10:141–170
Mehta RC, Marks MP (1992) Physiologic imaging of the brain. Curr Opin Radiol 4:95–100
Reed W, Jagust W, Al-Mateen M, Vichinsky E (1999) Role of positron emission tomography in determining the extent of CNS ischemia in patients with sickle cell disease. Am J Hematol 60:268–272
Gross H, Kling A, Henry G, Herndon C, Lavretsky H (1996) Local cerebral glucose metabolism in patients with long-term behavioral and cognitive deficits following mild traumatic brain injury. J Neuropsychiatry Clin Neurosci 8:324–334
Pegelow CH, Macklin EA, Moser FG, Wang WC, Bello JA, Miller ST, Vichinsky EP, DeBaun MR, Guarini L, Zimmerman RA, Younkin DP, Gallagher DM, Kinney TR (2002) Longitudinal changes in brain magnetic resonance imaging findings in children with sickle cell disease. Blood 99:3014–3018
Pegelow CH, Wang W, Granger S, Hsu LL, Vichinsky E, Moser FG, Bello J, Zimmerman RA, Adams RJ, Brambilla D (2001) Silent infarcts in children with sickle cell anemia and abnormal cerebral artery velocity. Arch Neurol 58:2017–2021
Switzer JA, Hess DC, Nichols FT, Adams RJ (2006) Pathophysiology and treatment of stroke in sickle-cell disease: present and future. Lancet Neurol 5:501–512
Hoffman JM, Welsh-Bohmer KA, Hanson M, Crain B, Hulette C, Earl N, Coleman RE (2000) FDG PET imaging in patients with pathologically verified dementia. J Nucl Med 41:1920–1928
Smith MA, Harris PL, Sayre LM, Perry G (1997) Iron accumulation in Alzheimer disease is a source of redox-generated free radicals. Proc Natl Acad Sci USA 94:9866–9868
Good PF, Perl DP, Bierer LM, Schmeidler J (1992) Selective accumulation of aluminum and iron in the neurofibrillary tangles of Alzheimer's disease: a laser microprobe (LAMMA) study. Ann Neurol 31:286–292
Miller ST, Macklin EA, Pegelow CH, Kinney TR, Sleeper LA, Bello JA, DeWitt LD, Gallagher DM, Guarini L, Moser FG, Ohene-Frempong K, Sanchez N, Vichinsky EP, Wang WC, Wethers DL, Younkin DP, Zimmerman RA, DeBaun MR (2001) Silent infarction as a risk factor for overt stroke in children with sickle cell anemia: a report from the Cooperative Study of Sickle Cell Disease. J Pediatr 139:385–390
Wang W, Enos L, Gallagher D, Thompson R, Guarini L, Vichinsky E, Wright E, Zimmerman R, Armstrong FD (2001) Neuropsychologic performance in school-aged children with sickle cell disease: a report from the Cooperative Study of Sickle Cell Disease. J Pediatr 139:391–397
Armstrong FD, Thompson RJ Jr, Wang W, Zimmerman R, Pegelow CH, Miller S, Moser F, Bello J, Hurtig A, Vass K (1996) Cognitive functioning and brain magnetic resonance imaging in children with sickle cell disease. Neuropsychology Committee of the Cooperative Study of Sickle Cell Disease. Pediatrics 97:864–870
Bernaudin F, Verlhac S, Freard F, Roudot-Thoraval F, Benkerrou M, Thuret I, Mardini R, Vannier JP, Ploix E, Romero M, Casse-Perrot C, Helly M, Gillard E, Sebag G, Kchouk H, Pracros JP, Finck B, Dacher JN, Ickowicz V, Raybaud C, Poncet M, Lesprit E, Reinert PH, Brugieres P (2000) Multicenter prospective study of children with sickle cell disease: radiographic and psychometric correlation. J Child Neurol 15:333–343
Kugler S, Anderson B, Cross D, Sharif Z, Sano M, Haggerty R, Prohovnik I, Hurlet-Jensen A, Hilal S, Mohr JP et al (1993) Abnormal cranial magnetic resonance imaging scans in sickle-cell disease. Neurological correlates and clinical implications. Arch Neurol 50:629–635
Vichinsky EP, Neumayr LD, Gold JI, Weiner MW, Rule RR, Truran D, Kasten J, Eggleston B, Kesler K, McMahon L, Orringer EP, Harrington T, Kalinyak K, De Castro LM, Kutlar A, Rutherford CJ, Johnson C, Bessman JD, Jordan LB, Armstrong FD (2010) Neuropsychological dysfunction and neuroimaging abnormalities in neurologically intact adults with sickle cell anemia. JAMA 303:1823–1831
De Reuck J, Leys D, De Keyser J (1997) Is positron emission tomography useful in stroke? Acta Neurol Belg 97:168–171
Arkuszewski M, Melhem ER, Krejza J (2010) Neuroimaging in assessment of risk of stroke in children with sickle cell disease. Adv Med Sci 55:115–129
Funding source
This study was supported by an unrestricted grant from Novartis Pharmaceuticals.
Conflicts of interest
ATT is a member of Novartis Speakers' Bureau.
Author information
Authors and Affiliations
Corresponding author
Additional information
Khaled M. Musallam and Wassim Nasreddine contributed equally as first authors.
Rights and permissions
About this article
Cite this article
Musallam, K.M., Nasreddine, W., Beydoun, A. et al. Brain positron emission tomography in splenectomized adults with β-thalassemia intermedia: uncovering yet another covert abnormality. Ann Hematol 91, 235–241 (2012). https://doi.org/10.1007/s00277-011-1291-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-011-1291-3