
Abstract
The presence and description of anatomical findings about the foramen of Vesalius (FV) is important in the surgical procedure on the trigeminal nerve and/or trigeminal ganglion. This is an evaluation area for percutaneous techniques. A morphological analysis of the FVs was made in a total of 344 sides of the basis cranii of adult skulls by computerized photogrammetry using standardized digital photographs. The FV was identified in 60 specimens (34.8 %). The FV was observed to be present bilaterally in 16 specimens (9.3 %). The incidence of unilateral FV was 25.5 % of the skulls, of which in 26 specimens (15.1 %) it occurred on the left side, and in 18 specimens (10.4 %) on the right side. The FV was observed to present a double opening in two specimens. The diameters of the FV were found to be 0.86 ± 0.21 (right) and 1.07 ± 0.37 mm (left). The incidence of openings with a diameter of FV 0.5 mm or more was found to be 45 %. The area of the FV was calculated as 1.09 ± 0.51, and 1.4 ± 0.83 mm2 on the right and the left, respectively. The mean distances of FV to the foramen ovale were measured as 2.30 ± 1.14 mm (right) and 2.46 ± 0.89 mm (left). The mean distances of FV to foramen spinosum were found to be 10.76 ± 1.26 mm (right) and 10.42 ± 1.29 mm (left). The findings suggest that the diameter of FV as <0.5 mm was safer to work with, while the opening types bigger than 0.5 mm opening types were highly risky for percutaneous techniques on the foramen ovale. In our study, a clear standardization has been achieved. The findings were the data obtained through computer-assisted three dimensional landmarks, appropriate for use in three dimensional planning.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The motor portion of the third division of the trigeminal nerve is situated in front of the sensory root, and runs under the trigeminal ganglia in the direction of the foramen ovale (FO) [2, 23]. The ‘Foramen of Vesalius’, or shortly the ‘foramen Vesalius’ (FV) is sphenoidal emissary foramen found between the FO and the foramen spinosum (FS) [8]. The FV allows the extracranial passage of the plexuses, which enables brain drainage [4, 14, 30]. It connects the pterygoid plexus with the cavernous sinus, and transmits a small emissary vein, which drains the cavernous sinus [15, 26]. Bergman et al. [3] reported that the FV might even transmit the accessory meningeal artery.
The FV has a closed relationship with middle cranial openings such as FO, foramen rotundum (FR), foramen lacerum (FL) and carotid canal (CC) [8, 17, 25]. The FV, if present, is generally situated posteromedially from the FR, and anteromedially from the FO, FS and FR. The FV may alter the operating techniques in interventions to be carried out on FO, because every skull may have an opening, or that it may be very close to FO [1, 11, 24]. In order to treat trigeminal neuralgia through percutaneous techniques such as ablation, glycerol injection, ballon compression and neuronavigation techniques such as microelectrodes, there is a need for detailed knowledge near the FO [1, 18, 19]. Although the transovale approach for percutaneous trigeminal rhizotomy is widely used in neurosurgical practice, various complications, although rare, such as cerebrospinal fluid leakage, carotidocavernous fistulas, intracranial hemorrhages, cranial nerve injuries, and even death, were reported after this approach [12, 20, 21, 24].
The FV has a wide variation reported by several studies [2–4, 8, 11, 15, 17, 19]. As few studies have examined the arrangements of the FVs and their close relationship with the middle cranial foramens detail, our team has studied the arrangements of the FVs of the middle cranial fossa [1, 26, 29]. The presence of the FV may negatively affect the success of the intervention [1, 27–29]. Particularly in the interventional operations, the direction, the angle and the position of the procedure may change according to the presence of the FV and the difference in the measurements may alter the surgical technique [26–28]. In an intervention, the presence of the FV, which is an opening close to the important anatomical structures such as FO, FS, FL or CC, may lead to an entry into the wrong opening, complications or intracranial bleeding [1, 13, 16].
Moreover, morphometry of the FV is important while percutaneously safer accessing the trigeminal ganglion and the nerve. The goal of our study was to measure the proximity of the FV to the cavity structures and the other important cavities in its nearest neighborhood using computerized photogrammetry.
Materials and methods
One hundred and seventy-two sphenoidal bones in the basis cranii, in total 344 sides of adult dry skulls in total of unknown age and sex obtained from the collections at the Department of Anatomy, Faculty of Medicine, Ege University were used to measure the dimensions and determine the localization of the FV. The macro mode of Sony DSC H1 5.1 megapixel camera was used for photography. The photographs were taken in aperture priority mode, with f 3.5 diaphragm clarity and at 4 zoom adjustment. The skulls were fixed horizontally. The shots were made by fixing the camera 37.5 cm away from the FV with the help of a tripod at an angle of 78º with the horizontal surface.
The pictures were then uploaded onto a personal computer, and a specific software (Able Software Corporation 3D-Doctor V 3.5.050402 Demo version for Windows 98/NT/2000) http://www.ablesw.com/3d-doctor/support.html was used (Fig. 1). With the software, inferior contours of the FVs were manually chosen, and their perimeter and relations with the other structures (FO, CC, FL and FS) were evaluated on the right and left sides separately in the same photos (Figs. 2, 3) (Mehmet Asim Ozer). Differences between the data of skull measurements (mean, minimum, maximum, standard deviation) were analyzed by the Student t test (Table 1). The Pearson correlation test was used in the statistical analysis which was made from the values of 17 parameters such as the diameter and the distance FV–FO; the diameter and the distance FV–FS; the diameter and the distance FV–CC; the distance FV–FO and the distance FV–FS; the distance FV–FO and the distance FV–CC; the distance FV–FS and the distance FV–CC (Table 2). For all the analyses, p < 0.05 was accepted as statistically significant, while p < 0.01 was accepted as highly significant.

Perimeter measurement of the FV using Able Software Corporation 3D-Doctor V 3.5050402 Demo version. FO foramen ovale, FV foramen of Vesalius, FS foramen spinosum, T top, R right

Calculation of some of the measurements and related structures made of the FV using the V 3.5050402 Demo version. FO foramen ovale, FS foramen spinosum, CC canalis caroticus, FV foramen of Vesalius, FL foramen lacerum, T top, L left

Types of foramen of Vesalius (FV). a Type 1: diameter of FV < 0.5 mm, b type 2: diameter between 0.5 and 1 mm, c type 3: diameter over 1 mm. FO foramen ovale, FM foramen magnum, T top, L left
The study was approved by a suitably constituted ethics committee of the institution within which the work was undertaken, and the study conforms to the previous of the Declaration of Helsinki in 1964.
Result
In 344 specimens, no differences were observed in the structure of the openings between FO, FS and FR. In these specimens, posterolateral to the FR was the FO. Slightly dorsolateral to the FO was a 4–8 mm long bony channel, the FS. Medial to the FO, and usually slightly dorsal to it was an irregular bone gap, referred to as the FL because of its shape. The FL was an irregular gap bounded in front by the body, and the adjoining roots of the pterygoid process and the greater wing of the sphenoid bone. In most cases, CC was in most cases oval; its long axis indicated a mediorostral to laterodorsal orientation.
The FV was located in the greater wing of the sphenoid bone between the FO and the FR (Figs. 1, 2, 3, 4). It was an elliptical opening, and its long axes were directed forward and medially. The FV was found medial to FO which ran to an oblique pathway directed towards the fossa pterygoidea. This pathway opened near the root of the pterygoid process.

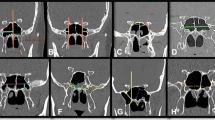
Different types of foramen of Vesalius (FV). a The absence of bilateral opening, b the presence of left-sided opening, c right-sided opening, d bilateral large openings, e a double opening on the left side and a small one on the right side. FO foramen ovale, T top; L left
In the 172 basis cranii analyzed, FV was identified in 60 specimens (34.8 %) (Figs. 3, 4a–e). The FV was observed to be present bilaterally in 16 specimens (9.3 %) (Fig. 4d). The incidence of the unilateral foramen was 25.5 % of the skulls, of which in 26 specimens (15.1 %), it was on the left side (Figs. 3, 4b), and in 18 specimens (10.4 %) on the right side (Fig. 4c). The FV was observed to present a double opening in two specimens (Fig. 4e).
The diameter of the long axis FV was found to be 0.86 ± 0.21 (right) and 1.07 ± 0.37 mm (left), respectively. When the FV was categorized according to the diameter of the opening, type 1 specimens had a diameter of FV less than 0.5 mm, type 2 specimens had diameters between 0.5 and 1 mm, whilst type 3 specimens had diameters greater than 1 mm. In five specimens (four right side, one left side), the diameter was found to be less than 0.5 mm (Fig. 3a). The incidence of type 1 was 8.3 %. In 11 specimens, its diameter was calculated to be more than 1 mm (Fig. 3c). The incidence of type 3 was 18.3 %. The circumference of the FV was found to be 2.43 ± 0.52 and 2.74 ± 0.97 mm on the right and left, respectively. The area of the FV was measured as 1.09 ± 0.51, and 1.4 ± 0.83 mm² on the right and left, respectively.
The mean distances of the FV to the FO were measured as 2.30 ± 1.14 mm (right), and 2.46 ± 0.89 mm (left), respectively. The mean distances of the FV to the FS were found as 10.76 ± 1.26 mm (right), and 10.42 ± 1.29 mm (left), respectively. The mean distances of the FV to the FL were found as 5.40 ± 1.53 mm (right), and 5.42 ± 1.71 mm (left), respectively. The findings of these measurements are shown in Table 1.
In the Pearson correlation analysis, it was also significant that a statistical meaningfulness on the relationship was found between the perimeter and the distance FV–FS; the distance FV–FO and the distance FV–FS left side. Their correlations were significant at the 0.05 level (Table 2).
Discussion
The sphenoid bone presents multiple foramina which permits the extracranial passage of the nerves and venous plexus, which allows brain drainage. The basal foramina of the middle cranial fossa such as FO, FR, FL, CC and FV are named as basal portals [6, 14]. Important arteries, veins and neural structures move through each hole [6, 30]. The mandibular nerve and a venous plexus (plexus venosus foraminis ovalis) pass through the FO to the infratemporal fossa. A sphenoid emissary vein passes through the FV [4, 14]. It is important to reach the FO trigeminal nerve and ganglion in the case of trigeminal neuralgia. Most of the percutaneous approaches to the trigeminal nerve necessitate morphometrical analysis of the FO and the related structures [4, 15, 20].
Trigeminal neuralgia is the most frequent occurence of the craniofacial neuralgias. For patients in whom medical treatment fails to control pain, microvascular decompression, glycerol rhizolysis, radiofrequency thermocoagulation and percutaneous trigeminal microdecompression procedures have been devised in infratemporal fossa [27, 28]. Repeated skull X-rays, stereotaxic techniques and navigation systems such as computed tomography-guided techniques have all been recommended to minimize the complication rate due to the blind path or incorrect trajectors during percutaneous approaches through the FO [1, 9, 29]. During these insertions, many punctures are made, and the needle can be accidentally inserted into the inferior orbital fissure, in the lacerated foramen, in the jugular foramen, in the CC, and in the FV [1, 26]. Carotidocavernous fistula due to internal carotid artery rupture temporary or persistent pareses of the cranial nerves, cerebrospinal fluid fistula and intracranial hemorrhages are well-known complications of trigeminal rhizotomy [1, 10, 12, 13].
Despite the fact that the variation in the middle cranial foramens as well as the measurements and the incidence have been recognized in previous clinical and anatomical studies, it has been observed during the treatment of trigeminal neuralgia that the presence of the FV was not as low as it had been reported by many authors [2, 15, 17, 19, 21, 23, 27]. Moreover, the FV is important from the surgical point of view, because during percutaneous trigeminal rhizotomy, the needle insertion through the FV may cause cavernous sinus puncture [18].
Incidence
Most researchers have reported the incidence of the FV in values which can vary greatly (8.5 to 100 %). The presence of the FV was reported in 8.5 % of the skulls Williams et al. [30], Chaisuksunt et al. [5] in 16.1 %, by Wysocki et al. [31] in 17 %, Kodama et al. [17] in 21.75 %, Reymond [23] in 22 %, Gupta et al. [8] in 32.9 %, Shinohara et al. [26] in 33.8 %, Boyd [4] in 36.5 %, Berge et al. [2] in 40 %, Kale et al. [11] in 45 %, Ramalho et al. [22] in 71.87 % and Kaplan et al. [13] in 100 %. In our study, the incidence was recorded as 34.8 %.
The knowledge about the features such as the incidence and the size can provide important anatomical features and significant clinical data [1, 8, 23, 26, 29]. The FV is reported as a hole located anteriorly and medially to the FO, to the FS and to the CC. In this study, the FO was found to be anteromedial with the FV.
Opening side
Researchers found the incidence of the unilateral patent in values 5.5 to 80 %. According to the previous reports, the frequency of the unilateral opening FV might be as 5.5 % of the skulls (Kodama et al. [17]), 11.9 % (Chaisuksunt et al. [5]), 18.3 % (Shinohara et al. [26], 19.9 % (Kale et al. [11]), 20 % (Gupta et al. [8]), and 80 % (Ginsberg et. al. [7]). Previous researchers have reported the incidence of the bilateral foramina in values greatly varying from 12.5 to 66 %. The incidence rate for bilateral presence was 12.5 % for Boyd [4], 15.5 % for Shinohara et al. [26], 22 % for both Kodama et al. [17] and Gupta et al. [8], 35 % for Berge and Bergman [2]. According to most researchers, the FV is usually observed in one side, which conflicts with our results. Based on our findings, we reported that the incidence of the unilateral FV (25.5 %) is greater than bilateral foramen (9.3 %) in individual skulls.
Diameter
Even though the incidence of the FV has been given in many studies, in fact, the diameter measurements of these openings is more important. Furthermore, the number of the openings having a diameter suitable for a percutaneous needle to pass through is of importance. In the majority of the previous studies, this detail was ignored, while only the incidence of the opening was evaluated [4, 8]. According to Kodama et al., the FV is classified as the open type, and the closed type [17]. Shinohara et al. reported that the average diameter of FV was 0.69 mm (range 0.24–1.6 mm) on the right, while on the left side, the value was 0.72 mm (range 0.08–2.06 mm) [26]. The diameters of the long axis FV were found to be 0.86 ± 0.21 (right) and 1.07 ± 0.37 mm (left), in this study.
There is indeed a good deal of data concerning the diameter measurements. While several authors stated that they measured the diameter of the hole by caliper or metric, the others did not give any detailed information with respect to the method of measurement. It is a fact that some standardization errors were made in the measurement procedures of previously carried out studies. The high rate of the incidence of the opening does not mean that there is a high rate of failure during interventions due to the percutaneous needle erroneously entering the FV because the needles used in the trigeminal rhizotomy have a diameter between 0.7 and 1.27 mm [9, 21, 24].
In this study, we found many FV-like structures from which the acupuncture needles could not pass, and we did not evaluate them as the FV. In our study in which a reliable method whose margin of error is lower, a clear standardization has been achieved. The findings were obtained through computer-assisted three-dimensional landmarks, appropriate for use in digital photogrammetry.
In this study, digital photometric methods were used to collect linear, area and perimeter data of FV. The process of measuring photographs (photogrammetry) has been routinely in odontological studies for several decades, and is being employed in bioarchaeological and forensic investigations concerning other anatomical structures as well. Digital photogrammetry is a photogrammetry method applied to digital images instead of hard copies; all the studies are accomplished on digital data. Photogrammetry has several advantages over conventional measurements methods [6]. Another advantage of digital photogrammetry is the opportunity to preserve the material, which allows to repeat the measurements anytime, and to add new parameters in subsequent measurements [6]. After getting the digital images, they can be edited in image processing programs such as Photoshop to obtain any standard parameter desired. The measurements may be performed using digital image processing and analysis softwares like Image J, which is one of the most preferred processing and analysis, provided by National Institute of Health, available at http://rsb.info.nih.gov.ij. The most important point in measurements is to set a proper and visible scale for each size, the scale can be set using this bar. Success of photogrammetry depends on uniform lighting conditions, placement of feature positions close to their actual positions in images, and providing accurate scales on the images [6].
This fact constitutes one of the complications that result from the trigeminal rhizotomy, as the puncture of the FV diameter should be bigger than 0.7 or 0.5 mm. In our study the incidence of risky FV openings with a diameter of 0.5 and 1 mm or more (types 2 and 3), categorization according to their diameters was found to be 45 % in total (Fig. 3c). This is a high proportion. In 11 specimens, the diameter was calculated to be more than 1 mm. The incidence of type 3 was 18.3 %.
Measurement
The proximity of FV to the holes in the skull base has a clinical importance. In this research, these distances were measured on both sides as the distance between the FV and the FO, the distance between the FV and the FS, and the distance between the FV and the CC. The average distance between the FV and the FO was 2.30 mm on the right side and 2.46 mm on the left side. The average distance between the FV and FS was 10.76 mm on the right side and 10.42 mm on the left side. The distance between the FV and the CC was found to have an average value of 17.03 mm on the right side, and 17.03 mm on the left side. Kaplan et al. [13] showed the FV with a distance of 4 mm (range 3-5 mm) anteromedial to the FO. In the study by Shinohara et al., this measurement was much greater than ours, as they found 7 mm on the right and 6 mm on the left side [26].
With the presence of the FV, the familiar distances between the FO–CC and the FV–FS can change. In the types where the diameter of FV is large and in double openings, the trigeminal nerve intervention areas will be narrowed, and the intervention will require more caution.
The diameters of the FVs were categorized. The width of the diameter of the opening and the probability of the needle being faultily inserted into the opening were evaluated. In the procedures, the FV specimens with a diameter smaller than 0.5 mm are the ones with the smallest area, and therefore, the highest surgical success (Fig. 3a). The diameter types of FV including type 2 (Fig. 3b) and type 3 (Fig. 3c), where the percutaneous approach surface is quite narrow might cause problems in terms of orientation, as the surgical resonance area is narrow and the length is short. The quite high-frequency rate of these types (18.3 %) is in fact unfavorable. Information as the size, the occurrence, the incidence and the asymmetry can provide familiarity with important anatomical features, and can show variations which may be clinically significant.
The confluence of the FO with the foramen of Vesalius is reported in the literature [2, 4, 8, 15, 17, 19]. The presence of the FV reduces the area of safety in the bone during interventions, and reduces the chances of success. Kodama et al. [17] described the use of three-dimensional CT to guide the approach to the FO to block the mandibular nerve. The advantages of the neuronavigation systems consist of real-time instrument guidance, increased accuracy of target localization, and three-dimensional planning ability [1]. Anatomical studies of the FV on using stereotactic techniques give rise to cannulation success [9, 27], decrease the complications [8], and reduce pain recurrence after radiofrequency trigeminal rhizotomy [12, 20, 28, 29].
Finally, we can infer that the information provided in the course of time presents study that can help surgeons and researchers to increase their knowledge of anatomy in the middle cranial fossa.
References
Alvernia JE, Sindou MP, Dang ND, Maley HJ, Mertens P (2010) Percutaneous approach to the foramen ovale: an anatomical study of the extracranial trajectory with the incorrect trajectories to be avoided. Acta Neurochir 152:1043–1053
Berge JK, Bergman RA (2001) Variations in size and in symmetry of foramina of the human skull. Clin Anat 14(6):406–413
Bergman RA (2011) Thoughts on human variations. Clin Anat 24(8):938–940
Boyd GI (1930) Emissary foramina of cranium in man and the anthropoids. J Anat 65:108–121
Chaisuksunt V, Kwathai L, Namonta K, Rungruang T, Apinhasmit W, Choompoopong S (2012) Occurrence of the foramen Vesalius and its morphometry relevant to clinical consideration. Sci World J 817454. doi:10.1100/2012/817454
Douglas TS (2004) Image processing for craniofacial landmark identification and measurement: a review of photogrammetry and cephalometry. Comp Med Imaging Graph 28:401–409
Ginsberg LE, Pruett SW, Chen MY, Elster AD (1994) Skull base foramina of the middle cranial fossa: reassessment of normal variation with high-resolution CT. Am J Neuroradiol 15(2):283–291
Gupta N, Ray B, Ghosh S (2005) Anatomic characteristics of foramen Vesalius. Kathmandu Univ Med J 3(2):155–158
Hinteregger M, Zschiegner F, Lirk P, Ladner E, Goeschl A, Gaber O, Moser P, Lorenz I, Kolbitsch C (2004) A new guidance device facilitates percutaneous puncture of the foramen ovale in human cadavers. Can J Anaesth 51(10):990–992
James TM, Presley R, Steel FL (1980) The foramen ovale and sphenoidal angle in man. Anat Embryol (Berl) 160:93–104
Kale A, Aksu F, Ozturk A, Gurses AI, Gayretli O, Zeybek FG, Bayraktar B, Ari Z, Onder N (2009) Foramen of Vesalius. Saudi Med J 30(1):56–59
Kanpolat Y, Savas A, Bekar A, Berk C (2001) Percutaneous controlled radiofrequency trigeminal rhizotomy for the treatment of idiopathic trigeminal neuralgia: 25 year experience with 1,600 patients. Neurosurgery 48(3):524–532
Kaplan M, Erol FS, Ozveren MF, Topsakal C, Sam B, Tekdemir I (2007) Review of complications due to foramen ovale puncture. J Clin Neurosci 14(6):563–568
Keskil S, Gozil R, Calguner E (2003) Common surgical pitfalls in the skull. Surg Neurol 59(3):228–231
Kim DI, Kim HS (1995) High resolution CT evaluation on the morphologic characteristics and variations of foramen ovale and adjacent foramina in the skull base. J Kor Radiol Soc 33(1):43–48
Kocaogullar Y, Avci E, Fossett D, Caputy A (2003) The extradural subtemporal keyhole approach to the sphenocavernous region: anatomic considerations. Minim Invas Neurosurg 46(2):100–105
Kodama K, Inoue K, Nagashima M, Matsumura G, Watanabe S, Kodama G (1997) Studies on the foramen Vesalius in the Japanese juvenile and adult skulls. Hokkaido Igaku Zasshi 72(6):667–674
Kuether TA, O’Neill OR, Nesbit GM, Barnwell SL (1996) Direct carotid cavernous fistula after trigeminal balloon microcompression gangliolysis: case report. Neurosurgery 39(4):853-855 (discussion 855–856)
Lanzieri CF, Duchesneau PM, Rosenbloom SA, Smith AS, Rosenbaum AE (1988) The significance of asymmetry of the foramen of Vesalius. Am J Neuroradiol 9(6):1201–1204
Liu M, Wu CY, Liu YG, Wang HW, Meng FG (2005) Three-dimensional computed tomography-guided radiofrequency trigeminal rhizotomy for treatment of idiopathic trigeminal neuralgia. Chin Med Sci J 20(3):206–209
Lunsford LD, Niranjan A, Kondziolka D (2007) Surgical management options for trigeminal neuralgia. J Kor Neurosurg Soc 41:359–366
Ramalho AJC, Sousa-Rodriguez CF, Rodas PMM, Lins CJP, De Lima RL, Almeida ETDL, Neto JABS (2007) A incidência e as relações morfométricas do forame emissário do esfenóide em crânios humanos. Int J Morphol 25(1):147
Reymond J, Charuta A, Wysocki J (2005) The morphology and morphometry of the foramina of the greater wing of the human sphenoid bone. Folia Morphol (Warsz) 64(3):188–193
Sekimoto K, Koizuka S, Saito S, Goto F (2005) Thermogangliolysis of Gasserian ganglion under computed tomography fluoroscopy. J Anesth 19(2):177–179
Shapiro R, Robinson F (1967) The foramina of the middle fossa: a phylogenetic, anatomic and pathologic study. Am J Roentgenol 101:779–794
Shinohara AL, de Souza Melo CG, Silveira EM, Lauris JR, Andreo JC, de Castro Rodrigues A (2010) Incidence, morphology and morphometry of the foramen of Vesalius: complementary study for a safer planning and execution of the trigeminal rhizotomy technique. Surg Radiol Anat 32(2):159–164
Sindou M, Keravel Y, Abdennebi B, Szapiro J (1987) Neurosurgical treatment of trigeminal neuralgia. Direct approach or percutaneous method? Neurochirurgie 33(2):89–111
Sweet WH, Poletti CE (1988) Complications of percutaneous rhizotomy and microvascular decompression operations for facial pain. In: Schmideck HH, Sweet WH (eds) Operative neurosurgical techniques: indication, methods, and results. Grune and Straton, Orlando, pp 1139–1144
Tatli M, Sindou M (2008) Anatomoradiological landmarks for accuracy of frequency thermorhizotomy in the treatment of trigeminal neuralgia. Neurosurgery 63 (1Suppl 1):ONS129-37
Williams PL, Bannister LH, Martin MM et al (1995) Gray’s anatomy, 38th edn. Churchill Livingstone, London, pp 425–736
Wysocki J, Reymond J, Skarzynski H, Wrobel B (2006) The size of selected human skull foramina in relation to skull capacity. Folia Morphol 65(4):301–308
Conflict of interest
No financial conflict of interest exists with any commercial entity whose products are described, reviewed, evaluated or compared in the manuscript. None of the authors has a financial interest in any of the product, devices or drugs mentioned in this article. This article has not been submitted or published elsewhere in part or in whole and that it is original work.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ozer, M.A., Govsa, F. Measurement accuracy of foramen of vesalius for safe percutaneous techniques using computer-assisted three-dimensional landmarks. Surg Radiol Anat 36, 147–154 (2014). https://doi.org/10.1007/s00276-013-1148-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-013-1148-7