
Abstract
Purpose
The aim of our study was to determine guide parameters for clinicians by morphometric assessment of important landmarks on cranium intended for Vidian nerve surgery.
Methods
For the study, 23 half-skull bases, 40 skull bases and 40 skulls were obtained from the Department of Anatomy, Ege University Medicine Faculty. The vertical distances were measured using a digital caliper to the nearest 0.01 mm.
Results
The anterior opening of the Vidian canal (pterygoid canal) was observed as oval shaped on 57 specimens (31.1%), funnel shaped on 58 specimens (31.7%), round shaped on 64 specimens (35%) and septated on 4 specimens (2.2%). Vidian canal was embedded into the body of sphenoid on 55 specimens (52.4%) (embedded type) and protruded to sphenoidal sinus on 50 specimens (47.6%) (protruded type). 21 specimens of 50 were partial and 29 specimens were total. There were dehiscences on 21 specimens of 50 protruded type on the base of sphenoidal sinus (20%). Anterior opening of the Vidian canal was assessed according to medial lamina of pterygoid process. It was located medially in 169 of the specimens (92.3%) and laterally in 14 specimens (7.7%).
Conclusion
Vidian canal and Vidian nerve are deeply located structures on skull. Vidian canal and surrounding structures are important landmarks for microsurgery and endoscopic approaches to Vidian nerve. We consider that knowledge of anatomical features of Vidian canal and preoperative imaging by CT (computed tomography) will be supportive when choosing and planning a safe surgical approach.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vidius (1509–1569) was an Italian surgeon and anatomist. He performed important anatomic investigations. The Vidian nerve and canal in the skull were also identified by Vidius [2, 14, 18].
The Vidian nerve passing through the pterygoid canal is formed by the union of sympathetic and parasympathetic fibers separately derived from the greater petrosal branch of the facial nerve and the deep petrosal branch of sympathetic plexus of internal carotid artery. Thus the Vidian nerve is essentially secretomotor to the nasal mucosa and lacrimal gland. The length of the Vidian canal is about 10–18 mm. It also transmits the vessels [9, 12, 17].
The Vidian nerve surgery may be required in some cases like severe intractable secretomotor rhinopathy but relatively deep anatomical location of the nerve within the sphenoid bone access can be difficult [11]. The pterygopalatine fossa lies between the pterygoid process of the sphenoid bone posteriorly and posterior aspect of the maxilla anteriorly, inferior to the apex of the orbit [6].
The aim of our study was to determine guide parameters for clinicians by the morphometric assessments of important landmarks on cranium intended for Vidian nerve surgery.
Materials and methods
The materials used in this study consisted of 23 half-skull bases, 40 skull bases and 40 skulls that were examined in Department of Anatomy, Ege University Medicine Faculty. The age and gender of these dry adult skulls were not available.
The types of anterior opening of the Vidian canal were classified as oval shaped, funnel shaped, round shaped and septated.
The morphology of the Vidian canal was classified into two types according to the localization on the body of sphenoid:
Embedded type: The Vidian canal was embedded into the body of sphenoid bone.
Protruded type: The Vidian canal was partially or totally protruded to sphenoidal sinus.
The anterior opening location of the Vidian canal was classified into two types according to the relationship to the medial lamina of the pterygoid process:
-
1.
The Vidian canal located medial to the medial lamina of the pterygoid process.
-
2.
The Vidian canal located lateral to the medial lamina of the pterygoid process.
The parameters were measured:
-
1.
The length of the Vidian canal.
-
2.
The anterior opening diameter of the Vidian canal.
-
3.
The posterior opening diameter of the Vidian canal.
-
4.
The mean distance between anterior opening of the Vidian canal and foramen rotundum.
-
5.
The distance between anterior opening of the Vidian canal and posterior edge of sphenopalatine foramen.
-
6.
The distance between the sphenopalatine foramen and lateral margin of piriform aperture.
-
7.
The horizontal diameter of sphenopalatine foramen.
-
8.
The vertical diameter of sphenopalatine foramen.
-
9.
The distance between anterior opening of the Vidian canal and midline.
-
10.
The distance between anterior opening of the Vidian canal and lateral side of piriform aperture.
-
11.
The distance between posterior opening of the Vidian canal and midline.
-
12.
The distance between posterior opening of the Vidian canal and medial edge of foramen lacerum.
-
13.
The mean distance between posterior opening of the Vidian canal and foramen ovale.
-
14.
The angle between the Vidian canal and midline.
The vertical distances were measured using a digital caliper to the nearest 0.01 mm. If it was not possible to measure the distances directly by caliper, a thin wire was placed between two points of the distance, then the distance was measured on wire by the digital caliper. The study conforms to the provisions of the Helsinki Declaration of 1964 and all subsequent revisions.
All statistical analyses were performed using SPSS software (ver. 18.0; SPSS Inc., Chicago, USA). Descriptive statistics are presented as means ± standard deviations. The Chi-squared (χ2) test was utilized to explore whether differences between the pneumatization of sphenoidal sinus and the relationship of the Vidian canal (protruded type) were significant (p < 0.05).
Results
The Vidian canal (pterygoid canal) connecting pterygopalatine fossa and foramen lacerum was present bilaterally in all specimens. The mean length of the Vidian canal was 16.2 ± 2.6 mm. The anterior opening of the Vidian canal was observed as oval shaped on 57 specimens (31.1%) (Fig. 1), funnel shaped on 58 specimens (31.7%) (Fig. 2), round shaped on 64 specimens (35%) (Fig. 3) and septated on 4 specimens (2.2%) (Fig. 4, Table 1). The anterior opening diameter of the Vidian canal was 4.2 ± 1.2 mm and the posterior opening diameter was 2.6 ± 0.7 mm.

Oval shaped anterior opening of Vidian canal—arrow anterior opening of Vidian canal, pp pterygoid process, ms maxillary sinus, ss sphenoidal sinus, R right side (anterior view)

Funnel shaped anterior opening of Vidian canal—arrow anterior opening of Vidian canal, pp pterygoid process, ms maxillary sinus, ss sphenoidal sinus, R right side (anterior view)

Round shaped anterior opening of Vidian canal—arrow anterior opening of Vidian canal, pp pterygoid process, fr foramen rotundum, ss sphenoidal sinus, L left side (anterior view)

Septated anterior opening of Vidian canal—arrow anterior opening of Vidian canal, pp pterygoid process, ms maxillary sinus, s: sphenoidal sinus, R right side (anterior view)
Accessory anterior opening of Vidian canal was determined on 10 specimens. Five of 10 specimens were on right side and five were on the left side. Six of them were located lateral to proper opening of Vidian canal. Four of them were located medially.
Vidian canal was embedded into the body of sphenoid on 55 specimens (52.4%) (embedded type) and protruded to sphenoidal sinus on 50 specimens (47.6%) (protruded type) (Fig. 5). 21 specimens of 50 were partial (20%) and 29 specimens were total (27.6%). There were dehiscences in the bony roof of Vidian canal on 21 specimens of 50 protruded type on the base of sphenoidal sinus (20%) (Fig. 6, Table 2).

Protruded type Vidian canal—arrow protrusion of Vidian canal, pp pterygoid process, ms maxillary sinus, ss sphenoidal sinus, c clivus, sf sphenopalatine foramen, L left side (midsagittal plane)

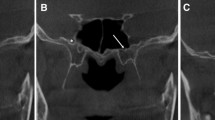
Dehiscence in the bony roof of Vidian canal—arrow dehiscence of Vidian canal, ss sphenoidal sinus, c clivus, Ant anterior, Post posterior, L left side (midsagittal plane)
The anterior opening location of the Vidian canal was also assessed according to medial lamina of pterygoid process. It was located medially 169 of specimens (92.3%) (Fig. 7) and laterally 14 specimens (7.7%).

The anterior opening position of the Vidian canal was medial to the medial lamina of pterygoid process—arrow anterior opening of Vidian canal, pp pterygoid process, ns nasal septum, pa piriform aperture, inc inferior nasal concha, if infra-orbital foramen, orb orbit (anterior view)
The relationship between anterior opening of the Vidian canal and foramen rotundum was also observed. Only in one specimen, anterior opening of the Vidian canal was medial to foramen rotundum and they were closer to each other. In all other specimens, anterior opening of the Vidian canal was inferomedial to foramen rotundum (Figs. 8, 9). The mean distance between anterior opening of the Vidian canal and foramen rotundum was 7 ± 2.1 mm.

The anterior opening of the Vidian canal was medial to foramen rotundum—Vc anterior opening of Vidian canal, pp pterygoid process, fr foramen rotundum, ss sphenoidal sinus, orb orbit, mp mastoid process, R right side (anterior view)

The anterior opening of the Vidian canal was inferomedial to foramen rotundum—Vc anterior opening of Vidian canal, pp pterygoid process, fr foramen rotundum, ss sphenoidal sinus, orb orbit, mp mastoid process, L left side (anterior view)
The distance between anterior opening of the Vidian canal and posterior edge of sphenopalatine foramen was 4.6 ± 0.2 mm. The distance between the sphenopalatine foramen and lateral margin of piriform aperture was 45.1 ± 5.2 mm. The mean horizontal diameter of sphenopalatine foramen was 5.7 ± 1.6 mm, the mean vertical diameter was 5.7 ± 1.6 mm.
The distance between anterior opening of the Vidian canal and midline was 10.1 ± 2.1 mm.
The distance between anterior opening of the Vidian canal and lateral side of piriform aperture averaged 53.3 ± 5.3 mm.
The distance between posterior opening of the Vidian canal and midline was 14.9 ± 2.0 mm.
The distance between posterior opening of the Vidian canal and medial edge of foramen lacerum was 5.6 ± 1.3 mm.
The mean distance between posterior opening of the Vidian canal and foramen ovale was 7.0 ± 1.7 mm.
The angle between the Vidian canal and midline was 17.6° ± 7.4°.
The sphenoidal sinus might be assessed in 105 specimens. The pneumatization of sphenoidal sinus had two variations: 87 specimens of 105 was sellar type and the other specimens had presellar type (Figs. 10, 11). The conchal pneumatization type was not seen in present study. If the pneumatization of sphenoidal sinus was sellar type, the Vidian canal was observed as more protruded type (p = 0.001 < 0.05) (Table 3). A statistically significant difference between the pneumatization of sphenoidal sinus and the relationship of the protruded type Vidian canal (p = 0.001 < 0.05).

The pneumatization of sphenoidal sinus was sellar type—arrow and ss sphenoidal sinus, c clivus, L left side (midsagittal plane)

The pneumatization of sphenoidal sinus was presellar type— arrow and ss sphenoidal sinus, c clivus, sf sphenopalatine foramen, L left side (midsagittal plane)
Discussion
The effectiveness of Vidian neurectomy to control the symptoms of vasomotor rhinitis and allergic rhinitis is well described in literature. However, since the Vidian nerve is located deeply within the sphenoid bone, the surgical treatment period has the difficulties. The techniques for approaching the Vidian nerve can be classified as transantral, transsphenoidal, intrasphenoidal, transpalatal and transnasal [4, 6, 7, 9, 11, 12].
The length of Vidian canal was 16.2 ± 2.6 mm while it was 13.7 mm in the study of Osawa et al. The distance between anterior opening of the Vidian canal and midline was 10.1 ± 2.1 mm in present study however it was 10.8 mm in Osawa et al.’s study. Also the distance between posterior opening of the Vidian canal and midline was 14.9 ± 2.0 mm while it was 15.1 mm in Osawa et al.’s study. The mean distance between posterior opening of the Vidian canal and foramen ovale was 7.0 ± 1.7 mm although it was 6.9 mm in Osawa et al.’s study [14].
The Vidian canal was classified into three types based on preoperative CT (computed tomography) findings by Lee et al. [11]. They examined that the Vidian canal completely within the sphenoidal sinus (type 1) in 28%, on the floor of sphenoidal sinus (type 2) in 47% and completely embedded in the body of sphenoid (type 3) in 25% of the cases as Vidian canal was embedded into the body of sphenoid on 55 specimens (52.4%) (embedded type) and protruded to sphenoidal sinus on 50 specimens (47.6%) (protruded type) in our study. According to Lee et al. study, the most common configuration of the Vidian canal was type 2. This was a different finding from ours (Table 4). The most common type in present study was embedded type (type 3 for Lee et al. study) [11]. Actually, Vidian neurectomy can be done within the sphenoidal sinus without entering the pterygopalatine fossa in case of presence of protruded type.
Omami et al. (2011) studied in 600 specimens on coronal sinonasal CT images that were collected from 300 adult patients. They also observed type 1 (38.3%), type 2 (39.6%) and type 3 (22%) [13] (Table 4). Açar et al. [1] performed a study using paranasal multidetector computed tomography images that were obtained from 250 human adults. They also observed type 1 (55.6%), type 2 (34.8%) and type 3 (9.6%) (Table 4). When they examined the relationship between the variations of Vidian canal types and surrounding structures, they noticed that the Vidian canal was located medially to medial lamina of pterygoid process in 78.8% of cases in type 1, in 87.9% in type 2 and in 9.2% in type 3 while laterally to medial lamina of pterygoid process in 21.2% in type 1, 12.1% in type 2 and 20.8% in type 3. Bahşi et al. [3] investigated Vidian canals using cone-beam computed tomography (CBCT) images that were obtained from 400 human adults. They also reported type 1 (35.87%), type 2 (44.37%) and type 3 (19.75%) (Table 4). They recorded that the position of the Vidian canal was medial (34.62%), on the same line (55.12%) and lateral (10.25%) to the medial plate of the pterygoid process. In present study the anterior opening location of the Vidian canal was observed according to medial lamina of pterygoid process. It was located medially 169 of specimens (92.3%) and laterally 14 specimens (7.7%). In the view from piriform aperture through the nasal cavity, anterior opening of Vidian canal to medial lamina of pterygoid process has an advantage for Vidian nerve surgery because of entire opening.
Lee et al. [9] emphasized that Vidian neurectomy can be easily done by intrasphenoidal approach in patients with protrusion of Vidian canal. Protrusion of the Vidian canal runs through the floor of the sphenoidal sinus from medial to lateral side. A better understanding of the anatomy of the pterygopalatine fossa and Vidian canal may led to a better surgical approach to Vidian nerve. CT scan can demonstrate the pneumatization of the sphenoidal sinus and Vidian canal. The instruments required are also needed a better understanding of this anatomic region [10]. In our study, we observed if the pneumatization of the sphenoidal sinus type was sellar type, the Vidian canal observed as more protruded type.
Previous literature also parallels the findings of the present study. For instance Gibelli et al. [5] reported a relationship between pneumatization of the sphenoidal sinuses and protrusion the Vidian canal. It was also noted that these anatomical variations have important clinical implications for endoscopic surgery. Also, according to Papavolisse et al. [16] there is a statistically significant relationship between the protrusion of Vidian canal and the lateral pneumatization of the sphenoidal sinuses.
In some previous studies presence of the dehiscences were reported. This number was between 4.4 and 32% in various radiological studies, while this ratio was 5% in Osawa et al.’s study [8, 14, 15, 19]. However, higher number of dehiscences is also possible to observe. For example in Omami et al.’s study this number was reported to be 26% and in the study of Yeğin et al. dehiscence in the bony roof of Vidian canal was present in 24.2% of their specimens [13, 20]. In the present study this ratio was found to be 20%.
A detailed anatomic knowledge presented in this study by morphometric values will also help to use the endoscopic techniques and decrease the surgical complications associated with endoscopic Vidian neurectomy.
There are some limitations to the present study caused by lack of access to old data. Records about age and gender of specimens were no longer available.
Conclusion
Vidian canal and Vidian nerve are deeply located structures on skull. We consider that knowledge of anatomical features of Vidian canal will support decreasing postoperative complications such as bleeding from the sphenopalatine artery. Preoperative imaging by CT is important for a safe surgical approach for preserving the nerve and surrounding anatomical structures, selecting of appropriate surgical approaches.
References
Acar G, Cicekcibasi AE, Cukurova I, Ozen KE, Seker M, Guler I (2019) The anatomic analysis of the Vidian canal and the surrounding structures concerning Vidian neurectomy using computed tomography scans. Braz J Otorhinolaryngol 85(2):136–143
Bahsi I (2018) Life of Guido Guidi (Vidus Vidius), who named the Vidian canal. Childs Nerv Syst. https://doi.org/10.1007/s00381-018-3930-7
Bahsi I, Orhan M, Kervancioglu P, Yalcin ED (2019) The anatomical and radiological evaluation of the Vidian canal on cone-beam computed tomography images. Eur Arch Otorhinolaryngol 276(5):1373–1383
el Shazly MA (1991) Endoscopic surgery of the vidian nerve. Preliminary report. Ann Otol Rhinol Laryngol 100(7):536–539
Gibelli D, Cellina M, Gibelli S, Cappella A, Oliva AG, Termine G, Dolci C, Sforza C (2020) Relation between volume of sphenoid sinuses and protrusion of Vidian nerve: possible applications to Vidian neurectomy. Surg Radiol Anat 42(5):583–587
Golding-Wood PH (1983) Transantral vidian neurectomy. In: Ballantyne JC, Harrison DFN (eds) Rob & Smith’s operative surgery. Nose and throat, 4th edn. Blantrye Printing Ltd, London & Glasgow, pp 126–138
Kassam AB, Vescan AD, Carrau RL, Prevedello DM, Gardner P, Mintz AH, Snyderman CH, Rhoton AL (2008) Expanded endonasal approach: Vidian canal as a landmark to the petrous internal carotid artery. J Neurosurg 108:177–183
Kim HS, Kim DI, Chung IH (1996) High-resolution CT of the pterygopalatine fossa and its communications. Neuroradiology 38(Suppl 1):S120–S126
Lee JC, Hsu CH, Kao CH, Lin YS (2009) Endoscopic intrasphenoidal vidian neurectomy: how we do it. Clin Otolaryngol 34:568–571
Lee JC, Kao CH, Hsu CH (2010) Endoscopic vidian neurectomy. An on-line video tutorial: how to do it. Clin Otolaryngol 35:496–499
Lee JC, Kao CH, Hsu CH, Lin YS (2011) Endoscopic transsphenoidal vidian neurectomy. Eur Arch Otorhinolaryngol 268(6):851–856
Lee JC, Lin YS (2012) Endoscopic vidian neurectomy: update on techniques and evidence. Curr Opin Otolaryngol Head Neck Surg 20:66–72
Omami G, Hewaidi G, Mathew R (2011) The neglected anatomical and clinical aspects of pterygoid canal: CT scan study. Surg Radiol Anat 33:697–702
Osawa S, Rhoton AL Jr, Seker A, Shimizu S, Fujii K, Kassam AB (2009) Microsurgical and endoscopic anatomy of the vidian canal. Neurosurgery 64(5 Suppl 2):385–411 (discussion 411-2)
Pandolfo I, Gaeta M, Blandino A, Longo M (1987) The radiology of the pterygoid canal: Normal and pathologic findings. AJNR Am J Neuroradiol 8:479–483
Papavasileiou G, Hajiioannou J, Kapsalaki E, Bizakis I, Fezoulidis I, Vassiou K (2020) Vidian canal and sphenoid sinus: an MDCT and cadaveric study of useful landmarks in skull base surgery. Surg Radiol Anat 42:589–601
Standring S (ed) (2005) Gray’s anatomy: the anatomical basis of clinical practice, 29th edn. Elsevier Churchill Livingstone, Edinburgh (Scotland), p 578
Tubbs RS, Salter EG (2006) Vidius Vidius (Guido Guidi) (C. 1509–1569). Neurosurgery 59:201–203
Unal B, Bademci G, Bilgili YK, Batay F, Avci E (2006) Risky anatomic variations of sphenoid sinus for surgery. Surg Radiol Anat 28:195–201
Yegin Y, Mustafa C, Ahmet A, Baverk MS, Burak O, Fatma TK (2017) Vidian canal types and dehiscence of the bony roof of the canal: an anatomical study. Turk Arch Otorhinolaryngol 55:22–26. https://doi.org/10.5152/tao.2017.2038
Author information
Authors and Affiliations
Contributions
HU was involved in project development, in data analysis and manuscript writing; ZAAI contributed to project development and manuscript writing; MDY analyzed the data, data collection and manuscript editing; EB was involved in data analysis and manuscript editing; LO performed protocol development, data management and manuscript editing.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ucerler, H., Aktan Ikiz, Z.A., Yoruk, M.D. et al. Morphometric assessment of important landmarks on skull intended for Vidian nerve surgery. Surg Radiol Anat 42, 987–993 (2020). https://doi.org/10.1007/s00276-020-02516-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-020-02516-5