
Abstract
Background
The structure and function of the serratus anterior muscle are partitioned into three parts. If the morphological characteristics in each part can be demonstrated in more detail, the cause of dysfunction will probably be identifiable more accurately. The purpose of this study was to demonstrate the details of the structure and innervation in each part of the serratus anterior muscle.
Materials and methods
This macroscopic anatomic study was conducted using ten sides from five cadavers. The structure and innervation in each part of this muscle were examined.
Results
In the superior part, the independent branch was divided from a branch innervating the levator scapulae muscle. In the middle part, the long thoracic nerve descended on one-third of the anterior region between the origin and insertion. In the inferior part, the long thoracic nerve which ramified into many branches and branches from the intercostal nerves were distributed on all sides.
Conclusion
This study demonstrated that the innervation of the serratus anterior muscle was different in each part. The difference indicates that the superior part has an intimate relation with the levator scapulae muscle while the middle and inferior parts could be the actual serratus anterior muscle. Moreover, the distribution of branches from the intercostal nerves shows that the inferior part has a connection with some trunk elements. Understanding these characteristics of innervation is useful to identify the cause of dysfunction. In addition, we assert that the constant distribution of branches from the intercostal nerves is significant for the morphology.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The serratus anterior muscle originates from the first to ninth rib and is inserted into the superior angle, medial border and inferior angle of the scapula. This large muscle is generally partitioned into three parts based on the definition by Eisler [5]. The superior part originates from the first and second ribs and is inserted onto the superior angle, the middle part originates from the second and third ribs and is inserted onto the medial border, and the inferior part originates from the ribs inferior to the third rib and is inserted onto the inferior angle.
The serratus anterior muscle is innervated by the long thoracic nerve, which is usually composed of the fifth cervical nerve (C5), C6, C7, and sometimes C8 [5]. Branches from C5 and C6 often pierce the middle scalene muscle [5, 29].
The superior part forms the main axis of rotation, the middle part draws the scapula forward, the inferior part rotates upward [6]. If the serratus anterior muscle is impaired by a disorder of the long thoracic nerve, patients cannot elevate or reach their upper limb because of what is called scapular winging. The causes of this condition have been thought to be various, such as compression by the middle scalene muscle, the second rib or the fascial sheath, entrapment in the middle or posterior scalene muscle, and traction [15, 18, 24]. That is, the disorder of the long thoracic nerve is likely to result from various causes. Therefore, when a physical therapist treats the dysfunction of the serratus anterior muscle, it is essential to evaluate what causes are related to its dysfunction. However, little has been reported on the arrangement and insertion of muscular fascicles or the course and distribution of nerves overall and in detail. If these morphological characteristics can be demonstrated in each part, physical therapists will be able to identify the cause of dysfunction more accurately.
The purpose of this study, therefore, is to demonstrate the details of the structure and innervation in each part of the serratus anterior muscle.
Materials and methods
The study was carried out on ten sides of five adult Japanese cadavers fixed in 8 % formaldehyde and preserved in 30 % ethanol (average age: 77.8). Four males and one female were dissected under the stereomicroscope (magnification: 12×, Operation Microscope OLYMPUS OME-1000, Olympus Optical, Tokyo).
First, the clavicle was cut and the middle scalene, levator scapulae, rhomboid which includes the rhomboid major and rhomboid minor muscles, serratus anterior muscles, and cervical and brachial plexuses were identified. The courses of the nerves innervating the levator scapulae, rhomboid, and serratus anterior muscles were examined. Then, the insertions of these three muscles were cut off the scapula. The upper limb including the scapula was separated from the thorax, and the arrangement of muscular fascicles of the serratus anterior muscle was examined. The origin of the rhomboid muscles was also cut off from the thoracic vertebrae. As the connective tissues between the serratus anterior muscle and thoracic wall were carefully removed using tweezers, the rhomboid and serratus anterior muscles were reversed laterally. After the branches from the intercostal nerves were found in the connective tissues, they were marked by threads, and their segments were identified. Then, the branches were cut to separate the serratus anterior muscle from the thoracic wall, so that a mass of these three muscles and nerves of cervical and brachial plexuses were obtained.
Second, the segments and distribution of the nerves innervating these three muscles were investigated. On five sides, the intramuscular distribution of the serratus anterior muscle was also investigated. The courses and distribution of the branches from the intercostal nerves were examined.
Results
The structure in each part of the serratus anterior muscle
The origin, insertion, and muscular arrangement in each part were examined (Fig. 1a). Some muscular fascicles of the superior part were hanging over the superior angle and were inserted onto not only the superior angle but also the medial border (Fig. 1b). The muscular fascicle was bounded by the levator scapulae muscle. The middle part originated from the narrow space of the second and third ribs and was inserted onto the broad space of the medial border. The middle part was thinner than the other parts. In one case, the muscular fascicles were changed into connective tissue (Fig. 1c). In the inferior part, most of the muscular fascicles were attached to the inferior angle of scapula. The rest of the muscular fascicles were adjoined to the rhomboid major muscle (Fig. 1d). On one side, these muscular fascicles were mixed with the rhomboid major muscle throughout its tendon.

a Three parts of the serratus anterior muscle, right side. b The anterior view of the superior part. The region of the white square is magnified. Some muscular fascicles were hanging over the superior angle (arrow), and the insertion expanded to the medial border (arrowhead). c The lateral view of the serratus anterior muscle. The muscular fascicles originating from the second rib were absent. Instead, the space was composed of connective tissue. d The posterior view of the inferior part. Most of the muscular fascicles were condensed to the inferior angle (circle), and a part of the muscular fascicles (asterisk) was adjoined to the rhomboid major muscle (arrow). LS levator scapulae muscle, LT long thoracic nerve, R rib, RH rhomboid muscles
The serratus anterior muscle was divided into each part with a small fusion. The superior part overlapped the middle part, and a part of the middle part was covered by the inferior part.
The innervation of levator scapulae, rhomboid and serratus anterior muscles
The segments and courses of the nerves innervating three muscles were examined (Fig. 2). The nerves originating from C3 and C4 mainly innervated the levator scapulae muscle. These nerves turned dorsolaterally and entered the levator scapulae muscle from the lateral surface. The nerves originating from C4 and C5 mainly innervated the rhomboid muscles. The nerve from C4 entered the levator scapulae muscle from the lateral surface, penetrated it and communicated with the nerve from C5 which passed behind the levator scapulae muscle, then these nerves innervated the rhomboid muscles. The serratus anterior muscle was mainly innervated by the nerves originating from C5, C6, and C7. The nerve from C4 was related to the three sides and the nerve from C8 to the five sides.

The segments and courses of the nerves innervating LS, RH, and the serratus anterior muscle. In the cervical region of the right side, the nerves to LS (open arrowhead), the nerves to RH and the nerves to the serratus anterior muscle (arrowhead) are shown. LS was mainly innervated by the nerves from C3 and C4, RH by the nerves from C4 and C5, and the serratus anterior muscle by the nerves from C5 to C7. The nerves distributed to the superior part and cranial area of the middle part turned dorsolaterally and entered from the lateral surface (asterisk). a The independent branch formed a common trunk (arrow) with the nerve to RH. The nerve from C8 also innervated the serratus anterior muscle. b The independent branch formed common trunks (arrow) with not only the nerve to RH but also the branch to LS. The common trunk between the independent branch and the nerve to RH pierced MS. MS middle scalene muscle
The innervation in each part of the serratus anterior muscle
The innervation in each part was examined (Fig. 3). The nerves innervating the superior part had two different sources: one was an independent branch not related to the main trunk of the long thoracic nerve, and the other was the long thoracic nerve. The independent branch was found on nine sides. On six sides, the independent branch was divided from a branch innervating the rhomboid muscles (Fig. 2a). On one sides, it was divided from a branch innervating the levator scapulae muscle. On two sides, it was divided from both branches (Fig. 2b). The independent branch was related to branches from C4, C5, or C6. Out of nine sides, the independent branch on eight sides pierced the middle scalene muscle (Fig. 2b). The long thoracic nerve ramified into three or four short branches. These branches turned dorsolaterally and entered the superior part and the cranial area of the middle part from the lateral surface. This course was similar to that of the nerves innervating the levator scapulae muscle (Fig. 2).

The course and distribution of the nerves innervating each part of the serratus anterior muscle. a The lateral view of the right serratus anterior muscle. The insertion to the medial border of the scapula (open arrowhead) is shown. b Drawing of the same specimen as photograph (a). The superior part; the independent branch (arrowhead) which formed a common trunk (arrow) with the nerve innervating RH and three or four short branches from the long thoracic nerve were distributed (asterisk). Middle part LT descended while ramifying a few branches. Inferior part LT ramified into many branches. DS dorsal scapular nerve
In the middle part, the long thoracic nerve descended on one-third of the anterior region between the origin and insertion and ramified into a few branches (Fig. 3).
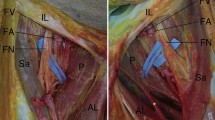
The inferior part was also innervated by the nerve originating from two sources: one was the long thoracic nerve, the other was a branch from the intercostal nerve. The long thoracic nerve ramified into many branches and they were distributed throughout the inferior part (Fig. 3). The branches from the intercostal nerves were found on all sides, and they were mainly composed of the nerve originating from T6 to T8 (Table 1). These branches penetrated the external intercostal muscles, turned caudally and posterior on the medial surface of the inferior part, and entered the inferior part (Fig. 4). On eight sides, the branches composed of one segment or two segments were distributed (Fig. 5a, b). On one side, the branches from T3 to T9 were involved (Fig. 5c, d). On three sides, this branch communicated with a branch from the long thoracic nerve (Fig. 5e, f).

Distribution of branches from the intercostal nerves. a The posterolateral view of the right thoracic wall. The serratus anterior muscle is retracted laterally. These branches penetrated the external intercostal muscle (arrow) and entered the inferior part. b The medial surface of the obtained serratus anterior muscle. The region of the white square is magnified. Branches turned caudally and posterior and were distributed to the inferior part. The asterisks correspond to each other in both figures

Variations on the distribution of branches from the intercostal nerves. The medial surface of the obtained serratus anterior muscle is shown. The region of the white square is magnified and drawn, respectively. a, b Only the branches from T6 were distributed. c, d Many branches from T3 to T9 were involved. e, f The branch communicated with the long thoracic nerve
Discussion
Differences of the characteristics of innervation in each part
In the superior part, the nerves from two different sources were distributed throughout: one was an independent branch, the other was the long thoracic nerve. The independent branch is defined as an unrelated branch for the long thoracic nerve forming the main trunk, a ramified branch before the main trunk is formed, and a comparatively thick branch [10]. Kato and Sato [10] reported that the superior part was much closer to the rhomboid muscles because the independent branch was divided from the branch innervating the rhomboid muscles, which indicated the superior part was different from the middle or inferior part. However, we observed that the independent branch formed a common trunk with the branch from C4 innervating the levator scapulae muscle on three sides. This is inconsistent with the report by Kato and Sato [10]. However, ontogenetically, the levator scapulae and serratus anterior muscle formed a continuous fibrillated mass in the 9 mm human embryo [16]. A variant muscle between the serratus anterior and levator scapulae muscles was also reported in 32.2 % of the cases [19, 20]. In addition, phylogenetically, the serratus anterior and levator scapulae muscles existed earlier than the rhomboid muscles, and these muscles have been considered to be a continuous muscle before the prosimian [5, 8, 11, 12]. Moreover, Ribbing [22] stated that although in reptiles the anterior part of the serratus magnus originated from the inferior cervical vertebrae, its origin had gradually transferred to the superior ribs during the evolutionary process. Thus, judging by both the ontogeny and phylogeny, we think it is natural that the independent branch forms the common trunk with the branch innervating the levator scapulae muscle. Meanwhile, the long thoracic nerve ramified into three or four short branches. These branches turned dorsolaterally and were distributed throughout the superior part and the cranial area of the middle part. This was very similar to the innervation of the levator scapulae muscle. These characteristics of the independent branch and the short branches from the long thoracic nerve lead us to conclude that the superior part of the serratus anterior muscle has an intimate relation with the levator scapulae muscle and is an intermediary between the levator scapulae and the rest of the serratus anterior muscles.
The middle part was thinner than the superior or inferior part. In one case, the muscular fascicles were even absent. Bergman [1] also reported the presence of connective tissue instead of muscular fascicles. The long thoracic nerve descended on the middle part and ramified into comparatively fewer branches than the superior or inferior part. The characteristics of the middle part are obviously different from that of the superior part. However, this could be natural, based on the comparative anatomy. Besides previously mentioned Reptilia, Aves, Monotremata, or Mammalia such as Chiroptera, Erinaceidae, Leporidae, the serratus anterior muscle is considered to be composed of two parts: the cranial part and caudal part [22]. Both parts move away from each other, namely, the middle part in humans does not exist. That is to say, based on comparative anatomy, it could be said that the region corresponding to the middle part was immature. We suppose that the middle part could be the beginning part of the actual serratus anterior muscle which is innervated by the main trunk of the long thoracic nerve and may be just a connecting part between the superior part and inferior part.
In the inferior part, we found that the branches from the intercostal nerves were distributed to the serratus anterior muscle on all sides. Kodama [14] also reported that the branches from the intercostal nerves were distributed to the serratus anterior muscle or to a variant muscle under the serratus anterior muscle, however, the frequency was only 17 %. We maintain that the frequency is much higher in the Japanese cadavers because these branches are constantly distributed to the serratus anterior muscle. Moreover, we suppose that the serratus anterior muscle is affected by not only the cervical somites but also the thoracic somites. The cervical and thoracic elements often coexist in a structure or region. Kida et al. [13] reported a case of the serratus posterior superior muscle supplied by both the intercostal and dorsal scapular nerve. Kasai et al. [9] stated that although the intercostobrachial nerve was usually distributed in the brachial region, a part of the nerve remains on the thoracic wall. In addition, some reports examined the pectoralis major muscle innervated by the intercostobrachial nerve [17] or the levator scapulae muscle innervated by the posterior branch of the second cervical nerve [28]. In this study, we showed that the branches from the intercostal nerves communicated even with the long thoracic nerve. In other words, the boundary between the cervical and thoracic region is not clear and both regions overlap. Moreover, in their developmental studies, Huang et al. [7] and Shearman [23] found that the scapular blade and the attaching muscle in chicks did not originate from somites 13–16, which were related to the formation of the shoulder girdle, but from the somites 17–24. Valasek et al. [25, 26] demonstrated that the medial border and a part of the attaching muscles in mice did not express Met and Pax3; namely, these muscles did not migrate to become limb muscles. In conclusion, the distribution of the branches from the intercostal nerves on all sides leads us to believe that the inferior part of the serratus anterior muscle has a connection with some trunk elements.
Function of each part based on the structure and innervation
In the superior part, some muscular fascicles were hanging over the superior angle of the scapula, and were inserted onto not only the superior angle but also the medial border. This characteristic supports the idea that the superior part plays a role as the anchor [6]. In the inferior part, a part of the muscular fascicles was connected with the rhomboid major muscle by tendon. Braus [3] has indicated that this connection forms a straight structure from the ribs to the vertebrae which has an effect on respiration or postural control. We consider that this connection would be an essential structure affecting the expansibility of the serratus anterior and rhomboid major muscles for the upper rotation of the scapula.
Recent studies on the innervation have shown the segments, division, length, and diameter of the long thoracic nerve [2, 27, 29, 30]. However, the characteristics of each part have not been previously mentioned. In this study, we demonstrated that each part of the serratus anterior muscle has its own characteristic in terms of innervation. From these characteristics, the superior part has an intimate relation with the levator scapulae muscle. The levator scapulae muscle is generally considered to be antagonistic to the serratus anterior muscle because it functions for lower rotation of the scapula. However, we suggest that only the superior part can act to coordinate with the levator scapulae. In the middle part, the long thoracic nerve descends with comparatively fewer branches, while in the inferior part, the nerve ramifies into many branches. This characteristic provides evidence that upper rotation of the scapula by the inferior part is much stronger than the forward draw by the middle part. We think that understanding these characteristics of innervation in each part is useful to identify the cause of dysfunction.
In addition, the serratus anterior muscle has been considered to play a role as an accessory muscle of respiration [21]. However, recently Cannon et al. [4] have concluded that the serratus anterior muscle shows little muscular effort in respiration. These views are inconsistent with each other. Considering that the inferior part is constantly innervated by the branches from the intercostal nerves, the serratus anterior muscle has the potential to cooperate with other respiratory muscles to help ventilation. However, this function is not clear because a histological study has not been conducted to prove whether the branch is a motor or sensory neuron. In the future, additional study is needed to prove the function of the branch from the intercostal nerve distributed to the serratus anterior muscle.
Conclusion
The structure and function of the serratus anterior muscle have been partitioned into three parts based on its origin and insertion. This study showed that the innervation was also different in each part. Understanding the characteristics of the innervation in each part is useful to identify the cause of dysfunction. In addition, we found that the serratus anterior muscle was innervated by the branches from the intercostal nerves on all sides. We assert that this fact is very significant for morphology of the serratus anterior muscle. In the future, additional study is needed to prove the function of the branch from the intercostal nerve distributed to the serratus anterior muscle.
References
Bergman RA, Thompson SA, Afifi AK, Saadeh FA (1988) Muscles. In: Compendium of human anatomic variation. Urban & Schwarzenberg, Baltimore, pp 1–51
Bertelli JA, Ghizoni MF (2005) Long thoracic nerve: anatomy and functional assessment. J Bone Joint 87:993–998
Braus-Elze (1954) Spezielle Bewegungsapparate der oberen Extremität. In: Anatomie des Menchen. 3. Anfl. Bd. I. Springer, Berlin, pp 202–417
Cannon DT, Grout SL, May CA, Strom SD, Wyckoff KG, Cipriani DJ, Buono MJ (2007) Recruitment of the serratus anterior as an accessory muscle of ventilation during graded exercise. J Physiol Sci 57:127–131
Eisler P (1912) Muskeln der Brust. Musculi thoracis. In: Die Muskelen des Stammes. Gustav Fischer, Jena, pp 455–561
Gregg JR, Labosky D, Harty M, Lotke P, Ecker M, DiStefano V, Das M (1979) Serratus anterior paralysis in the young athlete. J Bone Joint Surg Am 61:825–832
Huang R, Zhi Q, Patel K, Wilting J, Christ B (2000) Dual origin and segmental organisation of the avian scapula. Development 127:3789–3794
Kardong KV (2006) The muscular system. Vertebrates Comparative Anatomy, Function, Evolution. The McGraw-Hill Companies, New York, pp 365–396
Kasai T, Yamamoto N (1966) Medial brachial cutaneous nerves and the intercostobrachial nerves. Kaibogaku Zasshi 41:29–42 (in Japanese)
Kato K, Sato T (1978) Morphological analysis of the levator scapulae, rhomboideus and serratus anterior. Kaibogaku Zasshi 53:339–356 (in Japanese)
Kato K, Sato T (1984) Innervation of the levator scapulae, the serratus anterior, and the rhomboideus in crab-eating macaques and its morphological significance. Anat Anz 157:43–55
Kato K, Sato T (1993) Innervation of the levator scapulae, the serratus anterior, the romboideus and the scapular muscles in the gray kangaroo (Macropus giganteus). Comparisons are drawn to the crab-eating macaque and man. Ann Anat 175:21–28
Kida Y, Tani M (1993) The human superior posterior serratus muscle supplied by both the intercostal and dorsal scapular nerves. Kaibogaku Zasshi 68:162–168 (in Japanese)
Kodama K (1986) Morphological significance of the supracostal muscles, and the superficial intercostal nerve—a new definition. Kaibogaku Zasshi 61:107–129 (in Japanese)
Laulan J, Lascar T, Saint-Cast Y, Chammas M, Le Nen D (2011) Isolated paralysis of the serratus anterior muscle successfully treated by surgical release of the distal portion of the long thoracic nerve. Chir Main 30:90–96
Lewis WH (1901) The development of the arm in man. Am J Anat 1:145–183
Loukas M, Louis RG Jr, Fogg QA, Hallner B, Gupta AA (2006) An unusual innervation of pectoralis minor and major muscles from a branch of the intercostobrachial nerve. Clin Anat 19:347–349
Martin RM, Fish DE (2008) Scapular winging: anatomical review, diagnosis, and treatments. Curr Rev Musculoskelet Med 1:1–11
Nishi S (1919) Nihonzin-no Kingakuchiken Haikin-no Toukeitekikenkyu. Tohoku Med J 1:249–263 (in Japanese)
Nishi S (1953) MIOLOGIO DE LA JAPANO. Statistika raporto pri muskolanomalioj ĉe japanoj. III. Muskoloj de trunko (1). Gumma J Med Sci 2:109–121
Reid DC, Bowden J, Lynne-Davies P (1976) Role of selected muscles of respiration as influenced by posture and tidal volume. Chest 70:636–640
Ribbing L (1938) Dei Muskeln und Nerven der Extremitaten. In: Bolk L, Göppert E, Kallius E, Lubosch W (eds) Handbuch der vergleichenden Anatomie der Wirbeltiere. Urban & Schwarzenberg, Berlin, pp 543–652
Shearman RM, Tulenko FJ, Burke AC (2011) 3D reconstructions of quail—chick chimeras provide a new fate map of the avian scapula. Dev Biol 355:1–11
Tubbs RS, Salter EG, Custis JW, Wellons JC 3rd, Blount JP, Oakes WJ (2006) Surgical anatomy of the cervical and infraclavicular parts of the long thoracic nerve. J Neurosurg 104:792–795
Valasek P, Theis S, Krejci E, Grim M, Maina F, Shwartz Y, Otto A, Huang R, Patel K (2009) Somitic origin of the medial border of the mammalian scapula and its homology to the avian scapula blade. J Anat 216:482–488
Valasek P, Theis S, DeLaurier A, Hinits Y, Luke GN, Otto AM, Minehin J, He L, Christ B, Brooks G, Sang H, Evans DJ, Logan M, Huang R, Patel K (2011) Cellular and molecular investigations into the development of the pectoral girdle. Dev Biol 357:108–116
Wang JF, Dang RS, Wang D, Zhang ZY, Liu Z, Huang HL, Wu AQ, Zhang CS, Chen EY (2008) Observation and measurements of long thoracic nerve: a cadaver study and clinical consideration. Surg Radiol Anat 30:569–573
Yamasaki M, Takahashi F (1983) The 1st bundle of the levator scapulae innervated by an aberrant branch of the 2nd dorsal cervical ramus. Kaibogaku Zasshi 58:51–58 (in Japanese)
Yazar F, Comert A (2009) Origin types of the long thoracic nerve. Surg Radiol Anat 31:737
Yazar F, Kilic C, Acar HI, Candir N, Comert A (2009) The long thoracic nerve: Its origin, branches, and relationship to the middle scalene muscle. Clin Anat 22:476–480
Acknowledgments
This study was partly supported by a Grant-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports (C) (No. 20590168) and also supported by a grant from Nokyo Kyosai Research Institute (Agricultural Cooperative Insurance Research Institute).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Nasu, H., Yamaguchi, K., Nimura, A. et al. An anatomic study of structure and innervation of the serratus anterior muscle. Surg Radiol Anat 34, 921–928 (2012). https://doi.org/10.1007/s00276-012-0984-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-012-0984-1