
Abstract
Background
The variable incidence of sigmoid volvulus, which depends on the presence of an elongated sigmoid colon, suggests the possibility of variations in the length of the sigmoid colon. This study was undertaken among the three major population groups to prove this hypothesis.
Patients and methods
Radiological films of patients of the three population groups (African, Indian and White) undergoing barium enema were reviewed. The stature was measured by the distance from T12 to L4. The collective length of the rectum and sigmoid colon as well as the entire colon was measured on the barium enema film using an opisometer. Measurement was from the upper border of the symphysis pubis to the upper border of the left iliac crest. The level of the apex of the sigmoid colon loop and its redundancy were also assessed.
Results
There were 109 patients (61 females) undergoing barium enema (39 Africans, 49 Indians, and 21 Whites). For the entire group the T12–L4 distance was 16.6 ± 2.2 cm and the entire colon length was 133 cm (range 88–262 cm) and was significantly longer among African patients (P = 0.003). The combined length of the rectum and sigmoid colon was 48.8 ± 15.7 cm (Africans 60.9 ± 14.4 cm, Indians 41.3 ± 12.2 cm and Whites 44 ± 11.6 cm). The sigmoid colon was significantly more redundant in Africans (90%), compared to Indians (25%) and Whites (24%) (P = 0.003 for Indians and P = 0.048 for whites). The apex of the sigmoid colon reached L1–L3 in 54% among Africans, 6% among Indians and in 10% among Whites (10%).
Conclusion
African patients had the longest combined length of the rectum and sigmoid colon translating into a long sigmoid colon. They also had the highest number of redundant sigmoid colon. This may explain the high incidence of sigmoid volvulus in African patients.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Sigmoid volvulus has a variable geographical and racial distribution. It is common in developing countries such as in Africa, Eastern Europe and India where it represents 20–54% of intestinal obstructions [3, 14, 17, 21, 26, 28] compared to 1–7% in developed countries [3, 6, 19, 22]. In Africa, the condition occurs almost exclusively in Africans than in Whites [1, 5, 13, 21], and it shows a marked male preponderance [9, 13, 21].
The actual aetiology of sigmoid volvulus remains speculative with many aetiological factors having been suggested including chronic constipation, high fiber diet, bowel habit, high altitude and enemas containing ginger, pepper and herbal extracts [14]. These have, however, failed to satisfactorily explain the geographical variation and the male preponderance of sigmoid volvulus.
We hypothesized that the length of the sigmoid colon must play a major role in geographical and gender differences in sigmoid volvulus, considering that the condition requires an elongated sigmoid colon to develop. It has therefore become necessary to revisit the length of the sigmoid colon in the different population groups in order to explain these differences. The primary aim of this anatomico-radiological study therefore was to establish any differences in the length of the sigmoid colon between the different population groups and the secondary aim was to establish any differences in the length of the entire colon.
Materials and methods
This was a prospective study of the colon, using barium enema radiographs, in the different population groups in Durban, South Africa, in order to assess the length of the entire colon and the sigmoid colon. Ethical approval was obtained from the Biomedical Research Ethics Committee of the College of Health Sciences, University of KwaZulu-Natal. The radiographs of all patients undergoing barium enema examination at King Edward VIII and Addington Hospitals were reviewed on an ongoing basis from 1 January 2004 to 30 September 2004. The radiographs of the three major population groups were studied. The population groups were defined as Africans, Indians and Whites according to the criteria used by the South African Government.
All patients presenting for barium enema who were considered to be free of any type of colonic disease were included in the study. Exclusion criteria were (1) patients with structural disease of the colon such as diverticular disease, (2) patients in whom the structure of the colon could not be elucidated because of poor contrast or because of overlapping loops of bowel, (3) patients with megacolon, making it difficult to identify the different parts of the colon, (4) patients in whom the sigmoid colon could not be traced from the pubic symphysis to the anterior superior iliac spine because the field of view had been “cut” by the radiographer, and (5) patients with some form of malposition of the colon.
An indicator of the stature of the patient was assessed by measuring the distance from the upper border of the 12th thoracic vertebra (T12) to the lower border of the 4th lumbar vertebra (L4) in the prone control film [25]. The combined length of the sigmoid colon and rectum was measured from the prone film using an opisometer (Fig. 1). This instrument has a wheel that measures the distance in centimetres as it runs over the colon on the barium enema film (Fig. 1b). A supine film showing the entire colon from symphysis pubis to the caecum was selected. Post-evacuation films were not used. As there is no clear demarcation between rectum and sigmoid colon, a combined length of the sigmoid colon and rectum was measured. The measurements were taken from the upper part of the symphysis pubis to the upper border of the left anterior superior iliac spine. The measurement was then continued to measure the rest of the colon up to the caecum. The level of the upper limit of the sigmoid loop as measured by the highest lumbar vertebrae reached was documented. The redundancy of the sigmoid colon loop was determined and documented. All measurements were done by one investigator (TEM); sometimes with the presence of one of the other co-investigators (MRH).

a Shows a picture of an opisometer. b Shows the investigator using an opisometer to measure the colon. The wheel measures length as it is run along the colon in the barium enema radiograph
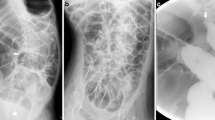
The sigmoid colon was regarded as redundant when its entire length could not be contained in the true pelvis and a large part of it had been displaced out of the pelvis into the abdomen [29]. Slight degrees of displacement due to distension were accepted as normal. Figure 2 shows a non-redundant sigmoid colon. Figure 3 shows a redundant sigmoid colon which courses first to the right, then centrally, before it descends to the pelvis. Figure 4 shows how a redundant sigmoid colon becomes “non-redundant” after evacuation.

In this barium enema the sigmoid colon is “bundled” in the pelvis

The redundant sigmoid colon courses first to the right and then centrally, before it descends to the pelvis

Barium enema films. a Shows a redundant sigmoid colon. b, is the same film with the barium having been evacuated. The originally redundant sigmoid colon appears to be “non-redundant” after evacuation
Data were collected onto a dedicated proforma sheet and then transferred onto a computer database. Data were analysed using the Statistical Package for the Social Sciences (SPSS) version 11.5. One-way ANOVA was used for comparison of means by race group. Bonferroni post hoc tests were applied for specific two-way comparisons. Mann–Whitney U test was used for comparisons of all the other variables. A P < 0.05 was taken as significant. Pair-wise subgroup comparisons between the races were done using a Bonferroni correction.
Results
The patient profile is shown in Table 1. A total of 287 barium enemas were performed during this period. One hundred and seventy-eight were excluded and only 109 barium enema radiographs were studied, of whom 61 were females and 48 were males (female to male ratio = 1.3:1). There were 39 African, 49 Indian and 21 White patients. The median age was 52 years (range 14–92 years). African patients were younger at 48 years compared to the other population groups; however, this difference was not statistically significant.
Table 2 shows comparisons of stature as determined by the T12–L4 distance, length of the colon, combined length of the rectum and sigmoid colon and redundancy of the sigmoid colon. Statistical analyses were not calculated for gender differences, as numbers were very small. The stature as reflected by the distance between T12 and L4 vertebrae was similar in all population groups. The entire colon was significantly longer in Africans compared to the other population groups (African vs. Indian P = 0.003; African vs. white P = 0.048, Indian vs. White P = 1.0). The entire colon in the total cohort tended to be longer for females than for males; in Africans it tended to be longer in males, and in Indians and Whites it tended to be longer in females. The collective length of the rectum and sigmoid colon was significantly longer in Africans compared to the other population groups (African vs. other population groups P = 0.003, Indians vs. White P = 1.0). It tended to be longer in males among Africans and longer in females among Whites and the length was similar in Indians. There was marked redundancy of the sigmoid colon in Africans compared to the other population groups (P = 0.003). Redundancy was uncommon among Indians and Whites and the difference between the two population groups was not statistically significant (P = 1.0). The apex of the sigmoid colon reached L1–L3 in 54% among Africans, 6% among Indians and in 10% among Whites (10%).
Discussion
Sigmoid volvulus is common in developing countries such as in Africa, Eastern Europe and India, where it represents 20–54% of intestinal obstructions [3, 14, 17, 21, 26, 28] compared to 1–7% in developed countries [3, 6, 19, 22]. In Africa, the condition occurs more commonly in Africans than in Whites [1, 5]. Figures for South Africa are no different from those in other developing countries; the age incidence is 42–46 years [13, 21] and the male to female ratio ranges from 9:1 to 13:1 [9, 13, 21].
Published series from South Africa only report on sigmoid volvulus from African patients and none from White and Indian patients [9, 13, 15, 21, 27, 31]. An ongoing local study in the Teaching hospitals of the University of KwaZulu-Natal has shown that only two of 99 patients treated for sigmoid volvulus were White and the rest were African [20].
The actual aetiology of sigmoid volvulus remains speculative [3]. Many aetiological factors have been suggested including chronic constipation [3, 6, 14, 17, 21, 22, 26, 28], high fiber diet [4, 14, 15, 17, 22, 26–28, 30], bowel habit [14, 30], high altitude [2, 14, 31] and enemas containing ginger, pepper and herbal extracts [7, 14]. These various aetiological factors that have been suggested have, however, failed to satisfactorily explain the geographical variation and the male preponderance of sigmoid volvulus. A number of theories have been advanced to explain this male preponderance, including the more spacious female pelvic area which allows spontaneous reduction of a beginning volvulus [11, 12] and gender specific cultural patterns of defecation which may affect the recto-sigmoid junction differently in males and females [30].
The present study has looked at the length of the sigmoid colon on barium enema radiographs in order to establish variations in the length of the sigmoid colon and thus explain some of the population differences in the clinicopathological manifestation of sigmoid volvulus. It was necessary to measure the patients’ stature in order to exclude the influence of stature on colon length. The use of the distance from T12 to L4 vertebrae has been shown by others to be an accurate reflection of the stature [25]. The stature thus assessed was similar in all population groups in this series and therefore it can be inferred that the differences in the length of the colon and the sigmoid colon in this study were independent of the patient’s stature.
The study has shown variability in the length of the entire colon and that it was longest in Africans. As there is no clear demarcation between the sigmoid colon and the rectum in the barium enema radiograph, the sigmoid colon alone could not be measured. Hence the combined length of the sigmoid colon and the rectum was measured. Since the rectum is relatively constant [32], the variable component must be the sigmoid colon. It can thus be concluded that the differences observed in these measurements reflect variation in the length of the sigmoid colon. The combined length of the rectum and sigmoid colon was also longest amongst Africans compared to other population groups and we infer from this finding that the sigmoid colon was longest in Africans. The long and redundant sigmoid colon seen in Africans may explain the high incidence of sigmoid volvulus in this population group. Whether the variation in length occurs in the mobile or fixed part of the sigmoid colon cannot be answered by this anatomico-radiological study, but further studies are required to address this question.
Other radiological studies have looked at the differences in the length of the entire colon and the sigmoid colon. In 1993, Bassey [7] undertook a radiological study in the Calabar community in Nigeria to assess the effect of chronic enema use on the length of the colon. That study demonstrated the redundancy of the segments of the colon in a high proportion of habitual enema users compared to non-users (71 vs. 19%). The sigmoid and descending colons were observed to be comparatively the most vulnerable segments for the development of redundancy. Bassey concluded that chronic enema use led to colon redundancy, including the sigmoid colon and might explain the differences. Although Bassey attributed these differences to chronic enema use, it does support our view that these variations exist.
In the study by Saunders et al. [25] in the UK total colonic length was greater in women despite the women’s smaller stature, suggesting gender differences. Gender differences were also observed in the present series although the numbers were very small. Interestingly, there were no differences in the present series between men and women in terms of stature.
Riedl [23] studied radiographs of 63 patients undergoing barium enema in Ethiopia and found a significant difference in the length of the sigmoid loops between men and women and between constipated and non-constipated patients. Men had longer and wider sigmoid colon loops than women; also, constipated patients had a longer and wider sigmoid colon than non-constipated patients. He suggested that constipation played an important role in anatomical differences of the sigmoid colon. However, that author did not calculate statistical differences.
Sadahiro et al. [24] studied barium enemas of Japanese subjects and compared the length of sigmoid colons of males and females according to age, sex and physique and found no difference in the length of the sigmoid colon in both sexes. They also found that the total colonic length was shorter in males than in females and that the length and surface area of the entire colon tended to increase with age in the whole cohort and with increase in physical dimensions in females.
All these studies support our findings of variability in the length of the entire colon and the sigmoid colon in the various communities, although the observations differ in these different communities. We believe that the redundancy of the sigmoid colon is not an anomaly as suggested by Tan [29], but just a variation from the normal.
These differences in length may also explain the reasons for failure of complete colonoscopy in patients with elongated colons. Hanson et al. [18] showed this in a study of 200 patients, who underwent CT Colonography following successful (100) and unsuccessful (100) optical colonoscopy. Patients with elongated and tortuous colons tended to have incomplete colonoscopy suggesting the difficulty associated with elongated colon. In that study, the sigmoid and transverse colons were longer in patients with failed complete colonoscopy. Saunders et al. [25] made similar observations and concluded that the elongated colon in Caucasian females might explain the difficult colonoscopy in females.
In an anatomical study of live patients and cadavers, Bhatnagar et al. [8] demonstrated variability in the length of the sigmoid colon, ranging from 25 to 86 cm in live individuals and 27–43 cm in cadavers. They concluded that the variations in the configuration of the sigmoid colon could have implications for the colonoscopist trying to negotiate this segment of the bowel with the endoscope.
Two studies [10, 16] have demonstrated variations in the ascending and descending colons and highlighted the importance of bearing this in mind when performing percutaneous nephrostomy. Although these two studies did not directly address the sigmoid colon, they do emphasize the important point made by the present study, i.e. that there are variations in the length of the segments of the colon.
There are a number of limitations to the measurements of the length of the colon and its components in a radiological study. In order to be referred for barium enema these patients must have had symptoms related to the colon; however, only films of patients in whom the barium enema revealed no pathology in the colon were included. Since there is no radiological demarcation between the rectum and the sigmoid colon, it was not possible to measure the sigmoid colon alone without including the rectum; for this reason, we measured both the rectum and the sigmoid colon. It was presumed that the length of the rectum is more or less constant and therefore any difference found would be due to the variable length of the sigmoid colon. We concede, however, that the third sacral vertebra may be used as a landmark for the demarcation of the rectum from the sigmoid on barium enema. However, the area of commencement of the sigmoid colon from the descending colon may not be constant. Some of the loops appeared “end-on” and could not be measured; this could sometimes be overcome by measuring on the lateral view of the barium enema, although this was not possible in the majority of patients. In some radiographs the colon loops were “grouped” in the pelvis and they were again difficult to measure. The nature of the study of barium enema means that barium and gas must be insufflated into the colon and this increases the diameter of the colon and causes it to move out of the pelvis. However, after evacuation of the barium the now empty sigmoid colon appears to be “non-redundant”. The timing of the picture in relation to emptying of the barium by the colon is therefore very important. The position of a mobile segment of the colon, such as the sigmoid colon can vary during a single radiological examination depending on the positioning of the patient. All the films should ideally be taken at the same phase of filling. This was not possible in the present study as the films were taken by different people and measurements were performed afterwards.
Despite these limitations, we believe that this study provides adequate information to make substantive conclusions relative to the length of the colon, the recto-sigmoid segment and the sigmoid colon. The advantages of the present study are the large number of patients and the comparison between the different population groups. To our knowledge this is the only study that compares all three population groups by radiological study in one area.
Conclusion
There is a variation in the length of the sigmoid colon and the entire colon. The differences are population based and the entire colon and the sigmoid colon are longest among Africans. This seems to be unaffected by stature. These differences might explain the geographic and racial differences in the incidence of sigmoid volvulus. Further studies with large numbers under uniform conditions are required to know further about the anatomy of the sigmoid colon. The study may also explain the difficulty experienced by colonoscopists in some patients as suggested by others.
References
Arnold GJ, Nance FC (1973) Volvulus of the sigmoid colon. Ann Surg 177:527–537
Asbun HJ, Castellanos H, Balderrama B et al (1992) Sigmoid volvulus in the high altitude in the Andes. Review of 230 cases. Dis Colon Rectum 35:350–353
Avots-Avotins KV, Waugh DE (1982) Colon volvulus in the geriatric patient. Surg Clin N Am 62:249–260
Ballantyne GH (1982) Review of sigmoid volvulus. History and results of treatment. Dis Colon Rectum 25:494–501
Ballantyne GH (1982) Review of sigmoid volvulus: clinical pattern and pathogenesis. Dis Colon Rectum 25:823–830
Ballantyne GH, Brandner MD, Beart RW et al (1985) Volvulus of the colon. Incidence and mortality. Ann Surg 202:83–92
Bassey DE (1993) Radiological observations in the colon of Nigerians with chronic enema abuse. East Afr Med J 70:452–454
Bhatnagar BN, Sharma CL, Gupta SN et al (2004) Study on the anatomical dimensions of the human sigmoid colon. Clin Anat 17:236–243
Bhuiyan MMZU, Machowski ZA, Linyama BS et al (2005) Management of sigmoid volvulus in Polokwane-Mankweng hospital. S Afr J Surg 43:17–19
Boon JM, Shinners B, Meiring JH (2001) Variations of the position of the colon as applied to percutaneous nephrostomy. Surg Radiol Anat 23:421–425
Bruusgard C (1947) Volvulus of the sigmoid colon. Surgery 22:466–478
Burkitt D (1981) No relation of sigmoid volvulus to fibre content of African diet. N Engl J Med 304:914
Degiannis E, Levy RD, Sliwa K et al (1996) Volvulus of the sigmoid colon at Baragwanath Hospital. S Afr J Surg 34:25–28
El Masri SH (1987) Volvulus. In: Adeloye A (ed) Davey’s companion of surgery in Africa. Churchill Livingstone, Edinburgh, pp 335–348
Faranisi CT (1990) An approach to the management of volvulus of the sigmoid colon. Central Afr J Med 36:31–33
Faure JP, Chansigaud JP, Scepi M et al (2001) A prospective radiological anatomical study of the variations of the position of the colon in the left pararenal space. Surg Radiol Anat 23:335–339
Gibney EJ (1991) Volvulus of the sigmoid colon. Surg Gynecol Obstet 173:243–255
Hanson ME, Pickhardt PJ, Kim DH et al (2007) Anatomic factors predictive of incomplete colonoscopy based on findings at CT colonography. Am J Roentgenol 189:774–779
Kerry RL, Ransom HK (1980) Volvulus of the colon. Arch Surg 99:215–222
Manzini VT, Quazi MA, Govindasamy V et al (2006) Sigmoid volvulus in KwaZulu-Natal Teaching Hospitals: Preliminary results. S Afr Med J 96:732
Mokoena TR, Madiba TE (1995) Sigmoid volvulus among Africans in Durban. Trop Geograph Med 47:216–217
Reilly PMJ, Jones B, Bulkley GB (1992) Volvulus of the colon. In: Cameron JL (ed) Current surgical therapy. Decker Inc, St Louis, pp 170–174
Riedl P (1978) Radiological morphology of the sigmoid colon in the Ethiopian population with reference to the occurrence of volvulus. East Afr Med J 55:470–476
Sadahiro S, Ohmura T, Yamada Y et al (1992) Analysis of length and surface area of each segment of the large intestine according to age, sex, and physique. Surg Radiol Anat 14:451–457
Saunders BP, Fukumoto M, Halligan S et al (1996) Why is colonoscopy more difficult in women? Gastrointest Endosc 43:124–126
Schagen van Leeuwen JH (1985) Sigmoid volvulus in a West African population. Dis Colon Rectum 28:712–716
Segal I (1985) The effects of westernisation on sigmoid volvulus. Trop Gastroenterol 6:4–9
Sroujieh AS, Farah GR, Jabaiti SK et al (1992) Volvulus of the sigmoid colon in Jordan. Dis Colon Rectum 35:64–68
Tan CK (1972) Observations on some anomalies of the sigmoid colon. Singapore Med J 13:146–150
Tegegne A (1995) Cultural bowel patterns and sex differences in sigmoid volvulus morbidity in an Ethiopian hospital. Trop Geograph Med 47:212–215
Wapnick S, Mufundi F, Musengesi L (1975) Aetiological factors related to intestinal obstruction. Central Afr J Med 21:53–57
Williams PL, Warwick R, Dyson M et al (1989) The large intestine. In: Williams PL, Warwick R, Dyson M et al (eds) Gray’s anatomy. Churchill Livingstone, Edinburgh, pp 1365–1376
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Madiba, T.E., Haffajee, M.R. & Sikhosana, M.H. Radiological anatomy of the sigmoid colon. Surg Radiol Anat 30, 409–415 (2008). https://doi.org/10.1007/s00276-008-0344-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-008-0344-3