
Abstract
Manual compression (MC) is a well-established technique for haemostasis following percutaneous arterial intervention. However, MC is labour and time intensive with potential limitations, particularly for patients who are coagulopathic, unable to comply with bed rest or obese and when large sheaths or anti-coagulants are used. There are a variety of vascular closure devices (VCDs) available to overcome these limitations. This review gives an overview of current VCDs, their mechanism of action, individual strengths and weaknesses, evidence base and utility in interventional radiology (IR) practice. The majority of the published evidence on VCDs is derived from patients undergoing cardiac interventions, which should be borne in mind when considering the applicability and transfer of this data for general IR practice. Overall, the evidence suggests that most VCDs are effective in achieving haemostasis with a similar rate of complications to MC although the complication profile associated with VCDs is distinct to that of MC. There is insufficient evidence to comparatively analyse the different types of VCDs currently available or reliably judge their cost-effectiveness. The interventional radiologist should have a thorough understanding of the available techniques for haemostasis and be able to identify and utilise the most appropriate strategy and closure technique for the individual patient.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The traditional technique of securing haemostasis following percutaneous femoral arterial access for interventional radiology (IR) procedures has been to apply manual compression (MC) over the puncture site for approximately 10–20 min, with a subsequent period of bed rest from 4 up to 24 h depending on sheath size and coagulation status. MC is generally considered safe and has changed little since it is original description by Seldinger in 1953 [1]. Haemostasis is achieved with this technique due to the formation of a fibrin and platelet plug after blood is exposed to collagen in the arterial wall at the puncture site. The optimum duration of bed rest remains to be agreed, but published evidence suggests mobilisation at 4 h after MC for an 8F sheath and 3 h after MC for a 5F sheath may be safe [2, 3]. Haematomas related to the puncture site are the commonest complication of MC, but most are self-limited [4]. Other potential complications of MC include retroperitoneal haemorrhage, pseudoaneurysm, vessel occlusion and arteriovenous fistula formation. Approximately, 0.5–1 % of MC leads to a complication that requires further treatment, transfusion or delayed discharge [5, 6].
The major disadvantage of MC is the prolonged period of bedrest required. This is particularly challenging in patients who have difficulty complying with bedrest due to issues such as musculoskeletal complaints, orthopnoea or dementia. Longer periods of pressure or bedrest may be required and increased risks of complications with MC may arise, due to abnormal clotting, obesity, use of large sheaths, antiplatelet agents or anticoagulant administration. MC can therefore lengthen overall procedure times and increase demands for specialist staff and hospital beds [7, 8].
The drawbacks of MC led to the development and introduction of vascular closure devices (VCDs) in the 1990s. The theoretical ideal VCD is easy to use with minimal training, comfortable for patient and operator, offers secure haemostasis regardless of vessel quality, clotting parameters or sheath size and allows immediate ambulation with no short or long-term risks. Current VCD technology offers potential advantages to MC, but there is no ideal device at present, and indeed this theoretical ideal may be unattainable. VCDs also have their own potential risks and complications that are different to MC and often specific to the type of device. There are a variety of closure devices available that range in mode of action, effectiveness, risk and cost. This review aims to give an overview of current VCDs, their mechanism of action, individual strengths and weaknesses, evidence base and utility in IR practice.
Non-invasive Adjuncts to Manual Compression
There are a number of devices available as adjuncts to MC such as mechanical clamp devices and haemostatic pads. Mechanical clamp devices apply direct pressure at the puncture site and may help free up the operator earlier, but the need for careful placement over the arteriotomy for adequate haemostasis, lack of direct operator supervision over the access site to detect complications and the continued need for prolonged bedrest are major drawbacks to their use. Haemostatic pads are coated with procoagulant material to promote clotting and haemostasis but still require a degree of MC and a period of bedrest. There are two, relatively small, published randomised controlled trials (RCTs) in IR, comparing compression with haemostasis pads and compression with conventional MC [9, 10]. Mlekusch et al. [9] demonstrated only a minimal reduction in the time to haemostasis, no difference in the time to ambulation and a greater incidence of minor bleeding and complications with the use of a haemostasis pad. Balzer et al. [10] demonstrated reduced time for haemostasis and time to ambulation with the use of a haemostasis pad versus conventional MC, but they routinely applied a pressure bandage at the access site for a minimum of 2 h following compression with the haemostasis pad and overall times to haemostasis and required time for application of a pressure bandage (mean 10.15 min and 3.47 h, respectively) remained relatively high in the haemostasis pad group. Small RCTs in the cardiology literature have similarly demonstrated only small reductions in the time required for compression and no significant reduction in the time to ambulation or higher rates of technical failure with haemostasis pads compared to conventional MC [11, 12]. Overall, the utility of mechanical clamps or compression devices and haemostasis pads as adjuncts to MC are at best of modest clinical value in overcoming the major drawbacks of MC and will not be discussed further.
Classification of Vascular Closure Devices
VCDs can be classified by their design and mechanism of action for actively gaining haemostasis into three main categories: plug-based (with plug material such as collagen, polyglycolic acid or animal intestinal submucosa), suture-mediated and staple or clip-based devices. In addition, there are relatively novel and unique invasive compression assist VCDs that help achieve haemostasis without leaving any implanted foreign material. We will only discuss currently available VCDs, summarised in Table 1.
Plug-Based VCDs
Angio-Seal
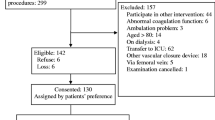
The Angio-Seal (St. Jude Medical, MN, USA) is a collagen-based VCD that is long established and one of the most widely used of all VCDs. The closure components consist of a 1 × 2 × 10 mm co-polymer anchor attached to a collagen plug by an absorbable suture (Fig. 1). The anchor remains intraluminal following deployment. Haemostasis is achieved by the dual mechanism of the closure components physically approximating to bridge the arteriotomy as well as the procoagulant effect of the swelling collagen causing platelet aggregation to aid haemostasis. All of these components are degraded by hydrolysis and are resorbed within 60 to 90 days. The Angio-Seal device is available in 6- and 8-French sheath sizes. The latest iterations of the Angio-Seal device are the Angio-Seal VIP (V-twist Integrated Platform) which provides a larger collagen footprint to conform better to the vessel by twisting down on to the arterial wall and the Angio-Seal Evolution which has an automated collagen compaction system to allow single-handed deployment and reduce deployment variability.

Diagrammatic representation of the closure components of the Angio-Seal VCD during deployment. (Reproduced with permission of St. Jude Medical)
The main drawbacks of the Angio-Seal relate to the implanted material. There is a risk that the intravascular anchor may cause luminal narrowing or foreign body reaction that could lead to vessel occlusion [23]. Repeat puncture or surgical cutdown prior to absorption of the implanted material could lead to dislodgement and distal embolisation of the intra-arterial component [24]. However, there have been reports of safe early re-access, particularly if repeat puncture is performed 1 cm distal or proximal to the original Angio-Seal deployment site [25]. There is also a risk that an inflammatory response to the collagen plug may lead to scarring and patient discomfort [26].
There have been several RCTs and observational studies published regarding this device. In an early RCT of 435 patients undergoing cardiac catheterisation, Kussmaul et al. [20] reported a high deployment success rate (96 %), significantly shorter time to haemostasis with 76 % of patients having immediate haemostasis (within 1 min) and a reduced number of complications for patients with Angio-Seal compared to MC. These findings have been supported by other RCTs in the cardiology literature with improved times to haemostasis despite anticoagulation and a lower rate of complications compared to MC [20–22]. There have been two smaller RCTs in patients undergoing peripheral vascular interventions that also demonstrated improved haemostasis times and no significant increase in the number of complications with the Angio-Seal device compared to MC [27, 28].
Mynx
The MynxGrip (AccessClosure, Inc, CA, USA) VCD is the latest generation of the Mynx VCD and works by delivering a non-biologic sealant, polyethylene glycol, to the extravascular space directly above the arteriotomy, whilst a small semi-compliant balloon is temporarily inflated inside the vessel against the wall for haemostasis (Fig. 2). The sealant does not directly promote clotting but conforms to the arteriotomy and expands on contact with fluid and blood products to seal the vessel. The polyethylene glycol sealant is degraded by hydrolysis and is completely resorbed by the body within 30 days. The MynxGrip device is available in 5- and 6/7-French sizes and is deployed through the procedure sheath. There is a Mynx Ace version of the device that utilises the same extravascular MynxGrip sealant but is delivered via its own 7-French delivery sheath. A non-randomised single-arm prospective trial of 190 patients undergoing diagnostic and interventional cardiac catheterisation and closure with the Mynx device resulted in successful deployment in 93 % of cases with a mean time to haemostasis and time to ambulation of 1.3 min and 2.6 h, respectively [29].

Deployment of the MynxGrip. A small balloon is inflated within the vessel for temporary hemostasis (A). Extravascular polyethylene glycol sealant is delivered (B). The sealant conforms to the arteriotomy surface to seal the vessel (C). (Images reproduced with permission of AccessClosure, Inc.)
The primary advantage of the Mynx VCD is the intended absence of intraluminal material, thereby reducing the risks of luminal narrowing, vessel occlusion or distal embolisation. However, there are reports of distal embolisation occurring with the Mynx VCD [30, 31]. In one single-centre retrospective series of cardiac interventions in 238 patients with the original Mynx device and 190 patients with the Angio-Seal device, there was no difference in the rate of access-related major vascular complications in both groups (2.1 %), but there was a higher rate of device failure in the Mynx cohort (9.2 %) compared to the Angio-Seal cohort (3.7 %) [32]. However, it should be noted that the Mynx device has undergone four further iterations with device improvements since this early comparative report. Safe repeat puncture and access of the vessel following closure with a Mynx VCD have been described in an animal model with no evidence of sealant prolapse or embolisation [33], but there is no clinical experience published regarding this at present.
Exoseal
The Exoseal (Cordis Corp., NJ, USA) VCD achieves haemostasis by deploying an extravascular polyglycolic acid plug directly over the arteriotomy. The Exoseal delivery device has a visual marker that indicates the intended site of placement just outside the vessel (Fig. 3). The polygolic acid plug is hydrolysed and resorbed within 60–90 days. The Exoseal is available in 5- to 7-French sheath sizes and is deployed via the existing procedure sheath as long as it is no longer then 12 cm. Two minutes of non-occlusive MC is advised following deployment, and ambulation is proposed by the manufacturers at 6 h or later. The Exoseal also has the potential advantage of not having an intravascular implant thereby diminishing the risks of anchor-related luminal narrowing, occlusion or embolism.

Deployment of the Exoseal. The Exoseal device is inserted via the existing procedural sheath (A). A visual display on the Exoseal device indicates that the intended site of deployment as the device and sheath is slowly withdrawn from the arteriotomy (B). The extravascular polyglycolic acid plug is deployed over the arteriotomy site for haemostasis (C). (Images reproduced with permission of Cordis Corp.)
The ECLIPSE trial was a multi-centre RCT of 401 patients undergoing diagnostic or interventional cardiovascular procedures randomised to closure with Exoseal or MC [34]. Mean time to haemostasis and time to ambulation were significantly shorter in the Exoseal arm of the study (4.4 vs 20.1 min and 2.5 vs 6.2 h, respectively), and there were no major complications reported in this study [34]. It should be noted that this trial, like many pre-approval studies, excluded patients with femoral arterial disease, moderate calcifications at the site of sheath insertion and those with a history of recent femoral artery access. The rate of procedural technical success in the Exoseal arm of this trial was 91.8 % [34]. In a single-centre prospective non-randomised series, the Exoseal was evaluated in the closure of 100 antegrade femoral artery punctures in 93 patients undergoing peripheral vascular intervention [35]. The reported rate of technical success in this series was 96.0 %. The Exoseal could not be deployed in one case due to kinking of the vascular sheath introducer and in three cases because the bio-absorbable plug was not properly delivered to the extravascular space adjacent to the arterial puncture, but instead fully removed with the delivery system [35]. Minor vascular complications were found in seven cases (7.0 %), with four cases (4.0 %) of pseudoaneurysm and three cases (3.0 %) of significant late bleeding, none of which required surgery, and there were no major adverse events in this series [35]. In a similar smaller series of antegrade femoral closure with the Exoseal device in 59 patients, the reported success rate was high (98.3 %), and access vessel calcification, BMI or clotting did not significantly influence adverse events in this small series [65].
FISH
The Femoral Introducer Sheath and Haemostasis (FISH) VCD (Morris Innovative Inc., IN, USA) achieves haemostasis by placement of a ribbon of porcine-derived small intestine submucosa (SIS) attached to a cuff within the vessel wall at the arteriotomy site (Fig. 4). The SIS patch is an extracellular matrix that acts as a bio-scaffold promoting remodelling of the vessel wall leaving behind only natural organised tissue. The implanted intravascular plug is absorbed within 30 days. The FISH device is unique because it utilises SIS and also because it is delivered pre-mounted on a sheath for vascular access during the procedure. The FISH VCD is available in sheath sizes of 5- to 8-French. The intravascular component is very pliable potentially allowing for closure in small or diseased vessels, but this remains to be proven in published clinical practice.

Deployment of the FISH device. The small intestinal submucosa (SIS) ribbon is pre-mounted on a vascular access sheath (A). The SIS ribbon forms a plug in the artery wall when this is deployed as the sheath is withdrawn (B). The resorbable SIS plug remains deployed across the arteriotomy for haemostasis (C). (Images reproduced with permission of Morris Innovative Inc.)
In a multi-centre RCT of 297 patients undergoing diagnostic coronary intervention randomised to FISH or MC, mean time to haemostasis and mean time to ambulation were reduced for the FISH cohort compared to MC (8.9 vs 17.2 min and 2.4 vs 4.3 h, respectively), and there were no significant differences in the rates of adverse events between the two cohorts in this study [64]. However, it is notable that 27 (14.1 %) patients randomised to FISH were converted to MC due to anticipated suboptimal haemostasis [64]. Further published data regarding the efficacy and safety of the FISH VCD, particularly in patients undergoing IR procedures, are awaited.
Suture-Mediated Closure Devices
Suture-mediated closure devices (SMCDs) work by deploying a pair of needles on either side of the arteriotomy to enable a suture to be placed which can be pulled and tied to mechanically close the arteriotomy. There have been several examples and iterations of SMCDs in the past that work on a similar basis. We will present the two most widely available SMCDs.
Perclose Proglide
The Perclose Proglide (Abbott Vascular, IL, USA) delivers a single pre-tied non-biodegradable monofilament polypropylene suture to close the arteriotomy (Fig. 5). It is the latest version of the Perclose SMCD and is licensed in the closure of sheath sizes from 5-French to 21-French. Sheath sizes greater then 8-French require at least two devices using the pre-close technique which has been well described in the literature to successfully close larger arteriotomies, particularly in the setting of endovascular aneurysm repair [13–15]. With this technique, two Perclose Proglide devices are pre-deployed at the same access site at the beginning of the procedure before the arteriotomy is dilated beyond 8-French. Each device is pre-deployed and angled 30°–60° from the anterior midline in opposite directions, and the sutures are left untied during the procedure. Following completion of the procedure, the sheath is removed over a wire, whilst the pre-deployed sutures are tensioned. The advantage of this pre-close technique is that large sheath sizes can be closed percutaneously, and a guide wire can be retained during tensioning of the sutures to allow insertion of a further VCD or temporary sheath to stop bleeding in the event of unsatisfactory haemostasis.

Diagram demonstrating Perclose Proglide device needles being deployed from the device through the artery wall to the footplate. The needles engage the suture, and the plunger is then withdrawn, which draws the suture out through the proximal part of the device. The lever is then lowered so the device can be partially withdrawn, and the suture/knot combination can be pulled free. The device is removed, and the slip part of the knot can then be pulled tight to secure the arteriotomy. (Images provided courtesy of Abbott Vascular)
Prostar XL
The Prostar XL device (Abbott Vascular, IL, USA) is indicated for the closure of 8.5 to 10-French sheath common femoral artery access sites, but as with the Perclose Proglide, larger sheath sizes up to 24-French have been closed successfully using the pre-close technique although only one Prostar XL device is required as each Prostar XL delivers two sutures. Also in contrast to the Perclose Proglide, the Prostar XL device is larger, measuring 10-French, and the sutures are braided polyester and not pre-tied.
The Prostar XL also allows the guidewire to be retained whilst tying the sutures which can be advantageous. There is no limitation regarding repeat vessel puncture at the same site following use of an SMCD. However, the drawbacks of this device and SMCDs generally are that there are a greater number of procedural steps which increase the complexity of the VCD and introduce a potentially longer learning curve.
There are several RCTs and observational series published that generally support the use of the Perclose and Prostar SMCDs. Large observational series and RCTs comparing these devices to MC have demonstrated high rates of achieving haemostasis with SMCDs ranging from 85.7 to 99 % as well as significantly reduced times to haemostasis and ambulation post-procedure in diagnostic and interventional cardiology cases with no significant increase in the rate of complications [36–38]. In one RCT, within the diagnostic cardiology cohort, there were significantly fewer vascular complications with the use of a Perclose device compared to MC [36]. There is a potential risk of infection related to the implanted suture material, and in one series, the infection rate was 0.5 % [38]. There is a large observational series of Perclose use in 930 patients with peripheral arterial disease which also demonstrated a high rate of technical success (92.2 %), permitting early ambulation despite being fully anticoagulated following intervention, although there was a 7.0 % incidence of groin-related complications, all patients were free of local symptoms at 30-day follow-up [39].
Clip-Based VCD
StarClose
The StarClose SE (Abbott Vascular, IL, USA) achieves vessel closure by placement of a 4-mm disc-shaped nitinol clip on the outside of the vessel wall (Fig. 6). The StarClose is designed for closure of 5- to 6-French sheath sizes. The main advantage of the StarClose is that there is no implanted intraluminal material. However, a theoretical disadvantage is that there is a residual permanent metal implant.

Deployment of the StarClose device. The device is inserted via a sheath, the locator button is depressed, and the device is withdrawn until resistance is felt (A). The thumb advancer splits the delivery sheath (B). The device angle is raised (C), and the clip is deployed to seal the arteriotomy (D). (Images provided courtesy of Abbott Vascular)
The CLIP trial was an RCT of 596 patients undergoing diagnostic and interventional coronary interventions randomised to closure with StarClose or MC [40, 41]. Device success was achieved in 94.1 % of diagnostic cases and 86.8 % of interventional cases. StarClose resulted in significantly reduced times to haemostasis and ambulation (1.5 vs 15.5 and 163 vs 269 min, respectively) in the diagnostic group with no significant differences in the rates of complications compared to MC [40]. In the interventional group, there was a significantly reduced time to haemostasis (8 vs 29 min), but no significant reduction in the time to ambulation compared to MC and no differences in the rates of complications compared to MC [41]. There were no reports of infection related to the implanted device in the CLIP trials. Isolated case reports of StarClose clip embolisation have been described [42].
There is a published observational series of 222 patients with peripheral arterial disease who underwent StarClose closure following diagnostic or therapeutic IR procedures [43]. Immediate haemostasis was achieved in 96 % of patients in this cohort, and there were no major complications although there was a reported 8 % incidence of a small haematoma and a 3 % incidence of minor bleeding that settled spontaneously at the time of closure [43].
Invasive Compression Assist Devices
This is a relatively novel group of VCD that achieves haemostasis without any retained or implanted material, offering the potential advantage of eliminating the risks of embolisation, occlusion or infection related to the implanted material. However, the disadvantage of this type of VCD is that there is a continued need for a degree of MC although the time required for this may be reduced.
Axera
The Axera (Arstasis, CA, USA) device creates an ultra-low angle vascular access channel, approximately 5°–10°, at the beginning of the procedure through which a 5 or 6-French sheath can be inserted (Fig. 7). The shallower angle of access results in increased arterial wall overlap with tract compression due to the radial pressure of flowing blood applied to the vessel wall. Essentially, this device helps create a ‘self-sealing’ arteriotomy puncture. MC is still required after sheath removal but for a reduced duration of time. The major advantage of this device is that there is no implanted material. At present, there is little published evidence of clinical experience with this device only in coronary and neurovascular procedures, but with wider commercial availability this may increase [16, 17]. In a single-centre retrospective study of 94 patients undergoing neurovascular procedures with 5- to 6-French sheaths, the median time to haemostasis with compression was 4 min; all patients were allowed to ambulate at 1 h, and there was a complication rate of 3 % (1 local haematoma and 2 failed procedures) [17].

Deployment of the Axera device. Following a standard micropuncture vessel access, the deployment device is inserted. A needle is deployed that travels in an ultra-low angle across the vessel wall (A). A guidewire is then placed through that needle, and the assembly is withdrawn. A sheath is then placed through this ultra-low angle access (B). At the end of the procedure, the sheath is withdrawn, and hydrostatic pressure facilitates hemostasis (C). (Images reproduced with permission of Arstasis)
Catalyst
The Catalyst II and Catalyst III (Cardiva Medical Inc., CA, USA) are the latest generations of the Boomerang VCD (Cardiva Medical Inc., CA, USA). This device is indicated to close 5- to 7-French sheath sizes and utilises a deployable nitinol mesh disc on an 18-gauge wire inserted through the access sheath at the end of the procedure (Fig. 8). The nitinol disc provides temporary haemostasis, whilst the wire is fixed externally to allow the arteriotomy to recoil to the size of the 18-gauge wire. The minimum recommended dwell time for the fixed nitinol disc is 15 min for diagnostic and 120 min for interventional cases after which the disc is collapsed and removed with MC applied to achieve final haemostasis. The Catalyst II has a proprietary haemostatic coating on the wire to help achieve haemostasis, and the Catalyst III also has an additional protamine sulphate coating for use in heparinised patients. The advantages of this device are that there is no permanent implant and there appears to be little anatomical constraint on its use with some evidence of utilisation in patients with peripheral vascular disease and in the paediatric population although this is outside of the manufacturer’s standard indication for use [18, 19]. The disadvantages of this device appear to be the prolonged device dwell times, the potential to disturb the haemostatic plug as the collapsed disc passes through the arteriotomy and percutaneous tract after the dwell time and also the continued need for MC.

The Catalyst III disc is deployed inside the lumen of the artery to enhance the vessel wall’s elastic recoil and tissue apposition. Coagulation is also aided by the haemostatic coating of the extravascular part of the device. The disc is later folded and removed through the arteriotomy as haemostasis is supported by manual compression. (Images reproduced with permission of Cardiva Medical Inc.)
There is also little published clinical experience with this device. In an observational study of the Boomerang VCD in 96 patients undergoing diagnostic cardiac catheterisation, the device was successfully deployed and haemostasis achieved in 99 % of patients; patients were ambulated at a mean time of 82 min (1 h after haemostasis was achieved), and there was a minor complication rate of 5 %, but there were no major complications [18].
Evidence in IR
When reviewing the presented device-specific evidence, it is important to bear in mind there are several significant limitations to these trials and studies that may preclude direct transfer and applicability of this data to general IR settings:
-
(1)
Many of the studies excluded patients that would be considered high risk such as those with femoral artery calcification, coagulopathy, prior access or scarring.
-
(2)
The majority of the trials were performed in patients undergoing diagnostic or routine cardiac intervention with sheath sizes smaller then 8-French.
-
(3)
Enrolment numbers were generally low and as such the studies were underpowered to detect serious but uncommon device-related complications.
-
(4)
Definitions of success and what constitutes minor and major complications are not universal or standardised and make comparisons between studies difficult.
-
(5)
Some of the trials are single-arm non-randomised, whilst in the majority of the RCTs, comparison of the VCD was made to MC and not other available VCDs.
In view of the above limitations, evidence from registries and metaanalyses are of increased importance. The majority of these are again published in the Cardiology literature with the notable exceptions of a dedicated metaanalysis of VCDs in IR and a European IR registry of Angio-Seal use [43, 44]. The results of the metanalysis of VCDs in IR by Das et al. [43] were similar to those of the main large cardiology metaanalyses and demonstrated a non-significant trend towards fewer complications with VCDs but no statistically significant difference in the rates of complications with pooled VCDs and MC. In the multi-national European registry of 1107 IR patients undergoing closure with Angio-Seal, there was a high reported technical success rate of 97.2 % and a low complication rate of 2.4 %, of which half were reported as serious (1.2 %) [44]. There is insufficient published evidence to favour a specific VCD [43, 46]. This may be because few studies have compared different types of VCDs and also because differences between individual VCDs are subtle, and therefore large comparative trials are required to demonstrate statistically significant differences [43, 46].
Complications
It is important to note that whilst there is a generally similar published rate of complications related to VCDs and MC overall, there is a differing profile of complications for individual VCDs. Complications of MC such as haematoma, continued bleeding, vessel thrombosis, arteriovenous fistula and pseudoaneurysm formation are well recognised. The use of VCDs introduces the potential for novel complications such as infection of implanted material, distal embolisation of device components, luminal narrowing or distortion and foreign body reactions [24, 30–32, 38, 45]. There may also be potential complications due to attempted early repeat access following VCD deployment with certain devices. Recently published Society of Interventional Radiology (SIR) guidelines regarding the use of VCDs recommend that institutional complication rates for VCD use should be less than or equal to that of MC with a threshold acceptable rate of 3 % for major complications [46]. These guidelines also recommend that femoral angiography be routinely considered prior to deployment of VCDs to exclude patients with suboptimal access sites, thereby reducing VCD-related complications [46].
Non-standard Places for VCDs
The vast majority of published data and VCD ‘indications for use’ apply to retrograde access of the common femoral artery (CFA). There are successful reports of VCD use in antegrade access [35, 44]. In a European IR registry report, whilst Angio-Seal deployment failure was not significantly related to calcification or peripheral vascular disease at the access site, there was a significantly higher rate of deployment failure for antegrade punctures compared to retrograde punctures (8.8 and 1.8 %, respectively).
The application of VCDs in the brachial and popliteal arteries is more challenging due to the smaller calibre of these vessels, which are more prone to spasm and thrombosis compared to the CFA. There are two large series of successful brachial artery closure with the Angio-Seal device in selected patients undergoing cardiac intervention [47, 48]. Belenky et al. reported 100 % technical success rate, and no major complications at 64 brachial access sites with a minimum diameter greater than 4mm closed with an Angio-Seal [48]. Lupatelli et al. [47] reported a technical success rate of 96.9 %, and a major complication rate of 3.1 % with Angio-Seal deployed in 161 brachial access sites that were considered to be of adequate size and free from significant calcification. Successful closure of brachial access sites has been reported in smaller case series with Perclose SMCDs, StarClose and Exoseal VCDs [49–51]. Similarly, popliteal artery access sites have also been successfully closed with StarClose and Angio-Seal VCDs in small case series [52, 53].
There is a risk of inadvertent arterial cannulation during intended central venous access, particularly when performed without ultrasound guidance or adequate training, and there are a number of case reports describing salvage closure with Angio-Seal, Perclose and StarClose VCDs in these cases [54–58]. There have even been cases of successful extreme salvage closure reported with Angio-Seal use in the descending aorta and right ventricle following iatrogenic injury [59, 60].
Cost-Effectiveness
VCDs add a further device cost to the procedure compared to MC. This cost could potentially be offset if there is a demonstrable reduction in complications, reduced hospital stay or increased departmental throughput. There are a few studies based on coronary procedures that have demonstrated cost advantages of VCDs [61–63]. However, these studies do not all consider the cost implications of VCD-related complications or are based on a lower rate of complications with VCD use compared to MC that has not been universally demonstrated. There is inadequate evidence for an overall cost advantage of VCD use in IR practice, and guidelines suggest that VCDs should not be used for the explicit purposes of cost reduction [43, 46].
Conclusion
A wide variety of VCDs are available to the interventional radiologist with evidence to suggest that VCD use is generally effective in achieving haemostasis with a similar rate of complications to MC. The types of complications associated with VCDs are generally distinct to those of MC and often unique to the type of VCD. The group of patients for whom the use of VCDs should be strongly considered are those who are high risk for MC (for example, due to abnormal clotting, obesity or being unable to comply with bed rest) but with access vessels of adequate diameter and quality for VCD use. There is insufficient evidence at present to comparatively analyse the different types of VCDs or judge their cost-effectiveness. The majority of the published evidence is derived from coronary procedures in relatively small studies that may not reflect the procedures performed or population served by the interventional radiologist. There is a need for further detailed study of VCDs in IR to establish their efficacy, safety and cost-effectiveness. The interventional radiologist should have a thorough understanding of the range of techniques available for haemostasis and be able to identify and utilise the most appropriate device and strategy best suited to the individual patient.
References
Seldinger SI. Catheter replacement of the needle in percutaneous arteriography. Acta Radiol. 1953;39:366–76.
Bogart MA, Bogart DB, Rigden LB, et al. A prospective randomized trial of early ambulation following 8 French diagnostic cardiac catheterization. Catheter Cardiovasc Interv. 1999;47:175–8.
Steffenino G, Dellavalle A, Ribichini F, et al. Ambulation three hours after elective cardiac catheterization through the femoral artery. Heart. 1996;75:477–80.
Babu SC, Piccorelli GO, Shah PM, et al. Incidence and results of arterial complications among 16,350 patients undergoing cardiac catheterization. J Vasc Surg. 1989;10:113–6.
McGraw J, et al. Society of interventional radiology quality improvement guidelines for diagnostic arteriography. J Vasc Interv Radiol. 2003;14:S283–8.
The British Society of Interventional Radiology. Third BIAS Report 2008. Oxfordshire: Dendrite Clinical Systems; 2008.
Ten Silber S. years of arterial closure devices: a critical analysis of their use after PTCA. Z Kardiol. 2000;89(5):383–9.
Koreny M, Riedmuller E, Nikfardjam M, et al. Arterial puncture closing devices compared with standard manual compression after cardiac catheterization: systematic review and meta-analysis. JAMA. 2004;291:350–7.
Mlekusch W, Minar E, Dick P, et al. Access site management after peripheral percutaneous transluminal procedures: neptune pad compared with conventional manual compression. Radiology. 2008;249(3):1058–63.
Balzer JO, Schwarz W, Thalhammer A, et al. Postinterventional percutaneous closure of femoral artery access sites using the Clo-Sur PAD device: initial findings. Eur Radiol. 2007;17(3):693–700.
Nguyen N, Hasan S, Caufield L, et al. Randomized controlled trial of topical hemostasis pad use for achieving vascular hemostasis following percutaneous coronary intervention. Catheter Cardiovasc Interv. 2007;69(6):801–7.
Mlekusch W, Dick P, Haumer M, et al. Arterial puncture site management after percutaneous transluminal procedures using a hemostatic wound dressing (Clo-Sur P.A.D.) versus conventional manual compression: a randomized controlled trial. J Endovasc Ther. 2006;13(1):23–31.
Lee WA, Brown M, Nelson PR, Huber TS. Total percutaneous access for endovascular aortic aneurysm repair (“Preclose” technique). J Vasc Surg. 2007;45(6):1095–101.
Dosluoglu HH, Cherr GS, Harris LM, Dryjski ML. Total percutaneous endovascular repair of abdominal aortic aneurysms using Perclose ProGlide closure devices. J Endovasc Ther. 2007;14(2):184e8.
Lee WA, Brown MP, Nelson PR, Huber TS, Seeger JM. Midterm outcomes of femoral arteries after percutaneous endovascular aortic repair using the Preclose technique. J Vasc Surg. 2008;47(5):919e23.
Turi ZG, Wortham DC, Sampognaro GC, et al. Use of a novel access technology for femoral artery catheterization: results of the RECITAL trial. J Invasive Cardiol. 2013;25(1):13–8.
Fortes MC, Jindal G, Polifka AJ, et al. Low-angle vascular access for neurovascular procedures using the Arstasis AXERA access device. J Vasc Interv Radiol. 2013;24:693–7.
Doyle BJ, Godfrey MJ, Lennon RJ, et al. Initial experience with the Cardiva Boomerang vascular closure device in diagnostic catheterization. Catheter Cardiovasc Interv. 2007;69(2):203–8.
Seltzer S, Alejos JC, Levi DS. Experience with the cardiva boomerang catalyst system in pediatric cardiac catheterization. Catheter Cardiovasc Interv. 2009;74(3):476–81.
Kussmaul WG, Buchbinder M, Whitlow PL, et al. Rapid arterial hemostasis and decreased access site complications after cardiac catheterization and angioplasty: results of a randomized trial of a novel hemostatic device. J Am Coll Cardiol. 1995;25:1685–92.
Chevalier B, Lancelin B, Koning R, et al. Effect of a closure device on complication rates in high-local-risk patients: results of a randomized multicenter trial. Cathet Cardiovasc Interv. 2003;58:285–91.
Applegate RJ, Grabarczyk MA, Little WC, et al. Vascular closure devices in patients treated with anticoagulation and IIb/IIIa receptor inhibitors during percutaneous revascularization. J Am Coll Cardiol. 2002;40:78–83.
Eidt JF, Habibipour S, Saucedo JF, et al. Surgical complications from hemostatic puncture closure devices. Am J Surg. 1999;178:511–6.
Adusumilli S, Mah J, Richardson A. Acute leg ischemia secondary to embolization of an Angio-Seal device. Diagn Interv Radiol. 2011;17:98–100.
Applegate RJ, Rankin KM, Little WC, Kahl FR, Kutcher MA. Restick following initial Angioseal use. Cathet Cardiovasc Interv. 2003;58:181–4.
Gargiulo NJ 3rd, Veith FJ, Ohki T, et al. Histologic and duplex comparison of the perclose and angio-seal percutaneous closure devices. Vascular. 2007;15(1):24–9.
Beyer-Enke SA, Söldner J, Zeitler E. Immediate sealing of arterial puncture site following femoropopliteal angioplasty: a prospective randomized trial. Cardiovasc Interv Radiol. 1996;19:406–10.
Upponi SS, Ganeshan AG, Warakaulle DR, et al. Angioseal versus manual compression for haemostasis following peripheral vascular diagnostic and interventional procedures—a randomized controlled trial. Eur J Radiol. 2007;61:332–4.
Scheinert D, Sievert H, Turco MA, et al. The safety and efficacy of an extravascular, water-soluble sealant for vascular closure: initial clinical results for Mynx. Cathet Cardiovasc Interv. 2007;70:627–33.
Islam MA, George AK, Norris M. Popliteal artery embolization with the Mynx closure device. Cathet Cardiovasc Interv. 2010;75:35–7.
Rao S, Kaul P, Stouffer GA. Successful aspiration of Mynx vascular closure device sealant that embolized to the popliteal artery. J Invasive Cardiol. 2013;25(8):E172–4.
Azmoon S, Pucillo AL, Aronow WS, et al. Vascular complications after percutaneous coronary intervention following hemostasis with the Mynx vascular closure device versus the AngioSeal vascular closure device. J Invasive Cardiol. 2010;22(4):175–8.
Garasic JM, Marin L, Anderson RD. Acute evaluation of the Mynx vascular closure device during arterial re-puncture in an ovine model. J Invasive Cardiol. 2009;21(6):283–5.
Wong SC, Bachinsky W, Cambier P, et al. A randomized comparison of a novel bioabsorbable vascular closure device versus manual compression in the achievement of hemostasis after percutaneous femoral procedures: the ECLIPSE (Ensure’s Vascular Closure Device Speeds Hemostasis Trial). JACC Cardiovasc Interv. 2009;2:785–93.
Schmelter C, Liebl A, Poullos N, Ruppert V, Vorwerk D. Suitability of Exoseal vascular closure device for antegrade femoral artery puncture site closure. Cardiovasc Interv Radiol. 2013;36(3):659–68.
Gerckens U, Cattelaens N, Lampe EG, Grube E. Management of arterial puncture site after catheterization procedures: evaluating a suture-mediated closure device. Am J Cardiol. 1999;83:1658–63.
Baim DS, Knopf WD, Hinohara T, et al. Suture-mediated closure of the femoral access site after cardiac catheterization: results of the suture to ambulate and discharge (STAND I and STAND II) trials. Am J Cardiol. 2000;85:864–9.
Fram DB, Giri S, Jamil G, et al. Suture closure of the femoral arteriotomy following invasive cardiac procedures: a detailed analysis of efficacy, complications, and the impact of early ambulation in 1200 consecutive, unselected cases. Cathet Cardiovasc Interv. 2001;53:163–73.
Balzer JO, Scheinert D, Diebold T, et al. Postinterventional transcutaneous suture of femoral artery access sites in patients with peripheral arterial occlusive disease: a study of 930 patients. Cathet Cardiovasc Interv. 2001;53:174–81.
Hermiller J, Simonton C, Hinohara T, et al. Clinical experience with a circumferential clip-based vascular closure device in diagnostic catheter- ization. J Invas Cardiol. 2005;17:504–10.
Hermiller JB, Simonton C, Hinohara T, et al. The StarClose Vascular Closure System: interventional results from the CLIP study. Cathet Cardiovasc Interv. 2006;68:677–83.
Stock U, Flach P, Gross M, et al. Intravascular misplacement of an extravascular closure system: StarClose. J Interv Cardiol. 2006;19:170–2.
Das R, Ahmed K, Athanasiou T, Morgan RA, Belli AM. Arterial closure devices versus manual compression for femoral haemostasis in interven- tional radiological procedures: a systematic review and meta-analysis. Cardiovasc Interv Radiol. 2011;34:723–38.
Reekers JA, Müller-Hülsbeck S, Libicher M, et al. CIRSE vascular closure device registry. Cardiovasc Interv Radiol. 2011;34:50–3.
Sohail MR, Khan AH, Holmes DR, et al. Infectious complications of percutaneous vascular closure devices. Mayo Clin Proc. 2005;80:1011–5.
Sheth RA, Walker TG, Saad WE, et al. Quality improvement guidelines for vascular access and closure device use. J Vasc Interv Radiol. 2014;25:73–84.
Lupattelli T, Clerissi J, Clerici G, et al. The efficacy and safety of closure of brachial access using the AngioSeal closure device: experience with 161 interventions in diabetic patients with critical limb ischemia. J Vasc Surg. 2008;47:782–8.
Belenky A, Aranovich D, Greif F, et al. Use of a collagen-based device for closure of low brachial artery punctures. Cardiovasc Interv Radiol. 2007;30:273–5.
Kim A, Fusman B, Jolly N, Feldman T. Percutaneous suture closure for brachial artery puncture. J Interv Cardiol. 2002;15(4):277–80.
Puggioni A, Boesmans E, Deloose K, et al. Use of StarClose for brachial artery closure after percutaneous endovascular interventions. Vascular. 2008;16(2):85–90.
Pieper CC, Wilhelm KE, Schild HH, Meyer C. Feasibility of vascular access closure in arteries other than the common femoral artery using the ExoSeal vascular closure device. Cardiovasc Interv Radiol. 2014;37:1352–7.
Noory E, Rastan A, Sixt S, et al. Arterial puncture closure using a clip device after transpopliteal retrograde approach for recanalization of the superficial femoral artery. J Endovasc Ther. 2008;15(3):310–4.
Henry M, Amor M, Allaoui M, et al. A new access site management tool: the Angio-Seal hemostatic puncture closure device. J Endovasc Surg. 1995;2(3):289–96.
Railo M, Roth W-D. The use of a collagen-based puncture closure device in the subclavian artery after inadvertent introduction of an 11.5 French hemodialysis catheter. Cardiovasc Interv Radiol. 2004;27(6):681–2.
Szkup PL. A minimally invasive technique for closing an iatrogenic subclavian artery cannulation using the Angio-Seal closure device: two case reports. J Med Case Rep. 2012;6(1):82.
Fraizer MC, Chu WW, Gudjonsson T, Wolff MR. Use of a percutaneous vascular suture device for closure of an inadvertent subclavian artery puncture. Catheter Cardiovasc Interv. 2003;59(3):369–71.
Tran V, Shiferson A, Hingorani AP, et al. Use of the StarClose device for closure of inadvertent subclavian artery punctures. Ann Vasc Surg. 2009;23(5):688.
Nicholson T, Ettles D, Robinson G. Managing inadvertent arterial catheterization during central venous access procedures. Cardiovasc Interv Radiol. 2004;27(1):21–5.
Hatfield MK, Zaleski GX, Kozlov D, et al. Angio-seal device used for hemostasis in the descending aorta. AJR Am J Roentgenol. 2004;183(3):612–4.
Petrov I, Dimitrov C. Closing of a right ventricle perforation with a vascular closure device. Catheter Cardiovasc Interv. 2009;74(2):247–50.
Rickli H, Unterweger M, Sütsch G, et al. Comparison of costs and safety of a suture-mediated closure device with conventional manual compression after coronary artery interventions. Cathet Cardiovasc Interv. 2002;57:297–302.
Slaughter PM, Chetty R, Flintoft VF, et al. A single center randomized trial assessing use of a vascular hemostasis device vs. conventional manual compression following PTCA: what are the potential resource savings? Cathet Cardiovasc Diagn. 1995;34:210–4.
Resnic FS, Arora N, Matheny M, Reynolds MR. A cost-minimization analysis of the angio-seal vascular closure device following percutaneous coronary intervention. Am J Cardiol. 2007;99(6):766–70.
Bavry AA, Raymond RE, Bhatt DL, et al. Efficacy of a novel procedure sheath and closure device during diagnostic catheterization: the multicenter randomized clinical trial of the FISH device. J Invasive Cardiol. 2008;20(4):152–6.
Maxien D, Behrends B, Eberhardt KM, et al. Evaluation of the 6-F ExoSeal vascular closure device in antegrade femoral artery punctures. J Endovasc Ther. 2012;19(6):836–43. doi:10.1583/JEVT-12-3922R.1.
Conflict of interest
Dr. Rafiuddin Patel, Prof. Stefan Muller-Hulsbeck, Dr. Robert Morgan, and Dr. Raman Uberoi have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Patel, R., Muller-Hulsbeck, S., Morgan, R. et al. Vascular Closure Devices in Interventional Radiology Practice. Cardiovasc Intervent Radiol 38, 781–793 (2015). https://doi.org/10.1007/s00270-015-1116-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-015-1116-1