
Abstract
Introduction
Long-term results of uterine artery embolization (UAE) for adenomyosis are largely unknown. We assess long-term outcome of UAE in 40 women with adenomyosis.
Materials and methods
Between March 1999 and October 2006, 40 consecutive women with adenomyosis (22 in combination with fibroids) were treated with UAE. Changes in junction zone thickness were assessed with magnetic resonance imaging (MRI) at baseline and again at 3 months. After a mean clinical follow-up of 65 months (median 58 [range 38–129]), women filled out the uterine fibroid symptom and quality of life (UFS-QoL) questionnaire, which had additional questions on the long-term evolution of baseline symptoms and adverse events.
Results
During follow-up, 7 of 40 women (18%) underwent hysterectomy. Among these 7 women, the junction zones were significantly thicker, both at baseline (mean 23 vs. 16 mm, P = 0.028) and at 3-month follow-up (mean 15 vs. 9 mm, P = 0.034). Of 33 women with preserved uterus, 29 were asymptomatic. Four patients had symptom severity scores of 50 to 85 and overall QoL scores of 60 to 66, indicating substantial clinical symptoms. There was no relation between clinical outcome and the initial presence of fibroids in addition to adenomyosis.
Conclusion
In women with therapy-resistant adenomyosis, UAE resulted in long-term preservation of the uterus in the majority. Most patients with preserved uterus were asymptomatic. The only predictor for hysterectomy during follow-up was initial thickness of the junction zone. The presence or absence of fibroids in addition to adenomyosis had no relation with the need for hysterectomy or clinical outcome.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Adenomyosis is a benign uterine disease characterized by invasion of endometrium into the myometrium resulting in focal or diffuse enlargement of the uterus. Adenomyosis commonly affects premenopausal women with clinical symptoms similar to those of uterine fibroids, such as abnormal uterine bleeding and dysmenorrhea [1]. Treatment options consist of hormonal therapy and endometrial ablation [2]. However, these therapies often fail, and hysterectomy may then be offered as definitive treatment for the adenomyosis [2].
In recent years, uterine artery embolization (UAE) has emerged as an effective therapy in the treatment of uterine fibroids. However, UAE for adenomyosis is considered controversial by some investigators because recurrence of symptoms has been observed after a symptom-free period [3, 4]. In contrast there is increasing evidence that UAE might be effective in the treatment of adenomyosis [5, 6].
Short-term clinical results of UAE for symptomatic adenomyosis are promising in most observational studies, but long-term results are largely unknown [7–9]. In this study, we assess long-term clinical and imaging results in a cohort of 40 women with adenomyosis with or without associated fibroids.
Materials and Methods
Patients
The Institutional Review Board approved this retrospective study with a waiver for informed consent. From our database with prospectively collected data, we identified 40 consecutive women (mean age 43.7 years; median 45; range 31–51) with adenomyosis treated with UAE between March 1999 and October 2006. Of 40 women, 18 had pure adenomyosis, and 22 had adenomyosis in combination with fibroids. The diagnosis of adenomyosis was established by history, clinical examination and magnetic resonance imaging (MRI). Adenomyosis on MRI was defined as diffuse or focal thickness of the junction zone of >12 mm with low myometrial signal intensity on T2-weighted images. Presenting symptoms of the 40 women with adenomyosis were abnormal bleeding in 38 (95%), pain in 25 (63%), and pressure in 13 (33%). In all women, therapy with progestogens, hemostatic agents, or gonadotrophin-releasing hormone agonists had insufficient clinical response. Embolization was offered as treatment to women who sought to preserve the uterus.
MRI at Baseline and 3-Month Follow-Up
MRI consisted of T2- and T1-weighted contrast-enhanced images and was performed before embolization and again at 3-month follow-up. The following criteria were used for diagnosis of adenomyosis on the basis of sagittal T2-weighted images: low myometrial signal intensity, diffuse (>12 mm) or focal thickening of the junctional zone, high signal–intensity foci corresponding to myometrial cysts, poor definition of the endomyometrial junction, and poor definition of lesion borders.
UAE Procedure
UAE was performed after selective catheterization of both uterine arteries by way of a unilateral approach as described in earlier reports [6]. Embospheres of 500–700 and 700–900 μm (Biosphere Medical, Roissy, France) were used as embolic agent. Embospheres of 500–700 μm were preferably used in women with pure adenomyosis because the afferent arterioles in this condition are generally somewhat smaller than the vessels of the perifibroid plexus. The end point of embolization was complete stasis of contrast in the ascending segment of the uterine artery. Complications were recorded.
Clinical Follow-Up
Baseline clinical status was assessed using a standardized questionnaire inquiring about bleeding symptoms, pain, and pressure symptoms. In patients with hysterectomy during follow-up, timing was recorded. In January 2010, all 40 women agreed to participate in this long-term clinical follow-up study. Women with preserved uterus filled out the uterine fibroid symptom and quality of life (UFS-QoL) questionnaire, which had additional questions on long-term evolution of baseline symptoms and adverse events. Women with a symptom severity score <20 in combination with an overall health-related QoL score >80 were considered asymptomatic. In patients with hysterectomy during follow-up, the following clinical and imaging parameters were compared with those of patients with preserved uterus at follow-up: initial presence of fibroids, initial junction zone thickness, and decrease of junction zone thickness on 3-month follow-up MRI.
Statistical Analysis
Summary descriptive statistics were used for demographic parameters. Complications were expressed as a proportion with 95% confidence interval (CI). Timing of hysterectomy during follow-up was evaluated with Kaplan Mayer survival analysis. In women with preserved uterus, mean decrease in junction zone thickness was calculated as a proportion of initial value from baseline and 3-month follow-up MRI. Unpaired Student t test was used for comparison of means, and χ2 test was used for proportions; P < 0.05 was considered significant. Statistical analysis was performed with MedCalc statistical software (MedCalc, Mariakerke, Belgium).
Results
UAE
There were no procedural complications in 40 women (0%; 95% CI 0–10.4%). During follow-up, 2 women (age 40 and 44 years, respectively) developed permanent amenorrhea, and 1 woman (age 38 years) had transient amenorrhea. Three women reported transient increased vaginal discharge.
Additional Therapy
During a mean clinical follow-up of 65 months (median 58 [range 38–129]) in 8 of 40 women (20%), additional therapy was performed due to insufficient symptom relief. Seven women underwent hysterectomy (3 with pure adenomyosis and 4 with adenomyosis and fibroids), and 1 woman underwent embolization a second time. Timing of hysterectomy during follow-up in 7 patients is displayed in Fig. 1. Five of 7 hysterectomies occurred within 18 months after UAE, and 2 occurred after >5 years after UAE.

Timing of hysterectomy in 7 of 40 patients during long-term follow-up
Clinical Results
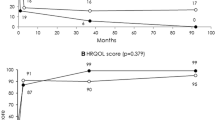
The results of the UFS-QoL questionnaires in 33 patients with preserved uterus during a mean follow-up of 65 months (median 58 [range 38–129]) are listed in Table 1. Of 33 women, 29 had symptom severity scores <20 in combination with overall health-related QoL scores >80, indicating they were asymptomatic. Four patients had symptom severity scores of 50–85 and overall QoL scores of 60–66, indicating substantial clinical symptoms despite embolization. There was no relation between clinical outcome and the initial presence of fibroids in addition to adenomyosis (Table 2). The long-term evolution of baseline symptoms is listed in Table 3.
MRI
All 40 patients underwent 3-month follow-up MRI; mean junction zone thickness for patients in relation to clinical outcome is listed in Table 4. The 7 women with hysterectomy during follow-up had significantly thicker junction zones compared with 29 patients having clinical improvement both at baseline (mean 23 vs. 16 mm, P = 0.028) and at 3-month follow-up (mean 15 vs. 9 mm, P = 0.034). There was no difference in mean junction zone thickness between 29 patients with clinical improvement and 4 patients with unchanged clinical status both at baseline and at 3 months follow-up.
Discussion
In this study, we found that in women with therapy-resistant adenomyosis, UAE results in long-term preservation of the uterus in the majority. Almost all patients with preserved uterus were asymptomatic with good health related QoL. The only predictor for hysterectomy during follow-up after UAE was the initial thickness of the junction zone: Patients with hysterectomy had substantial thicker junction zones on baseline MRI. The presence or absence of fibroids additional to the adenomyosis had no relation with clinical outcome. Most hysterectomies were performed within 18 months after UAE.
Our results are in concordance with those of Kim et al. [10], who conducted the only other long-term follow-up study of women with adenomyosis treated with UAE. In that study, long-term clinical success after >3.5 years was achieved in 50 of 54 women (93%), and 31 women (57%) were still asymptomatic. During the follow-up period, 5 women underwent hysterectomy for recurrence of symptoms. Other studies concerning the subject comprise mostly small case series with incomplete and variable follow-up. In a small case series of 18 patients by Pelage et al. [3], most patients had improvement or cure of symptoms, and 5 (28%) patients underwent hysterectomy at various time intervals during follow-up. In a series of 30 patients by Jha et al. [7], good outcome was reported in all patients after 1-year follow-up.
Recent studies [7, 8, 10, 11] tried to identify MRI predictors for good long-term clinical outcome of UAE in patients with symptomatic adenomyosis. Decrease of junction zone thickness, volume decrease of the uterus, and presence of areas of infarction after UAE were inconsistently observed in women both with and without improvement of symptoms. These observations indicate that follow-up MR imaging parameters have only limited value in prediction of good or bad clinical outcome. MRI may be of help in the diagnosis of adenomyosis and in assessment of concomitant fibroids. The MRI observation in our study, i.e., that a thick junction zone at baseline and at 3 months after UAE is related to hysterectomy during long-term follow-up, is important when counseling patients before UAE. Patients with a thick junction zone may be informed about the lower chance of clinical success.
Regarding follow-up after UAE for adenomyosis, evolution of symptoms is the most important parameter. In patients with improvement of symptoms and satisfaction with treatment, MRI follow-up may not be necessary as a routine procedure. However, in patients with insufficient clinical response after UAE, MRI can be helpful to compare thickness of the junction zone, uterine volume, and other parameters with baseline findings and thus MRI follow-up may guide clinical decision making.
In conclusion, our long-term follow-up study of 40 patients with adenomyosis treated with UAE confirmed the good clinical outcome of previous studies in these patients. We found no difference in clinical outcome between women treated with UAE for pure adenomyosis or in combination with fibroids. Almost all patients improve in the short term, and the majority are asymptomatic in the long term. Only a small proportion of patients will proceed to hysterectomy at various intervals after UAE due to treatment failure or recurrence of symptoms. MRI is helpful in the diagnosis of adenomyosis and the presence of concomitant fibroids. A thick junction zone at baseline is a predictor of insufficient clinical response. MRI has little value in clinical decision making at follow-up in patients with a favourable clinical response.
References
Azzir R (1989) Adenomyosis: current perspectives. Obstet Gynecol Clin N Am 16:221–235
Wood C (1988) Surgical and medical treatment of adenomyosis. Hum Reprod Update 4:323–336
Pelage JP, Jacob D, Fazel A et al (2005) Midterm results of uterine artery embolization for symptomatic adenomyosis: initial experience. Radiology 234:948–953
Bratby MJ, Walker WJ (2009) Uterine artery embolisation for symptomatic adenomyosis—mid-term results. Eur J Radiol 70:128–132
Levgur M (2007) Therapeutic options for adenomyosis: a review. Arch Gynecol Obstet 276:1–15
Rabinovici J, Stewart EA (2006) New interventional techniques for adenomyosis. Best Pract Res Clin Obstet Gynaecol 20:617–636
Jha RC, Takahama J, Imaoka I et al (2003) Adenomyosis: MRI of the uterus treated with uterine artery embolization. AJR Am J Roentgenol 181:851–856
Siskin GP, Tubulin ME, Stainken BF, Dowling K, Dolen EG (2001) Uterine artery embolization for the treatment of adenomyosis: clinical response and evaluation with MR imaging. AJR Am J Roentgenol 177:297–302
Lohle PN, De Vries J, Klazen CA, Boekkooi PF, Vervest HA, Smeets AJ et al (2007) Uterine artery embolization for symptomatic adenomyosis with or without uterine leiomyomas with the use of calibrated tris-acryl gelatin microspheres: midterm clinical and MR imaging follow-up. J Vasc Interv Radiol 18:835–841
Kim MD, Kim S, Kim NK et al (2006) Long-term results of uterine artery embolization for symptomatic adenomyosis. AJR Am J Roentgenol 186:855–864
Kitamura Y, Allison SJ, Jha RC et al (2006) MRI of adenomyosis: changes with uterine artery embolization. AJR Am J Roentgenol 186:855–864
Conflict of interest
The authors do not have any conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Smeets, A.J., Nijenhuis, R.J., Boekkooi, P.F. et al. Long-Term Follow-up of Uterine Artery Embolization for Symptomatic Adenomyosis. Cardiovasc Intervent Radiol 35, 815–819 (2012). https://doi.org/10.1007/s00270-011-0203-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-011-0203-1