
Abstract
Background and Purpose
It is known that interventional neuroradiology (IN) involves high radiation dose to both patients and staff even if performed by trained operators using modern fluoroscopic X-ray equipment and dose-reducing technology. Therefore, every new technology or imaging tool introduced, such as three-dimensional rotational angiography (3D RA), should be evaluated in terms of radiation dose. 3D RA requires a series with a large number of images in comparison with 2D angiography and it is sometimes considered a high-dose IN procedure. The literature is scarce on the 3D RA radiation dose and in particular there are no data on carotid arteriography (CA). The aim of this study was to investigate patient dose differences between 2D and 3D CA.
Methods
The study included 35 patients undergoing 2D CA in hospital 1 and 25 patients undergoing 3D CA in hospital 2. Patient technical data collection included information on the kerma area product (KAP), fluoroscopy time (T), total number of series (S), and total number of acquired images (F).
Results
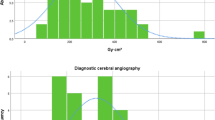
Median KAP was 112 Gy cm2 and 41 Gy cm2 for hospitals 1 and 2, respectively, median T was 8.2 min and 5.1 min, median S was 13 and 4, and median F was 247 and 242. Entrance surface air-kerma rate, as measured in “medium” fluoroscopy mode measured in 2D acquisition using a 20 cm phantom of polymethylmethacrylate, was 17.3 mGy/min for hospital 1 and 9.2 mGy/min for hospital 2.
Conclusion
3D CA allows a substantial reduction in patient radiation dose compared with 2D CA, while providing the necessary diagnostic information.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
It is widely known that interventional neuroradiology (IN) involves a high radiation dose to both patients [1–6] and staff [7–10] even if it is performed by trained operators with modern fluoroscopic X-ray equipment and dose-reducing technology [4]. As the application of IN procedures expands, a number of radiation injuries have been reported [11, 12] and the need to measure radiation dose has become evident. A number of studies in the recent literature either evaluate the radiation risk during such procedures [13], or propose methods to determine entrance skin dose to the patient [14–16]. The results of the American Society of Cardiovascular and Interventional Radiology task force study revealed that some interventional radiology procedures may produce a maximum skin dose sufficient to cause deterministic effects to the skin [17].
It is evident that every new technology or imaging tool that is introduced in IN should be evaluated in terms of clinical benefit and radiation dose. One of these is three-dimensional rotational angiography (3D RA), which provides additional useful information to two-dimensional digital subtraction angiography (2D DSA). In this technique, 2D angiographic projections are acquired in a 180° arc. These projections are then used to reconstruct a 3D volumetric image which can be viewed at any angle for optimal delineation of the existing anatomy [6]. Due to the fact that 3D RA requires series with a large number of images (100–300 images in every series) in comparison with those of 2D conventional angiography (10–40 images per series), it is considered by some authors as a relatively high-dose IN procedure producing an additional dose to the patient [18]. On the other hand, the literature data regarding the radiation dose in 3D RA are limited and based on theoretical calculations of radiation dose [6, 19], while there are practically no data on carotid arteriography (CA). Recognizing the need for measuring the radiation dose in IN procedures, the European Concerted Action SENTINEL (Safety and Efficacy for New Techniques and Imaging using New Equipment to Support European Legislation) [20] has included radiation dose measurements in one of its work packages. Within this context, and appreciating the absence of patient radiation data on 3D versus 2D CA, the authors of the current study investigated the differences in patient dose between two centers using these two techniques.
Materials and Methods
Participating Hospitals
The study included measurements performed in two major hospitals in Greece and Spain. The first hospital (henceforth referred to as hospital 1) is situated in Athens and is the second largest hospital in Greece. It is a tertiary hospital of 700 beds and has a mean number of 40,000 inpatients every year. The second hospital is situated in Madrid (henceforth referred to as hospital 2) and is a University Hospital. It is also a tertiary hospital of around 950 beds, had 36,000 inpatients during 2005, and serves a fixed population of about 550,000 people in Madrid. About 3,000 interventional procedures are performed every year in hospitals 1 and 2 respectively.
X-ray Equipment
CA procedures in hospital 1 were performed with a digital angiography system (Philips Integris V3000; Philips Medical Systems, Best, The Netherlands) installed in 1995. The system was equipped with an undercouch tube/overcouch image intensifier with a full field of view (FOV) of 40 cm diameter and three magnification modes of 28 cm, 20 cm, and 14 cm diameter, respectively. Patient data in hospital 2 were collected in a Philips Integris Allura (Philips Medical Systems, Best, The Netherlands) monoplanar machine installed in 2005. The X-ray equipment was equipped with an undercouch tube/overcouch flat detector with a full FOV of 48.4 cm diagonal square and three magnification modes of 42.0 cm, 31.1 cm, and 22.6 cm diagonal square, respectively. The basic technical characteristics of the systems are given in Table 1. The entrance surface air-kerma rate (ESAKR) in fluoroscopy mode and the entrance surface air-kerma (ESAK) per image were the dosimetric quantities used to describe each machine. These dosimetric quantities (with backscatter included) are measured at the central beam axis of a phantom, the center of which is positioned at the isocenter of the X-ray system, as defined in the most recent document of the International Electrotechnical Commission [21]. In the current study, ESAKR and ESAK were measured with a calibrated dosimeter at the entrance to a 20 cm thick polymethylmethacrylate (PMMA) phantom that simulated a normal-sized patient (70 kg) and was placed on the patient table. The bottom of the phantom was placed at the interventional reference point (IRP) of the system (this being the point that represents the position of the patient skin’s at the entry site of the X-ray beam during interventional procedures [17]) with the antiscatter grid in position. Routine quality control tests were performed during the period of the study to confirm that the performance of the X-ray systems was in accordance with the manufacturer’s specifications and conformed to national standards.
Both X-ray systems had a kerma-area product (KAP) meter installed in the head of each unit so as to measure the patient radiation dose. The KAP meters were calibrated according to standard procedures [22]. The uncertainty in the reading of both instruments, as quoted by the manufacturer, was 4% for tube potentials ranging from 50 kVp to 110 kVp.
Patient Data
The study included 35 patients undergoing 2D CA in hospital 1 and 25 patients undergoing 3D CA in hospital 2. Board-certified senior interventional radiologists with sufficient knowledge of radiation protection measures, obtained in various radiation protection workshops, performed the above procedures. Patient informed consent was waived (by agreement with the ethics committee of the hospitals) since no personal data on the patients were used and dosimetric measurements are standard practice for these procedures. Patient technical data collection was based on a protocol developed during the SENTINEL project [20] that included information on KAP, fluoroscopy time in minutes (T), the total number of series (S), and the total number of images (F). The total number of images presented for hospital 2 are the sum of 2D images and 3D images (with a much lower dose per image: typically 0.1 mGy/image for a rotational image and 1.0–8.0 mGy/ image for a DSA image, depending on the body region being examined and the acquisition protocol). The patient sample was taken at random, including patients of various weights and sizes, since the KAP variation due to complexity of nominally identical IR techniques dominates the variation due to patient size [23].
Results
Table 2 presents a typical 3D CA procedure in which the details of the technique are shown. The 3D procedure includes one or two rotational acquisitions with 121 frames in each rotational series. As seen in Table 2, the second and the fifth series are rotational acquisitions that are taken applying approximately 1 mAs per image, in contrast to other 2D series with 9–84 mAs per image.
Table 3 shows the main technical parameters for 2D CA (hospital 1) and 3D CA (hospital 2). Due to the fact that the distributions of KAP and other technical parameters such as T, S, and F did not exhibit a normal distribution, instead of mean values, the median and range were calculated. As shown in the table, F is similar in hospitals 1 and 2 (approximately 245 images in total) but taken in a different way. Hospital 1, which does not apply RA, takes 247 2D images in 14 series resulting in about 18 images per series, whereas hospital 2 uses the rotational acquisition technique (121 images of low dose), avoiding some of the 2D series requiring more dose per acquired image (typically a factor of 10–80 in comparison with 3D images).
Discussion
As the results of the study show, the median patient radiation dose in 3D CA (41 Gy cm2) is almost 3 times lower than the value in 2D CA (112 Gy cm2). The dose differences are in part attributed to the different dose settings of the X-ray systems (Table 1). It must be noted though, that hospital 2 presented a much higher ESAK than hospital 1 and should normally have higher patient KAP values, since it is proven that up to 96% of the total dose to the patient in CA is due to image acquisition [15, 18, 24]; similar findings have also been reported for other interventional procedures [25–27]. The opposite, however, is shown in Table 3. This could be partially attributed to the use of RA, although the clinical protocol, the X-ray equipment, and the skill of the radiologist in each hospital also play an important role. In order to investigate whether the use of RA actually lowers the dose to the patient, a small sample of 2D and 3D CA procedures was collected and analyzed exclusively at hospital 2: The technical data of 17 3D and 28 2D CA procedures were collected, again using the SENTINEL protocol (Table 4). The results show a 27% reduction in KAP, 23% reduction in the number of images, and 23% reduction in the number of series. Thus, it seems that rotational acquisitions in carotid procedures allow a clear reduction in patient doses. Image quality in RA runs is, of course, not as good as in DSA series. However, after numerical reconstruction, 3D images allow selection of the appropriate C-arm angulations and avoid some of the DSA series typically acquired when the 3D option is not used. Unfortunately, there are no data in the literature regarding the radiation dose differences between 3D and 2D CA, for comparison purposes. Schueler et al. [19] reported radiation dose results for this imaging tool in CA, concluding that the 3D RA patient radiation dose is significantly lower than that for biplanar DSA. Their findings were based on an anthropomorphic skull phantom and biplanar DSA, the exposure parameters of which were determined by reviewing 40 patient DSA series. Bridcut et al. [6] calculated the patient dose during assessment of aneurysms. Their study was limited to the aneurysm assessment phase, which forms only part of the IN technique. They estimated mean total dose and claimed an overall reduction of patient dose by approximately 25%.
Limitations of our study include differences in operator skill, complexity of cases, imaging protocol, and X-ray equipment, which prevented detailed comparison of the two methods. However, the objective of our study was to investigate how radiologists are performing CA in two similar hospitals with and without RA so as to compare radiation doses to the patients. Clinical outcome was considered appropriate at all times since, otherwise, radiologists would never follow the particular practice. Initial findings seemed to favor the use of 3D RA in comparison with 2D in CA. The use of 3D avoids several 2D series, allowing the selection of the most useful projections [6]. This is very important for patient care and outcome, since 3D eliminates the misregistration artifacts that are associated with 2D and reduces the chance of motion artifacts by single acquisition [26].
The results of the study were compared with other data in the literature (Table 5). The large range in the results demonstrates the need to closely monitor radiation doses in CA and to find dose optimization techniques. It is also seen that older studies reported lower dose values in 2D CA while more recent studies, such as that of Bor et al. in 2006 [18] (131.8 Gy cm2) as well as the current study (112 Gy cm2), reported higher values due probably to more extended imaging protocols (larger number of series and images per series). A higher complexity of procedures could also be the reason for the differences in dose values since in the present study patient samples were taken at random. According to the clinical findings of the current study, 3D CA can result in large reduction of the radiation dose to patients and can be an important dose-reduction technique.
CA, a diagnostic IN procedure, requires quite long fluoroscopy times and a large number of images to adequately study the vasculature of the brain and to effectively and accurately investigate possible pathology. Therefore, it is associated with potentially high doses to the patient’s head and needs close monitoring, especially every time a new technique or imaging tool is introduced. Furthermore, constant dose optimization is essential so as to avoid the possibility of radiation injuries such as erythema or epilation [11, 12, 28–30]. As far as alternative methods are concerned, computed tomography angiography (CTA) can also be used for diagnosis and all necessary measurements for the evaluation of lesions as well as estimation of balloon or stent dimensions, with high sensitivity and specificity for the detection of intracranial aneurysms [31]. It should be noted also that some authors suggest the CTA radiation dose is lower than that of conventional angiography [32–34]. As quoted by Kuiper et al. [33], the average effective dose for CTA of the pulmonary arteries is 4.2 mSv (range 2.2–6.0 mSv), whereas pulmonary DSA has an average effective dose of 7.1 mSv (range 3.3–17.3 mSv). The aim of the current study, however, was simply to provide interventionalists with the radiation dose data for DSA with and without RA, to enable them to decide whether to use this option or upgrade existing systems. The results of the current study show that RA can substantially lower the radiation dose to the patient. Therefore RA could become a very important imaging tool allowing interventionalists to discover the projections that provide maximum information for diagnosis while simultaneously reducing the number of 2D series, which are those that contribute most of the dose to the patient.
References
Mini RL, Schmid B, Schneeberger P, et al. (1998) Dose-area product measurements during angiographic X-ray procedures. Radiat Prot Dosim 80:145–148
Steele HR, Temperton DH (1993) Technical note: Patient doses received during digital subtraction angiography. Br J Radiol 66:452–456
Fletcher DW, Miller DL, Balter S, et al. (2002) Comparison of dour techniques to estimate radiation dose to skin during angiographic and interventional radiology procedures. J Vasc Interv Radiol 13:391–397
Miller DL, Balter S, Cole P, et al. (2003) Radiation doses in interventional radiology procedures: The RAD-IR study. I. Overall measures of dose. J Vasc Interv Radiol 14:711–727
Hatakeyama Y, Kakeda S, Korogi Y, et al. (2006) Intracranial 2D and 3D DSA with flat panel detector of the direct conversion type: Initial experience. Eur Radiol 16:2594–2602
Bridcut, R, Murphy E, Workman A, et al. (2007) Patient dose from 3D rotational neurovascular studies. Br J Radiol [DOI: 10.1259/bjr/95349672]
Williams JR (1997) The interdependence of staff and patient doses in interventional radiology. Br J Radiol 70:498–503
Marx MV (2003) The radiation dose in interventional radiology study: Knowledge brings responsibility. J Vasc Interv Radiol 14:947–951
Behrman RB, Hijadi ZM (1999) Radiation risks to the patients and interventionalists: Risk reduction. Cathet Cardiovasc Intervent 45:455–456
Wenzl T, McDonald JC (2002) Is there and elevated risk of brain cancer among physicians performing interventional radiology procedures? Radiat Prot Dosim 102:99–100
Wagner L, McNeese MD, Marx V, et al. (1999) Severe skin reactions from Interventional fluoroscopy: Case report and review of the literature. Radiology 213:773–776
Mooney RB, McKinstry CS, Kamel HA (2000) Absorbed dose and deterministic effects to patients in interventional neuroradiology. Br J Radiol 73:745–751
Livingstone RS, Raghuram L, Korah IP, et al. (2003) Evaluation of radiation risk and work practices during cerebral interventions. J Radiol Prot 23:327–336
Rampado O, Ropolo R (2005) Entrance skin dose distribution maps for interventional neuroradiological procedures: A preliminary study. Radiat Prot Dosim 117:256–259
Gkanatsios NA, Huda W, Peters KR (2002) Adult patient doses in interventional neuroradiology. Med Phys 29:717–723
Rampado O, Ropolo R (2004) A method for a real time estimation of entrance skin dose distribution in interventional neuroradiology. Med Phys 31:2356–2361
Miller DL, Balter S, Cole P, et al. (2003) Radiation doses in interventional radiology procedures: The RAD-IR study. II. Skin Dose. J Vasc Interv Radiol 14:977–990
Bor D, Cekirge S, Türkay T, et al. (2005) Patient and staff doses in interventional neuroradiology. Radiat Prot Dosim 117:62–68
Schueler B, Kallmes D, Cloft H (2005) 3D cerebral angiography: Radiation dose comparison with digital subtraction angiography. AJNR Am J Neuroradiol 26:1898–1901
SENTINEL. Safety and efficacy for new techniques and imaging using new equipment to support European legislation. European Coordination Action (2005–2007). http://www.sentinel.eu.com/Documents/Project+Presentation.pdf. Accessed April 7, 2007
International Electrotechnical Commission IEC report 60601 (2000) Medical electrical equipment part 2–43: Particular requirements for the safety of X-ray equipment for interventional procedures. International Electrotechnical Commission, Geneva
Dosimetry Working Party of the Institute of Physical Sciences (1992) National protocol for patient dose measurements in diagnostic radiology. NRPB and College of Radiographers
Reay J, Chapple CL, Kotre CJ (2003) Is patient size important in dose determination and optimization in cardiology? Phys Med Biol 48:3843–3850
Struelens L, Vanhavere F, Bosmans, et al. (2005) Skin dose measurements on patients for diagnostic and interventional neuroradiology: A multicentre study. Radiat Prot Dosim 114:143–146
Bashore TM, Durcham NC (2004) Radiation safety in the cardiac catheterization laboratory. Am Heart J 147:375–378
Kuon E, Glaser C, Dahm JB (2003) Effective techniques for reduction of radiation dosage to patients undergoing invasive cardiac procedures. Br J Radiol 76:406–413
Hirai T, Korogi Y, Suginohara K, et al. (2003) Clinical usefulness of unsubtracted 3D digital angiography compared with rotational digital angiography in the pretreatment evaluation of intracranial aneurysms. AJNR Am J Neuroradiol 24:1067–1074
Norbash AM, Busick D, Marks MP (1996) Techniques for reducing interventional neuroradiologic skin dose: Tube position rotation and supplemental beam filtration. AJNR Am J Neuroradiol 17:41–49
Huda W, Peters KR (1994) Radiation induced temporary epilation after neuroradiologically guided embolization procedure. Radiology 193:642–644
Shortt CP, Fanning NF, Malone L, et al. (2007) Thyroid dose during neurointerventional procedures: Does lead shielding reduce the dose? Cardiovasc Intervent Radiol [Epub ahead of print, May 29]
Jayaraman MV, Mayo-Smith WW, Tung GA (2004) Detection of intracranialaneurysms: Multi-detector row CT angiography compared with DSA. Radiology 230:510–518
Coche E, Vynckier S, Octave-Prignot M (2006) Pulmonary embolism: Radiation dose with multi-detector row CT and digital angiography for diagnosis. Radiology 240:690–697
Kuiper JW, Geleijns J, Matheijssen NA (2003) Radiation exposure of multi-row detector spiral computed tomography of the pulmonary arteries: Comparison with digital subtraction pulmonary angiography. Eur Radiol 13:1496–500 [Epub Nov 13, 2002]
Willmann JK, Baumert B, Schertler T (2005) Aortoiliac and lower extremity arteries assessed with 16-detector row CT angiography: Prospective comparison with digital subtraction angiography. Radiology 236:1083–1093 [Epub July 29, 2005]
Acknowledgments
This study was partially funded by the European Commission Coordination Action SENTINEL (FP6-012909) and the Spanish grant FIS2006-08186 (Ministry of Education and Science).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tsapaki, V., Vano, E., Μavrikou, I. et al. Comparison of Patient Dose in Two-Dimensional Carotid Arteriography and Three-Dimensional Rotational Angiography. Cardiovasc Intervent Radiol 31, 477–482 (2008). https://doi.org/10.1007/s00270-007-9190-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-007-9190-7