
Abstract
Bronchogenic cyst is a rare developmental lesion. It is usually asymptomatic and most frequently located in the middle mediastinum and lung parenchyma. It can cause symptoms only when infected or pressing on neighboring structures. The MRI findings in a 34-year-old woman with an 8 months history of back pain were evaluated and revealed a cystic lesion in the left paravertebral area. The histopathologic evaluation of the material aspirated with CT guidance was reported to be bronchogenic cyst. A simultaneous alcohol ablation was accomplished. After the procedure the patient’s pain disappeared and the follow-up MRI scan 1 year later revealed no relapse. Paravertebrally located bronchogenic cysts are very rare and only 3 cases were found to be reported in the medical literature prior to this one. While aspiration alone is sufficient for diagnosis, it is insufficient to treat the lesion and prevent the recurrences. This paper reports a paravertebral bronchogenic cyst which was symptomatic despite of its small size. CT-guided aspiration was accomplished and simultaneous alcohol ablation was carried out to prevent recurrences.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
A bronchogenic cyst is a rare congenital lesion formed by abnormal branching of the ventral foregut during the embryologic development of the lungs. Bronchogenic cysts are usually located in the middle mediastinum next to the carina, although such cysts have developed at sites other than the mediastinum [1]. Symptoms caused by bronchogenic cysts, while rare, usually result from the compression of adjacent structures (which can cause stridor, cough, dyspnea, cyanosis, syncope, superior vena cava syndrome, or pain) or from infected cysts [1].
We present the case of a woman with a paravertebral bronchogenic cyst that caused back pain. Despite its very small size, we aspirated the cyst under computed tomographic (CT) guidance and simultaneously performed alcohol ablation to prevent recurrence of the lesion. The atypical location of this small cyst that caused symptoms, our use of percutaneous alcohol ablation despite the small size of the lesion, and the patient’s prompt response to treatment render this report noteworthy.
Case Report
A 34-year-old woman with back pain of 8 months’ duration was admitted to our institution. The site of the pain was not restricted to a specific dermatome. The pain was relieved to some extent by treatment with nonsteroidal anti-inflammatory agents, increased with physical activity, and sometimes woke the patient from sleep. The results of physical examination and laboratory tests were unremarkable. Magnetic resonance imaging (MRI) of the thorax, which was performed to rule out pathologic conditions of the thoracic disk, revealed a cystic lesion (10 mm × 10 mm × 6 mm) that was hypointense on T1-weighted images and hyperintense on T2-weighted images (Fig. 1) in the left paravertebral region of the fourth thoracic vertebra. The lesion was not enhanced by the intravenous injection of contrast medium.

T4 vertebral level axial plane MR image. A T2-weighted spin echo sequence shows a left paravertebral cystic lesion with high signal intensity
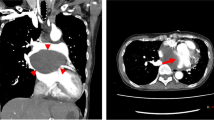
Percutaneous aspiration of the cyst to enable diagnosis and treatment was considered a minimally invasive intervention. Because the simple aspiration of cysts is known to result in high recurrence rates, we planned to instill alcohol into the cyst during aspiration. The procedure was explained to the patient, who provided written consent. Under CT guidance, a 22G Chiba needle was inserted into the cyst and 1 ml of clear mucoid fluid was aspirated. Then 0.3 ml of 96% alcohol was injected into the cyst (Fig. 2). Histopathologic analysis of the aspirated material confirmed the diagnosis of a bronchogenic cyst. The visual pain score of the patient, which had been 6 before the procedure, decreased to 0 after the procedure. The cyst-related pain was relieved completely, and at the 1 year follow-up evaluation, MRI studies showed no residual or recurrent lesion.

A, B CT images at the same T4 axial level before and during the procedure
Discussion
A bronchogenic cyst is a rare benign congenital cystic lesion that forms during the embryologic development of the tracheobronchial system. These cysts usually develop in the mediastinum and the pulmonary parenchyma [2]. In rare cases, cutaneous, retroperitoneal, cervical, infradiaphragmatic, intrapericardial, intraspinal, intracardiac, or intrapleural bronchogenic cysts have been identified [3], although such cysts rarely occur at paravertebral sites. A review of the medical literature revealed only 3 patients with a paravertebral bronchogenic cyst [4–6].
Bronchogenic cysts of the paravertebral region usually cause no symptoms. In rare instances, however, patients become symptomatic, as did the woman described in this report. The back pain that she experienced was probably caused by compression of the parietal pleural nerves by the cystic lesion. The resolution of pain after the aspiration and alcohol ablation of the cyst confirmed the lesion as the source of the patient’s discomfort. We were initially hesitant to treat such a small lesion with alcohol ablation, but no other source for the patient’s pain could be identified and we wanted to prevent recurrence of the cyst. Had the cyst recurred, its small size would have rendered repeat intervention more difficult. We therefore injected alcohol into the cyst to ensure its complete and permanent resolution.
CT imaging of a bronchogenic cyst usually reveals a homogeneous soft tissue or fluid density that is not enhanced by the intravenous injection of contrast medium [1]. On CT imaging the density of cysts containing calcium, anthracotic pigments, blood, or proteins increases [7]. Depending on the cyst content, T2-weighted MRI images have high-intensity signals and the signals of the T1-weighted sequences can be of either low or high intensity.
The definitive diagnosis of a bronchogenic cyst is based on histopathologic analysis: The cyst wall contains chondral elements, mucous glands, smooth muscle tissue, and fibrous tissue. An internal wall covering of ciliated respiratory epithelial cells is pathognomonic for a bronchogenic cyst [7]. In our patient, pathologic analysis of the cyst fluid revealed such cells.
To date, there is no standardized regimen for the treatment of bronchogenic cysts. Some authors recommend follow-up for asymptomatic patients [8], and others suggest surgical resection because of the risk of infection and the minimal risk of eventual malignant transformation [1]. Although aspiration alone can provide enough information for the diagnosis of a bronchogenic cyst, it is not enough to guide therapy because of the likelihood of recurrence of the lesion [9]. Aspiration and simultaneous alcohol ablation for the treatment of simple cysts that develop in various organs is a more effective therapy [10].
To the best of our knowledge, there is no prior report of the percutaneous alcohol ablation of a bronchogenic cyst. We injected the cyst with alcohol to prevent its recurrence because, given its small size, repeat intervention would have been more difficult or impossible [11]. We suggest that the use of alcohol ablation in addition to simple aspiration played a role in the complete resolution of our patient’s cyst.
Bronchogenic cysts can develop in atypical locations and can cause symptoms regardless of their size. Percutaneous aspiration and the simultaneous injection of alcohol combine diagnosis with treatment and are safe for the patient. This combined method can be applied to even very small cysts if the patient is symptomatic and no other source of the symptoms can be identified.
References
McAdams HP, Kirejczyk WM, Rosado-de-Christenson ML, Matsumoto S (2000) Bronchogenic cyst: Imaging features with clinical and histopathologic correlation. Radiology 217:441–446
Mehta RP, Faquin WC, Cunningham MJ (2004) Cervical bronchogenic cysts: A consideration in the differential diagnosis of pediatric cervical cystic masses. Int J Pediatr Otorhinolaryngol 68:563–568
Lee T, Tsai IC, Tsai WL, Jan YJ, Lee CH (2005) Bronchogenic cyst in the left atrium combined with persistent left superior vena cava: The first case in the literature. AJR Am J Roentgenol 185:116–119
Desrumaux I, De Wever W, Verschakelen J (2001) Paravertebral and diaphragmatic mass: An ectopic location of bronchogenic cyst. JBR-BTR 84:8–9
Beall DP, Daley ND, Liu CZ, Fish JR (2005) Paravertebral bronchogenic cyst diagnosed by computed tomography-guided biopsy. Curr Probl Diagn Radiol 34:163–166
Brunelli A, Al Refai M, Fianchini A (1998) Isolated bronchogenic cyst of the lower mediastinum. J Thorac Cardiovasc Surg 116:372–373
Duranceau ACH, Deslauriers J (2000) Foregut cysts the mediastinum. In: Shields TW, LoCicero J III, Ponn RB (eds) General thoracic surgery. Lippincott Williams & Wilkins, Philadelphia, pp 2401–2413
Zylak CJ, Eyler WR, Spizarny DL, Stone CH (2002) Developmental lung anomalies in the adult: Radiologic-pathologic correlation. Radiographics 22:25–43
Read CA, Moront M, Carangelo R, Holt RW, Richardson M (1991) Recurrent bronchogenic cyst. An argument for complete surgical excision. Arch Surg 126:1306–1308
Anon R, Guijarro J, Amoros C, et al (2006) Congenital splenic cyst treated with percutaneous sclerosis using alcohol. Cardiovasc Intervent Radiol 29:691–693
Roos-Hesselink JW, Verhoeven GT, Stoker J (1996) Bronchogenic cyst mimicking an intracardiac mass: Diagnosis by magnetic resonance imaging and treatment by needle aspiration. Heart 75:639
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lakadamyali, H., Ergun, T., Lakadamyali, H. et al. Alcohol Ablation Therapy of an Atypically Located Symptomatic Bronchogenic Cyst: A Case Report. Cardiovasc Intervent Radiol 30, 1274–1276 (2007). https://doi.org/10.1007/s00270-007-9082-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-007-9082-x