
Abstract
The percutaneous approach for RF ablation of liver lesions high up in the dome is always difficult. The authors describe a transpulmonary approach that may be simpler and safer to use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
CT-guided radiofrequency ablation of liver tumors is a well-established technique, and may be curative for small (<3 cm) tumors [1, 2]. Tumors close to the dome of the liver are traditionally difficult to approach, even for biopsy, with CT or ultrasound guidance, and various techniques such as “gantry tilt” and MRI guidance have been used to circumvent the inherent difficulties [3, 4]. Transpulmonary biopsy of otherwise difficult to reach liver dome tumors has been described previously [5]. We describe a transpulmonary approach for radiofrequency ablation of tumors located in the dome of the liver. To our knowledge, this approach has not been described previously for radiofrequency ablation of liver tumors.
Case Report
A 56-year old woman with colon cancer underwent sigmoid resection along with intraoperative radiofrequency ablation of seven liver metastases ranging in size from 0.5 to 2 cm. The radiofrequency ablation (RITA, “Starburst” 7 cm probe, Mountain View, CA, USA) was performed during her primary surgery (open laparotomy) using palpation and intraoperative ultrasound for guidance. Her recovery was uneventful, and she underwent postoperative chemotherapy for 6 months with a combination of 5-fluorouracil and irinotecan. Approximately 9 months after her surgery, a new 2.5 cm tumor was discovered in her liver, segment VII, and was confirmed with a positive positron emission tomography scan that correlated with the CT findings. The patient was referred to the interventional radiology service for CT-guided percutaneous radiofrequency ablation of this tumor after the surgeon who had performed the first surgery declined to operate again.
The radiofrequency ablation procedure, performed under conscious sedation, was technically challenging, due to the long probe tract, in addition to being poorly tolerated by the patient who had difficulty with breath-holds. We used a 15° gantry tilt with an anterior subcostal approach, and after initial biopsy with a 15 cm 22G Chiba needle, we used a tandem approach to introduce a 14G coaxial LeVeen needle probe (Boston Scientific, Burlington, MA, USA) into the tumor. The tract was ablated after completion of the radiofrequency ablation. A resulting complication was a 5 cm × 4 cm hematoma anterior to the left lobe of the liver, underlying the probe insertion site. However, the patient recovered well, and there were no major complications.
Two months following the procedure, follow-up scans demonstrated a second tumor in segment VIII of the liver measuring 2 cm, located posteriorly along the diaphragmatic surface, and the patient was referred again for CT-guided percutaneous radiofrequency ablation. The lesion (nor the previously ablated lesion) was not seen on ultrasound, thus precluding ultrasound as a guidance modality. Upon discussion with the patient and the referring physician, and keeping in mind the technical difficulties of the previous procedure, general anesthesia was offered as an option for the second procedure.
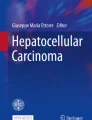
The patient was intubated, placed supine on the scanner table, and preliminary scans obtained, both without (Fig. 1A) and with a 10° gantry tilt (Fig. 1B). Since the shortest distance to the tumor that could reasonably be accessed via an anterior approach was 16–20 cm, we sought alternative routes.

A–C. A 56 year old woman with metastatic colon cancer referred for percutaneous radiofrequency ablation. A Initial planning non-contrast CT scan without gantry tilt demonstrates a distance of at least 20 cm to the tumor using a subcostal approach. B CT scan with 10° gantry tilt demonstrates a 16.3 cm distance to the tumor using the shortest route. The real distance would likely be longer because the needle insertion point would have to be lower to avoid traversing the pleura. C CT scan in the prone position and a transpulmonary approach plan demonstrate the virtual needle distance to the tumor to be 7 cm.
In consultation with the anesthesiologist, we decided to use a prone, transpulmonary approach. Accordingly, the patient was placed prone, and the shortest distance was measured at 7 cm (Fig. 1C). A transpulmonary intercostal (trans-eighth intercostal space) path was chosen. A 22G 10 cm Chiba needle was advanced into the tumor in one attempt after documenting an accurate path with an initial partial (extrapleural) insertion. This was followed by insertion of the trocar and cannula assembly of the 15 cm radiofrequency probe coaxial system (Boston Scientific, Burlington, MA, USA), using the tandem approach (Fig. 2A). Accurate positioning was achieved in two passes. After confirming accurate positioning of the trocar–cannula assembly in the tumor, the trocar was removed, and a 15 cm, 3.0 cm diameter, array-type probe (Boston Scientific, Natick, MA, USA) was inserted into the tumor and the tines deployed (Fig. 2B). The needle was removed and radiofrequency application commenced. The algorithm used was: initial starting power 50 W, followed by a 10 W increase every 1 min until “roll-off” was achieved (Radiotherapeutics RF2000 generator, Boston Scientific, Natick, MA, USA). “Roll-off” was achieved in 11 min, at 170 W, and this was followed by slight repositioning of the probe and restarting of the generator at 70% of the previous “roll-off” power; the second radiofrequency application took only 3 min. The entire procedure was monitored using intermittent CT scans (GE Lightspeed Ultra, General Electric, Milwaukee, WI, USA). No pneumothorax was noted either before or during the radiofrequency ablation procedure.

A–C. A 56 year old woman with metastatic colon cancer undergoing CT-guided radiofrequency ablation using the transpulmonary approach. A Tandem insertion of 22G needle and radiofrequency probe into the tumor using a posterior transpulmonary approach. B Deployment of the tines of the radiofrequency probe with complete coverage of the tumor area. C Contrast-enhanced CT scan following removal of probe at the end of the procedure demonstrates a small pneumothorax around the dome of the diaphragm. The patient did not suffer any clinical consequences, and recovered uneventfully.
At the end of the procedure, the probe was removed and an immediate postprocedural scan obtained after injection of 100 cm3 of intravenous nonionic contrast. The entire ablated area, including the tumor, was nonenhancing. At this point, a small pneumothorax was noted predominantly layering around the diaphragm (Fig. 2C). A postprocedural chest radiograph demonstrated a mildly raised right hemidiaphragm, minimal basal atelectasis, and a thin crescent of right apical pneumothorax.
Intraprocedural monitoring throughout the procedure showed that the patient’s oxygen saturation varied between 95% and 100%. Even after the small pneumothorax was discovered there was no decrease in the oxygen saturation, nor was there any increased resistance to ventilation. The patient was extubated without incident, and recovered well. Postprocedural chest radiographs obtained 2, 8, and 24 hr after the procedure showed a small sliver of right pneumothorax that resolved. The patient did not complain of any respiratory difficulty, and she was discharged home after overnight observation. When asked about the relative discomfort from the two percutaneous radiofrequency ablations, the patient stated that the second procedure was far more comfortable.
Discussion
Transpulmonary biopsy of liver tumors, particularly for tumors that are located high up and difficult to reach by other techniques, have been described previously, and based on one small series the innovation has been found to be effective and safe, even in the presence of underlying pulmonary disease [5]. We describe what is essentially an extension of the percutaneous transpulmonary liver biopsy technique, but applied to percutaneous radiofrequency ablation of otherwise difficult to reach liver tumors located high up in the dome of the liver.
The advantages include the ability to utilize a shorter path, fewer punctures through the liver, and the ability to place the radiofrequency probe more accurately rather than accepting a suboptimal placement after numerous attempts.
Potential complications would be related to the liver tumor treatment itself, and to puncture of the pleura, lung or diaphragm. Pneumothorax can be effectively treated intraprocedurally without interruption of the radiofrequency ablation as has been described for percutaneous ablation of lung tumors [6]. The treatment involves placement of a small-bore catheter or needle and manual aspiration of the pneumothorax if it interferes with the patient’s respiration or the ability to accurately localize the tumor to be ablated. Indeed, pneumothorax as a complication of percutaneous radiofrequency ablation of liver tumors using the non-transpulmonary route has been reported to have a pneumothorax rate of 0.2% [7].
Another complication that has been described from transpulmonary liver tumor biopsy is hemorrhage from the phrenic artery [8]. While this is certainly a potential problem, well worth being aware of, we believe that the coagulative action of the thermal ablation itself would prevent bleeding, particularly because the vessels involved are usually smaller than 2–3 mm in diameter. Also, in our case, the site of diaphragmatic entry was posterolateral, parallel to the expected course of the vessel, thereby decreasing the chances of injury [9, 10]. Diaphragmatic injury is possible but can be avoided, particularly if the ablation is centered away from the hepatic capsule, such that the expected maximal margin of the ablation volume is at least 1 cm away from the diaphragm. Also, it may be possible to more completely treat tumors close to the diaphragm if the area of contact is small, particularly when considering that most diaphragmatic injuries are not clinically significant [7].
Complications from the radiofrequency ablation of the liver tumor itself would not be expected to be any greater than for the non-transpulmonary approach, and indeed may potentially be lower as the smaller skin-to-target distance would be expected to increase accuracy and decrease the number of attempts required for accurate positioning. However, as noted by Gervais et al. [5], operator confidence and experience in percutaneous biopsy procedure, and particularly those of the thorax, is extremely important.
Other described techniques for approaching liver dome tumors include intrapleural injection of nonconducting fluids such as 5% dextrose, and iatrogenic pneumothorax (anecdotal reports; [11]). Alternatively, non-image-guided approaches to tumors such as the one in this report include laparoscopic radiofrequency ablation; the morbidity and complication profile appear similar to the percutaneous approach in some series. However, the operating costs for the laparoscopic approach would likely be greater given the operating room time and support personnel required.
In conclusion, the transpulmonary approach to liver dome tumors should be considered as an alternative way to approach such tumors for radiofrequency ablation, particularly when the alternative routes are difficult, long, and potentially more dangerous. Further studies in multiple patients are needed to establish the safety of this approach.
References
McGahan JP, Dodd GD, 3rd (2001) Radiofrequency ablation of the liver: current status. AJR Am J Roentgenol 176:3–16
Gazelle GS, Goldberg SN, Solbiati L, Livraghi T (2000) Tumor ablation with radio-frequency energy. Radiology 217:633–646
Lu D, Lee H, Farahani K, Sinha S, Lufkin R (1997) Biopsy of hepatic dome lesions: Semi-real-time coronal MR guidance technique. AJR Am J Roentgenol 168:737–739
van Sonnenberg E, Wittenberg J, Ferrucci JT, Jr, Mueller PR, Simeone JF (1981) Triangulation method for percutaneous needle guidance: The angled approach to upper abdominal masses. AJR Am J Roentgenol 137:757–761
Gervais DA, Gazelle GS, Lu DS, Han PF, Mueller PR (1996) Percutaneous transpulmonary CT-guided liver biopsy: A safe and technically easy approach for lesions located near the diaphragm. AJR Am J Roentgenol 167:482–483
Shankar S, vanSonnenberg E, Silverman SG, Tuncali K, Morrison PR (2003) Management of pneumothorax during percutaneous radiofrequency ablation of a lung tumor: Technical note. J Thorac Imaging 18:106–109
Rhim H, Dodd GD, Chintapalli KN, et al(2004) Radiofrequency thermal ablation of abdominal tumors: Lessons learned from complications. Radiographics 24:41–52
Padhani AR, Scott WWJ (1997) Re: Percutaneous transpulmonary CT guided biopsy. AJR Am J Roentgenol 169:313–314
Lu DS, Raman SS, Vodopich DJ, Wang M, Sayre J, Lassman C (2002) Effect of vessel size on creation of hepatic radiofrequency lesions in pigs: Assessment of the “heat sink” effect. AJR Am J Roentgenol 178:47–51
Ujita M, Ojiri H, Ariizumi M, Tada S (1993) Appearance of the inferior phrenic artery and vein on CT scans of the chest: A CT and cadaveric study. AJR Am J Roentgenol 160:745–747
Farrell MA, Charboneau JW, Callstrom MR, Reading CC, Engen DE, Blute ML (2003) Paranephric water instillation: A technique to prevent bowel injury during percutaneous renal radiofrequency ablation. AJR Am J Roentgenol 181:1315–1317
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shankar, S., Bhargava, P., Habib, F. et al. Transpulmonary CT-Guided Radiofrequency Ablation of Liver Metastasis. Cardiovasc Intervent Radiol 28, 481–484 (2005). https://doi.org/10.1007/s00270-004-4086-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-004-4086-2