
Abstract
Background
Complete mesocolic excision (CME) with central vascular ligation (CVL) is a well-known concept in colon cancer surgery. However, data on the oncological benefits of CVL are scarce. The objective of this study was to evaluate the prognostic significance of the distribution of lymph node metastases (LND) in patients with stage III colon cancer who underwent CME with CVL.
Methods
In total, 446 consecutive patients who underwent curative resection for stage III colon cancer from 2005 to 2011 were analyzed. Patients were classified as having LND1 (metastases in pericolic nodes), LND2 (metastases in intermediate nodes), or LND3 (metastases in main nodes). Survival outcomes were compared among the three groups.
Results
LND1, LND2, and LND3 were identified in 299 (67.0 %), 122 (27.4 %), and 25 (5.6 %) patients, respectively. The 5-year overall survival and relapse-free survival (RFS) of all patients were 86.7 and 76.2 %, respectively. The 5-year RFS of patients with LND1, LND2, and LND3 were 82.8, 65.4, and 52.0 %, respectively (p < 0.0001). Multivariate analysis showed that LND2 was an independent prognostic factor for RFS (p = 0.0185), although the significance of LND3 was marginal (p = 0.0621). Among patients with pN1, the 5-year RFS of patients with LND1 and LND2+3 were significantly different (84.4 vs. 71.5 %, respectively, p = 0.0102), and similar tendency was found between patients with pN2-LND1 and pN2-LND2+3 (72.6 vs. 53.1 %, p = 0.0428).
Conclusion
The high 5-year survival rates of patients with stage III colon cancer, even those with LND2 and LND3, would justify CVL as the standard procedure for advanced colon cancer.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The status of lymph node metastases (LNM) is one of the most important prognostic factors in patients with colorectal cancer, and adequate classification of LNM is critical for predicting prognosis and identifying candidates for adjuvant therapies [1, 2]. Classification of LNM is divided into two main methods: that based on the number of LNM and that based on the distribution of LNM (LND). The current TNM staging system in the seventh edition of the Union for International Cancer Control and American Joint Committee on Cancer [3] is solely based on the number of LNM, although some reports have demonstrated the prognostic importance of the LND [4–8].
Complete mesocolic excision (CME) with central vascular ligation (CVL) in colon cancer surgery was recently introduced as a concept similar to total mesorectal excision in rectal cancer surgery [9, 10]. CME with CVL involves sharp dissection along the embryological planes, ensuring resection of the specimen without damage to the mesocolic fascia and allowing for a high tie of the supplying arteries at their origin. CME with CVL can remove more mesocolon, is more likely to achieve resection in the mesocolic plane, and is associated with better survival rates than is standard excision [10, 11].
Intuitively, patients with node involvement along the major vessels are most likely to benefit from CVL. Therefore, the prognostic information gained from LND has important implications in the era of CME with CVL. To our knowledge, however, limited numbers of reports have addressed these topics. The aim of this study was to investigate the prognostic impact of LND in patients with stage III colon cancer in the era of CME with CVL.
Materials and methods
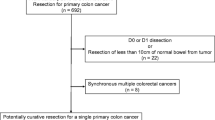
From March 2005 to June 2011, data from 508 consecutive patients who underwent radical resection for pathological stage III colon adenocarcinoma from the cecum to the rectosigmoid were reviewed. Patients with synchronous tumors (n = 36), appendiceal cancer (n = 15), preoperative chemotherapy for locally advanced ascending and rectosigmoid colon cancer (n = 2), familial adenomatous polyposis (n = 3), Lynch syndrome (n = 1), and ulcerative colitis (n = 1) were excluded. Among total residual 450 patients, 4 patients (0.9 %) with a tumor located at the resection margin (R1) were also excluded. Finally, 446 patients were eligible for this study.
All patients underwent open or laparoscopic standardized colectomy and regional lymphadenectomy at our institution according to the tumor location and degree of cancer progression [12–15]. Careful dissection along the embryonic tissue planes was performed to avoid any damage to the visceral fascial layer, based on the concept of CME. CVL was performed in all patients with stage III colon cancer (Fig. 1). After tumor removal, the surgeon identified and isolated the lymph nodes from fresh specimens and recorded both the number and distribution of the retrieved lymph nodes. The lymph node metastatic status was confirmed by pathologists via microscopic examination. In this study, nodal staging was performed according to both the number and distribution of LNM. In accordance with the TNM classification, the pN categories were subdivided into three groups based on the number of LNM: pN1 (metastases in 1–3 nodes), pN2a (metastases in 4–6 nodes), and pN2b (metastases in ≥7 nodes). With respect to LND, the patients were classified as having LND1 (LNM in pericolic lymph nodes), LND2 (LNM in intermediate lymph nodes), or LND3 (LNM in main lymph nodes) according to the Japanese Society for Cancer of the Colon and Rectum classification [16].

Surgical view after central vascular ligation in right hemicolectomy. SMV superior mesenteric vein, SMA superior mesenteric artery, MCA middle colic artery, MCV middle colic vein, RCA right colic artery, ARCV accessory right colic vein, RGEV right gastroepiploic vein, ICA ileocolic artery, ICV ileocolic vein
Statistical analysis was performed using JMP software, version 10.0.2 (SAS Institute, Cary, NC). Summarized data are presented as median values with ranges. Categorical variables were compared using the χ 2 test or Fisher’s exact test where appropriate. Continuous variables were analyzed with the Kruskal–Wallis test. Survival was assessed using the Kaplan–Meier method with the log-rank test. Relapse-free survival (RFS) was defined as the time from surgery to any recurrence. Local recurrence (LR) was defined as tumor recurrence within the bowel wall, regional lymphatic drainage system, or retroperitoneum [9]. All p values of <0.05 were considered statistically significant. Variables with a p value of <0.20 in the univariate analysis were further evaluated in the multivariate analysis using the Cox proportional hazard model to assess the independent predictors for RFS. The results of Cox model analysis are reported using hazard ratios and 95 % confidence intervals.
Results
Our study group comprised 233 (52.2 %) men and 213 (47.8 %) women. The median patient age at the time of the operation was 66 years. In total, 175 (39.2 %) patients had right-sided colon cancer (from the cecum to the distal transverse colon) and 271 (60.8 %) had left-sided colon cancer (from the descending colon to the rectosigmoid colon). The median number of lymph nodes harvested was 17 (range 4–66), and the median number of LNM was 2 (range 1–18). Adjuvant chemotherapy was delivered in 80.3 % of the patients. LND1, LND2, and LND3 were identified in 299 (67.0 %), 122 (27.4 %), and 25 (5.6 %) patients, respectively.
The patients’ clinicopathological factors according to their LND status are shown in Table 1. The preoperative serum CEA level, pT category, pN category, and number of LNM were significantly higher in patients with a higher LND status than in patients with LND1. Open surgery was more frequently performed in patients with a higher LND status than in patients with LND1. With respect to adjuvant chemotherapy, FOLFOX was more frequently performed in patients with a higher LND status than were other chemotherapy regimens.
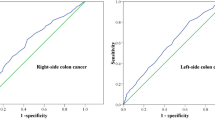
With a median follow-up interval of 60.2 months (range 1.0–103.9 months), the 5-year overall survival (OS), cancer-specific survival (CSS), RFS, and LR rates of all patients in this study were 86.7, 89.1, 76.2, and 2.0 %, respectively. The RFS curves according to the LND status were significantly different: the 5-year RFS of the patients with LND1, LND2, and LND3 were 82.8, 65.4, and 52.0 %, respectively (p < 0.0001) (Fig. 2a). The RFS between patients with LND1 and LND2 was significantly different (p = 0.0001), but the RFS between those with LND2 and LND3 was not (p = 0.3032). The 5-year RFS curves according to the pN categories, based on the number of LNM, also showed similar results: the 5-year RFS of the patients with pN1, pN2a, and pN2b were 81.3, 62.5, and 53.3 %, respectively (p = 0.0001) (Fig. 2b). The RFS between patients with pN1 and pN2a was significantly different (p = 0.0003), but that between patients with pN2a and pN2b was not (p = 0.5321).

Kaplan–Meier curves depicting a relapse-free survival (RFS) according to LND and b RFS according to pN category. c RFS curves of patients with pN1 subdivided into LND1 and LND2+3 and d pN2 subdivided into LND1 and LND2+3
Figure 2c shows the 5-year RFS curves of patients with pN1 subdivided into LND1 and LND2+3. The 5-year RFS of patients with LND1 (n = 258) and LND2+3 (n = 79) among all patients with pN1 was 84.4 and 71.5 %, respectively. The difference between the groups was significant (p = 0.0102). Figure 2d shows the RFS curves of patients with pN2 subdivided into LND1 and LND2+3. The 5-year RFS of patients with LND1 (n = 41) and LND2+3 (n = 68) among all patients with pN2 were 72.6 and 53.1 %, respectively. The difference reached statistical significance (p = 0.0428).
The associations between various clinicopathological factors and RFS are summarized in Table 2. The univariate analysis showed that tumor location, preoperative CEA level, pT category, pN category, LND, and histologic differentiation were significantly associated with RFS. With respect to the relationship between the LND and pN category, each group showed significant overlap, for example, 86 % of patients with LND1 were categorized as having pN1. Therefore, the multivariate analysis was performed separately using the LND or pN category as an independent variable (Table 3). In the multivariate analysis including the LND, LND2 was an independent prognostic factor for RFS (p = 0.0185), but LND3 did not reach statistical significance (p = 0.0621). Additionally, histologic differentiation and the pT4 were independent prognostic factors for RFS. In the multivariate analysis including the pN category, we found that the pN2a, preoperative serum CEA level, histological differentiation, and pT4 were independently associated with RFS.
Discussion
The concept of CME with CVL has rapidly spread worldwide since its recent introduction by Hohenberger et al. [9]. The oncological benefit of CME was demonstrated by West et al. [11], whose multivariate analysis showed that mesocolic resection translated into a significant survival advantage at 5 years compared with surgery in the muscularis propria plane in patients with stage III disease. However, while the advantages of surgery in the mesocolic plane appear obvious, data on oncological benefits of CVL remain scarce. If the numbers of patients with intermediate or main LNM (LND2 or LND3) and their survival rates are low, the estimated oncological benefit of CVL is small. If the situation is reversed, however, the presence of residual cancer cells associated with the performance of low ligation can have a significantly negative impact on survival. Therefore, our data on LND in patients with stage III colon cancer serve as a basis for considering the oncological benefit of CVL for patients with advanced colon cancer.
Although the data on the long-term outcomes after CME with CVL are still limited, Weber et al. [17]. reported a 5-year cancer-related survival rate of 81.8 % in patients with stage III colon cancer who underwent R0 resection from 2000 to 2004 in Erlangen (n = 95). Our 5-year CSS (89.1 %) was higher than that reported by Weber et al. [17]. Most recently, Cho et al. [18]. reported the long-term outcomes of modified CME with CVL for patients with right-sided colon cancer who underwent surgery from 2000 to 2009. They reported 5-year OS, CSS, and RFS rates of 71.0, 73.0, and 68.5 %, respectively, in patients with stage III right-sided colon cancer. Our survival outcomes for patients with stage III right-sided colon cancer (5-year OS, CSS, and RFS rates of 83.5, 84.7, and 70.8 %, respectively) were higher than those reported by Cho et al. [18]. Although the time frames differ and simple comparison is difficult (possibly because of different patient backgrounds), our routine adoption of CME with CVL might lead to improved survival outcomes for patients with stage III colon cancer.
The greatest survival advantage of CVL is expected in patients with LND2 or LND3 because insufficient removal of intermediate or main metastatic lymph nodes by low vascular ligation can result in the presence of residual cancer cells. Because patients with LND2 or LND3 constitute more than 30 % of patients with stage III colon cancer, both CME and CVL should be considered standard surgical procedures for treatment of advanced colon cancer. CME is also much more important in stage III colon cancer than in stage I and II because surgical disruption of the mesocolon is associated with a high risk of spillage of tumor cells in the lymphatic channel, and the benefit obtained by CVL can be canceled out by the disruption of the mesocolon.
In the present study, thirteen (7.4 %) of 175 patients with right-sided colon cancer and 12 (4.4 %) of 271 patients with left-sided colon cancer had LNM located at the origin of each major vessel, and these proportions are within previously reported ranges [2, 4, 5, 7, 19, 20]. The oncological benefit of complete removal of the main lymph nodes in patients with colon cancer has been controversial. Huh et al. [6]. evaluated the prognostic significance of LND in patients with sigmoid colon and rectal cancer and found that the 5-year OS and RFS rates of patients with LND3 sigmoid colon cancer (n = 31) were 35 and 28 %, respectively. Similarly, Kang et al. [21]. reported a 5-year RFS rate of 31.9 % in patients with LND3 sigmoid colon and rectal cancer (n = 33). Kobayashi et al. [19]. estimated the clinical significance of LND in patients with stage III right-sided colon cancer; they found that the 5-year OS and RFS rates of the patients with LND3 were 37.5 and 42.9 %, respectively. In the present study, the 5-year OS and RFS rates of patients with LND3 were 71.5 and 52.0 %, respectively, and our survival outcomes are better than those of previous reports. The better survival outcomes of patients with LND3 in the present study than in previous reports might be partly due to our significantly higher use of an oxaliplatin-based regimen as adjuvant chemotherapy (72 %) in patients with LND3. Furthermore, the recent progress in multimodal approaches after systemic recurrence, including multidrug chemotherapy and aggressive surgical approaches, might have significantly improved the OS in patients with LND3. Because LND3 can only be cured by CVL and better survival can be expected even in patients with LND3 in the current era of multimodal approaches, CVL should be performed to maximize the oncological outcome in patients with stage III colon cancer.
The present study has shown that the LND status is an independent predictive factor for 5-year RFS, although the p value of LND3 did not reach statistical significance. This lack of significance may have been due to the small number of patients with LND3. The hazard ratio for relapse was similar between LND2 and pN2a and between LND3 and pN2b, suggesting that LND is similar to the pN category as a predictor of relapse. Interestingly, patients with pN1 and LND2+3 had a significantly worse RFS rate than did patients with pN1 and LND1, and a similar tendency was found between patients with pN2-LND1 and pN2-LND2+3. Although the number of LNM was <4 (pN1), 23 % of patients were identified as LND2 or 3. Therefore, the addition of the concept of LND to the current nodal staging system might provide more accurate prognostic information and enable appropriate selection for adjuvant chemotherapy in patients with stage III colon cancer.
In the present study, open surgery was more frequently selected in patients with LND2 and LND3. Laparoscopic surgery for colorectal cancer was introduced at our institution in July 2005. Initially, bulky tumors, tumors invading adjacent organs, and LNM in main lymph nodes were excluded as indications for laparoscopic surgery. Therefore, in the early phase of this study, the patients with more advanced disease tended to be treated by open surgery. However, the indications for laparoscopic surgery were gradually extended, as our surgical teams gained greater experience. The laparoscopic ratio increased every year and there are no definite contraindications to laparoscopic surgery at present [22, 23]. This is the reason why patients with a higher LND status were more frequently performed by open surgery.
There are some potential limitations in the present study. First, we have no data on the grading of the plane of mesocolic dissection by pathologists at all because Japanese surgeons isolate the lymph nodes from fresh specimens before pathologic examination. Second, because this was a single-center retrospective study, it is difficult to draw any solid conclusions about the oncological benefit of CVL. Randomized controlled trials comparing CVL versus low ligation for treatment of advanced colon cancer might be necessary to demonstrate the oncological benefit of CVL with a high evidence level, although such a study would be ethically difficult, considering the high survival outcomes of CME with CVL reported by previous studies [17] and the present study. Therefore, despite potential limitations, we believe that our results could serve as a basis for the necessity of performing CVL in patients with advanced colon cancer.
In conclusion, we have demonstrated that LND2 and LND3 were identified in 27.4 and 5.6 % of patients with stage III colon cancer, respectively. The long-term outcomes associated with LND2 or LND3 were worse than those associated with LND1 but better than those in previous reports. The high survival rates of patients with stage III colon cancer, even those with LND2 and LND3, would justify CVL as the standard procedure for advanced colon cancer.
References
Hashiguchi Y, Hase K, Ueno H et al (2010) Prognostic significance of the number of lymph nodes examined in colon cancer surgery: clinical application beyond simple measurement. Ann Surg 251:872–881
Newland RC, Dent OF, Lyttle MN et al (1994) Pathologic determinants of survival associated with colorectal cancer with lymph node metastases. A multivariate analysis of 579 patients. Cancer 73:2076–2082
Edge SB, Compton CC (2010) The American Joint Committee on Cancer: the 7th edition of the AJCC cancer staging manual and the future of TNM. Ann Surg Oncol 17:1471–1474
Kobayashi H, Ueno H, Hashiguchi Y et al (2006) Distribution of lymph node metastasis is a prognostic index in patients with stage III colon cancer. Surgery 139:516–522
Kim CH, Huh JW, Kim HR et al (2014) Prognostic comparison between number and distribution of lymph node metastases in patients with right-sided colon cancer. Ann Surg Oncol 21:1361–1368
Huh JW, Kim YJ, Kim HR (2012) Distribution of lymph node metastases is an independent predictor of survival for sigmoid colon and rectal cancer. Ann Surg 255:70–78
Hida J, Okuno K, Yasutomi M et al (2005) Number versus distribution in classifying regional lymph node metastases from colon cancer. J Am Coll Surg 201:217–222
Yeo K, Kim HH, Kim D et al (2014) A distribution weighted prognostic scoring model for node status in advanced rectal cancer. Cancer Res Treat 46:41–47
Hohenberger W, Weber K, Matzel K et al (2009) Standardized surgery for colonic cancer: complete mesocolic excision and central ligation–technical notes and outcome. Colorectal Dis 11:354–364
West NP, Hohenberger W, Weber K et al (2010) Complete mesocolic excision with central vascular ligation produces an oncologically superior specimen compared with standard surgery for carcinoma of the colon. J Clin Oncol 28:272–278
West NP, Morris EJA, Rotimi O et al (2008) Pathology grading of colon cancer surgical resection and its association with survival: a retrospective observational study. Lancet Oncol 9:857–865
Akiyoshi T, Kuroyanagi H, Fujimoto Y et al (2010) Short-term outcomes of laparoscopic colectomy for transverse colon cancer. J Gastrointest Surg 14:818–823
Akiyoshi T, Kuroyanagi H, Ueno M et al (2011) Learning curve for standardized laparoscopic surgery for colorectal cancer under supervision: a single-center experience. Surg Endosc 25:1409–1414
Akiyoshi T, Kuroyanagi H, Oya M et al (2010) Factors affecting difficulty of laparoscopic surgery for left-sided colon cancer. Surg Endosc 24:2749–2754
Fujimoto Y, Akiyoshi T, Kuroyanagi H et al (2010) Safety and feasibility of laparoscopic intersphincteric resection for very low rectal cancer. J Gastrointest Surg 14:645–650
Japanese Society for cancer of the Colon and Rectum (2009) Japanese classification of colorectal carcinoma, 2nd edn. Kanehara & Co, Tokyo
Weber K, Merkel S, Perrakis A et al (2013) Is there a disadvantage to radical lymph node dissection in colon cancer? Int J Colorectal Dis 28:217–226
Cho MS, Baek SJ, Hur H et al (2014) Modified complete mesocolic excision with central vascular ligation for the treatment of right-sided colon cancer: long-term outcomes and prognostic factors. Ann Surg 00:1–8
Kobayashi H, Enomoto M, Higuchi T et al (2011) Clinical significance of lymph node ratio and location of nodal involvement in patients with right colon cancer. Dig Surg 28:190–197
Kanemitsu Y, Komori K, Kimura K et al (2013) D3 lymph node dissection in right hemicolectomy with a no-touch isolation technique in patients with colon cancer. Dis Colon Rectum 56:815–824
Kang J, Hur H, Min BS et al (2011) Prognostic impact of inferior mesenteric artery lymph node metastasis in colorectal cancer. Ann Surg Oncol 18:704–710
Nagasue Y, Akiyoshi T, Ueno M et al (2013) Laparoscopic versus open multivisceral resection for primary colorectal cancer: comparison of perioperative outcomes. J Gastrointest Surg 17:1299–1305
Nagasaki T, Akiyoshi T, Ueno M et al (2014) Laparoscopic salvage surgery for locally recurrent rectal cancer. J Gastrointest Surg 18:1319–1326
Author contributions
TN and TA contributed to the conception and design of this study. All the authors acquired, analyzed, and interpreted the data. All the authors contributed to drafting the article and to its critical revision. All the authors read and approved the final version.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All the authors have no conflict of interest or financial ties to disclose in association with this study.
Additional information
Toshiya Nagasaki and Takashi Akiyoshi have contributed equally to this work.
Rights and permissions
About this article

Cite this article
Nagasaki, T., Akiyoshi, T., Fujimoto, Y. et al. Prognostic Impact of Distribution of Lymph Node Metastases in Stage III Colon Cancer. World J Surg 39, 3008–3015 (2015). https://doi.org/10.1007/s00268-015-3190-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-015-3190-6