
Abstract
Background
Despite the fact that cholecystectomy is a common surgical procedure, the impact on long-term gastrointestinal quality of life is not fully known.
Methods
All surgical procedures for gallstone disease performed at Mora County Hospital, Sweden, between 2 January 2002 and 2 January 2005, were registered on a standard database form. In 2007, all patients under the age of 80 years at follow-up were requested to fill in a form containing the Gastrointestinal Quality-of-Life Index (GIQLI) questionnaire and a number of additional questions. The outcome was analysed with respect to age, gender, smoking, surgical technique, and original indication for cholecystectomy.
Results
A total of 627 patients (447 women, 180 men) underwent cholecystectomy, including laparoscopic cholecystectomy (N = 524), laparoscopic cholecystectomy converted to open cholecystectomy (N = 43), and open cholecystectomy (N = 60). The mean time between cholecystectomy and follow-up with the questionnaire was 49 months. The participation rate was 79 %. Using multivariate analysis in the form of generalised linear modelling, the original indication for cholecystectomy in combination with gender (p = 0.0042) was found to predict the GIQLI score. Female gender in combination with biliary colic as indication for cholecystectomy correlated with low GIQLI scores. Female gender also correlated with a higher risk for pain in the right upper abdominal quadrant after cholecystectomy (p = 0.028).
Conclusions
We found the original indication for cholecystectomy, together with gender, to predict gastrointestinal symptoms and abdominal pain after cholecystectomy. Careful evaluation of symptoms is important before planning elective cholecystectomy.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Despite the fact that cholecystectomy is a common surgical procedure and a well established treatment for patients with complicated as well as uncomplicated gallstone disease, predicting the benefit on long-term quality of life (QOL) is somewhat difficult. For example, it has been shown that atypical pain location and frequent pain episodes prior to elective cholecystectomy significantly reduces the chance of becoming pain-free postoperatively [1]. At the same time, patients with asymptomatic gallstones are at low long-term risk for developing symptoms eventually leading to cholecystectomy [2, 3].
The prevalence of gallstones is higher in women [4]. The metabolic risk factors for gallstone disease seem to differ between men and women [5]. There is also reason to believe that the clinical manifestations and symptoms related to gallstone disease, and hence outcome after surgery, may differ between genders [6, 7]. The risk for conversion from laparoscopic to open cholecystectomy has been reported to be more than twice as high in men [8]. However, it is not clear to the authors whether the larger number of women undergoing cholecystectomy is solely due to the higher prevalence of gallstone disease, or whether it also reflects a difference in the surgeon’s interpretation of symptoms in men and women.
The Gastrointestinal Quality-of-Life Index (GIQLI) questionnaire has previously been used to show significant long-term improvement in QOL after laparoscopic cholecystectomy for symptomatic gallstone disease [9, 10].
The primary aim of this study was to assess whether factors such as age, gender, smoking, time since cholecystectomy, surgical technique, or indication for cholecystectomy predict gastrointestinal QOL (as measured with the GIQLI questionnaire) or abdominal pain after cholecystectomy. Cosmetic dissatisfaction with the surgical scars was included as a secondary outcome.
Materials and methods
The database
All patients who underwent acute and elective cholecystectomy at Mora District Hospital in Sweden between 2 January 2002 and 2 January 2005 were registered in a local database by the surgeon performing the procedure. Variables registered included gender, Swedish personal registration number, indication for cholecystectomy, duration of surgery, intraoperative hemorrhage, intended surgical approach (open or laparoscopic), and type of surgery finally performed (taking conversion from laparoscopic to open cholecystectomy into account). Length of hospital stay, complications, and the outcome of intraoperative cholangiography were also recorded in the database.
Indications for elective cholecystectomy were repeated attacks of pain in the right upper abdominal quadrant occurring at least 2 times a year and/or recurrent postprandial pain in the upper right abdominal quadrant (grouped together as ‘biliary colic’); secondary complications of the gallstone disease, i.e. acute or previous acute cholecystitis (in this study grouped as ‘cholecystitis’), acute pancreatitis or common bile duct (CBD) stones.
The presence of gallstones confirmed with any imaging method, usually ultrasound, was required. The same indication criteria were applied to both genders but was not absolute, as the database was collected in a clinical setting. The subsequent outcome of microscopic examination of the gallbladder was not permitted to alter the originally entered indication for cholecystectomy in the database.
The questionnaire
To evaluate QOL after cholecystectomy, all patients under the age of 80 years in September 2007 were requested to fill in a questionnaire form sent by mail (with one reminder). The form consisted of the GIQLI questionnaire followed by a small set of non-validated single-item questions including smoking, satisfaction with surgical scars, and the possible presence and location of abdominal pain. In the case of abdominal pain, the specific pain location was marked by the responder on a sketch of the abdomen divided into the four abdominal quadrants.
The GIQLI questionnaire has been translated into Swedish and has been shown to have high reliability and validity for assessing the impact of gallstone disease on QOL [11]. It includes 36 items in five domains: gastrointestinal symptoms (19 items), emotions (five items), physical function (seven items), social function (four items), and side effects of medical treatment (one item). The answer to each item/question is rated from 0 to 4 points, yielding a global score from 0 to 144, where a higher score corresponds to fewer adverse symptoms and thus higher gastrointestinal QOL.
Statistical analysis
The initial statistical analysis was performed using univariate statistics, multivariate regression analysis, and tests for interactions between the predictor variables. For those variables that were identified as possible predictors of the outcome variables, a generalised linear model (GLM) analysis was performed to include interaction effects in the analysis. The GLM analysis was performed as fully factorial (all possible interaction effects included) for the categorical predictor variables, while the scalar predictor variables (time and age measures) were included as linear covariates in the model. If any variable did not show a significant effect on the outcome variable, it was removed from the model, and the reduced model was compared with the previous with the aid of model fit statistics (SPSS Omnibus test) to ensure equal or better statistical model performance.
The reason for using the GLM procedure instead of the more commonly used linear regression procedure was the finding of some complex and significant interactions between the predictor variables, both in predicting the values of each other and in predicting the results of the outcome variables in various combinations with each other.
Data were analyzed using SPSS 16.0 (SPSS Inc., Chicago, IL, USA). Statistical significance was accepted at the p < 0.05 level. Occasional missing answers were replaced with the item median for the items in the GIQLI form unless there were several missing items sequentially (such as a whole page of questions missing), in which case the subject was excluded from the study. For the additional non-validated questions, missing answers were handled simply as missing data.
Results
Of the original 627 patients in the cholecystectomy database, there were 571 patients still alive and below 80 years of age at the time of follow-up with the questionnaire. The median time between cholecystectomy and follow-up was 48 months.
The response rate was 480 of 571 patients (84.1 %). Altogether, 451 patients (327 women and 124 men) chose to participate and completed the questionnaire (participation rate 79.0 %), whereas 29 patients (5.1 %) responded but did not want to or were not cognitively able to participate in the study.
The median age at the time of cholecystectomy of the 451 study participants was 52 years. The non-participants (including the 120 non-responders) were significantly (p = 0.003) younger than the participants, with a median age at the time of cholecystectomy of 45 years. There was no significant difference with respect to gender, surgical technique, or indication for cholecystectomy between the participants and the non-participants.
The database included three patients operated on for gallbladder polyps. None turned out to be malignant upon histopathology examination. Furthermore, two patients had clinically suspected but not verified gallstone disease, where no gallstones were found. These five patients are referred to as ‘other indications’.
Interactions between predictor variables
The distribution of original indications for cholecystectomy varied with gender (Table 1). In the original database of 627 patients, 3.8 times more women than men underwent cholecystectomy for biliary colic (329 women and 87 men, p = 3 × 10−34), but only 1.3 times more women than men underwent cholecystectomy for cholecystitis (90 women and 70 men, p = 0.13). For pancreatitis or CBD stones, there was no difference between the genders (23 women and 23 men).
There was also a clear difference with respect to age between different indications for cholecystectomy (Table 2). For example, the median age of patients who had surgery for biliary colic was 50 years, while the median age of the patients who had surgery for cholecystitis was 59 years (p = 3 × 10−10).
This illustrates the interactions between the predictor variables (gender, age, indication for surgery) in the study and thereby the choice of the GLM procedure in the statistical analyses (as mentioned in the materials and methods section).
GIQLI score after cholecystectomy
Gender, in combination with indication for cholecystectomy was found to correlate with GIQLI score (p = 0.0042, Table 3). Increasing age corresponded with lower GIQLI score, but not significantly (p = 0.055). However, removing age from the statistical model resulted in a poorer model fit.
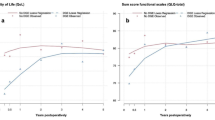
In order to rule out the effect of possible co-morbidity on the result, particularly in the group of patients who had undergone cholecystectomy for pancreatitis, the same analysis was performed comparing only those patients who had undergone cholecystectomy for biliary colic (N = 309) with those who had undergone cholecystectomy for cholecystitis (N = 107). The same general result was achieved, with gender in combination with indication for cholecystectomy predicting the GIQLI score significantly (p = 0.0076). Specifically, female gender and biliary colic as indication for surgery correlated with a lower GIQLI score than female gender and cholecystitis as indication for cholecystectomy. The trend was slightly in the opposite direction for men (Fig. 1). Increasing age significantly (p = 0.016) correlated with lower GIQLI score in this setting.

GIQLI score in relation to indication for cholecystectomy and gender. Gender and indication for cholecystectomy interact in predicting the GIQLI score after cholecystectomy (p = 0.0076). The y-axis is truncated downwards for illustrative purposes. GIQLI Gastrointestinal Quality-of-Life Index
Smoking, time since cholecystectomy, and surgical technique did not correlate with the total GIQLI score.
Abdominal pain after cholecystectomy
Female gender corresponded to a higher risk for pain in the right upper abdominal quadrant (p = 0.028, Table 3, Fig. 2).

Pain in the right upper abdominal quadrant in relation to gender. Gender predicts pain in the right upper abdominal quadrant after cholecystectomy (p = 0.028)
Abdominal pain in any location (pain in one or more of the four abdominal quadrants) was predicted by both indication for cholecystectomy (p = 0.00031, Table 3) and the combination of indication for cholecystectomy and surgical technique (p = 0.016). Specifically, biliary colic as indication for cholecystectomy corresponded to a higher risk for abdominal pain in any location, even more so when in combination with open surgery as surgical technique (Fig. 3a, b, respectively). Only the two major indication groups (biliary colic and cholecystitis, total N = 416) could be included in this analysis due to the remaining groups being too small to allow further analysis (causing an incomplete separation in the dataset).

Abdominal pain, any location, in relation to a indication for cholecystectomy, b surgical method and indication for cholecystectomy. Indication for cholecystectomy predicts abdominal pain after cholecystectomy (p = 0.00031). Indication for cholecystectomy and surgical method interact in predicting abdominal pain after cholecystectomy (p = 0.016)
Smoking, age, and time since cholecystectomy did not correlate with abdominal pain after cholecystectomy.
Cosmetically disturbing scars
Increasing age corresponded to a lower risk for cosmetic dissatisfaction with the surgical scars (p = 3.8 × 10−6, Table 3). Open surgery as surgical technique corresponded to a higher risk for cosmetic dissatisfaction (p = 3.6 × 10−5). However, known intention to perform open surgery (primary open surgical approach) lowered the risk for cosmetic dissatisfaction with the scar (p = 0.019) compared with conversion from laparoscopic to open surgery (Fig. 4).

Cosmetic disturbance from the scars in relation to surgical method. Cosmetic dissatisfaction with the surgical scars after cholecystectomy is predicted both by surgical method actually performed (p = 0.000036) and by the intended surgical method (p = 0.019)
Smoking, indication for cholecystectomy, and time since cholecystectomy did not correlate with cosmetic dissatisfaction.
Due to four missing answers, this analysis was performed on N = 447 individuals.
Discussion
For women, surgery on a relative indication (biliary colic) correlated with a worse outcome (lower GIQLI score) than surgery on a more obvious clinical indication (cholecystitis). Female gender also correlated with a higher risk for pain in the right upper abdominal quadrant after cholecystectomy. Indirectly, this indicates that there could have been a difference in pre-existing gastrointestinal conditions (apart from genuinely gallstone-related symptoms) between men and women in the study. The prevalence of gallstones is known to be higher in women [4, 5]. However, functional causes of abdominal pain, such as irritable bowel syndrome (IBS) [12], are also more common amongst women and could possibly resemble gallstone-related symptoms. It is therefore not unlikely that for a certain proportion of patients in the biliary colic group, cholecystectomy might have had little or no positive effect on gastrointestinal symptoms.
A related topic is gender differences with respect to gallstone complications. Although elective cholecystectomy for biliary colic is more common in women, the number of surgical procedures performed for cholecystitis, pancreatitis, and CBD stones did not differ much with respect to gender in our study (performed in a population-based context). The possibility of gender differences in complicated gallstone disease is illustrated in a previous study [6], showing more extensive inflammation around the gallbladder, higher conversion rate, and more postoperative complications for men than for women. In a study based on the Connecticut Laparoscopic Cholecystectomy Register [13], postoperative mortality was also found to be higher for men than for women.
Satisfaction with surgical scars seemed to correlate with the intended surgical approach, underlining the importance of clearly informing the patient that a need for conversion from laparoscopic to open surgery could arise during the operation.
Due to strong interaction effects, GLM was applied. The results are sometimes difficult to interpret, but the charts (Figs. 1, 2, 3, 4) graphically highlight the findings of the study and also illustrate the ability of GLM to detect and describe interactions in a complex dataset.
A limitation of this study was that the questionnaire was not answered prior to surgery also, so the exact effect of cholecystectomy on the subjects could not be evaluated. Furthermore, it was not possible to assess directly the rates of concomitant co-morbidity in this study.
In conclusion, the possibility of coexisting functional gastrointestinal symptoms should be taken into account when considering surgery for gallstone disease. Distinguishing between functional gastrointestinal symptoms and symptoms related to gallstone disease can sometimes be difficult. In order to achieve adequate expectations, the patient should ideally be informed that there is often only a limited subset of gastrointestinal symptoms that can be attributed to gallstones and that other symptoms may persist after cholecystectomy. In fact, some gastrointestinal symptoms could actually increase or make their debut after cholecystectomy.
References
Halldestam I, Kullman E, Borch K (2008) Defined indications for elective cholecystectomy for gallstone disease. Br J Surg 95:620–626
Halldestam I, Enell EL, Kullman E et al (2004) Development of symptoms and complications in individuals with asymptomatic gallstones. Br J Surg 91(6):734–738
Schmidt M, Hausken T, Glambek I et al (2011) A 24-year controlled follow-up of patients with silent gallstones showed no long-term risk of symptoms or adverse events leading to cholecystectomy. Scand J Gastroenterol 46(7–8):949–954
Borch K, Jönsson K, Zdolsek J et al (1998) Prevalence of gallstone disease in a Swedish population sample. Relations to occupation, childbirth, health status, life style, medications, and blood lipids. Scand J Gastroenterol 33:1219–1225
Sun H, Tang H, Jiang S et al (2009) Gender and metabolic differences of gallstone diseases. World J Gastroenterol 15(15):1886–1891
Botaitis S, Polychronidis A, Pitiakoudis M et al (2008) Does gender affect laparoscopic cholecystectomy? Surg Laparosc Endosc Percutan Tech 18(2):157–161
Quintana JM, Arostegui I, Oribe V et al (2005) Influence of age and gender on quality-of-life outcomes after cholecystectomy. Qual Life Res 14:815–825
Thesbjerg SE, Harboe KM, Bardram L et al (2010) Sex differences in laparoscopic cholecystectomy. Surg Endosc 24(12):3068–3072
Shi HY, Lee HH, Tsai MH et al (2011) Long-term outcomes of laparoscopic cholecystectomy: a prospective piecewise linear regression analysis. Surg Endosc 25(7):2132–2140
Lien HH, Huang CC, Wang PC et al (2010) Changes in quality-of-life following laparoscopic cholecystectomy in adult patients with cholelithiasis. J Gastrointest Surg 14(1):126–130
Sandblom G, Videhult P, Karlson BM et al (2008) Validation of Gastrointestinal Quality of Life Index in Swedish for assessing the impact of gallstones on health-related quality of life. Value Health 12(1):181–184
Cain KC, Jarrett ME, Burr RL et al (2009) Gender differences in gastrointestinal, psychological, and somatic symptoms in irritable bowel syndrome. Dig Dis Sci 54(7):1542–1549
Russell JC, Walsh SJ, Reed-Fourquet L et al (1998) Symptomatic cholelithiasis: a different disease in men? Connecticut laparoscopic cholecystectomy registry. Ann Surg 227:195–200
Funding
Center for Clinical Research, Dalarna, Sweden, and Department of Surgery, Mora Hospital, Sweden.
Conflict of interest
None of the authors has any personal or professional conflict of interest regarding the submitted manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work is originated from Department of Surgery, Örebro University Hospital, Örebro, Sweden.
Rights and permissions
About this article

Cite this article
Wanjura, V., Lundström, P., Österberg, J. et al. Gastrointestinal Quality-of-Life After Cholecystectomy: Indication Predicts Gastrointestinal Symptoms and Abdominal Pain. World J Surg 38, 3075–3081 (2014). https://doi.org/10.1007/s00268-014-2736-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-014-2736-3