
Abstract
Background
Surgeons are scarce in African countries. There is still a need to rely on general practitioners to perform a number of selected procedures. Their training needs to take these facts into consideration. The aim of this study was to evaluate the pattern of surgical procedures performed in a level III institution in an African city. We then analyzed the implications for training.
Methods
This descriptive retrospective study was conducted at the Regional Hospital, Limbe in Cameroon. This hospital had just been selected as the main training hospital for a newly created medical school. The postoperative notes of all procedures performed over 1 year were used to assess exposure of fourth-year medical students to various procedures and how much they matched their educational objectives.
Results
A total of 1,351 procedures were carried out during the study period, including 620 major and 731 minor procedures. Most procedures (84 %) were carried out by a trained specialist. The most frequently performed procedures were cesarean section (n = 131), circumcision (n = 148), laparotomy for various indications (n = 144), appendectomy (n = 81), and hernia repair (n = 81). Analysis of exposure of students to procedures indicated adequate exposure to cesarean section and some selected abdominal procedures.
Conclusions
If students are trained only in our institution, they are likely to perform appendectomy, cesarean section, and hernia repair correctly. Their skills in common orthopedic procedures are likely to be poor. There is need to continue prospects to identify other institutions with a more comprehensive pattern of activities to ensure proper training for students.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The overall surgical workload worldwide is on the rise [1] while the workforce is decreasing [2]. The burden of conditions requiring surgical intervention is not well known in African countries [3].
The workload and nature of procedures performed in surgical units of university teaching hospitals is of interest to medical students, especially those planning to embrace a future surgical career. It is also of interest to residents who need a minimum level of exposure to surgical procedures, heads of departments in building programs, and faculty administrators who are developing curricula.
In sub-Saharan Africa, the challenge of training general practitioners is special as they need to be able at the end of their curriculum to perform a significant number of basic surgical procedures without supervision to meet local needs [4, 5]. This necessity is related to the limited availability of surgeons and anesthetists and their inappropriate territorial distribution [4–6]. This situation has been described in some developed countries as well [7–9].
There is a general tendency to encourage the practice of surgery at the district level, where it is needed, rather than referring cases to tertiary centers [10, 11]. This need has been recognized and included in medical schools at government-run universities in Cameroon. One such school, the Faculty of Health Sciences of University of Buea, located in the South West Region of the Republic of Cameroon, started a training program in general medicine in 2006. One of the goals of the curriculum is to provide the community with graduates who are capable of performing the most common surgical procedures at the district level.
For this school and other medical schools to ensure that this goal is met, students enrolled in this program must have appropriate exposure to surgical procedures, especially those that require immediate action. These cases do not allow the possibility of referral to a center where there is a surgeon.
The aim of this study was to document the surgical procedures carried out at Regional Hospital, Limbe. It analyzed the exposure of fourth-year (first clinical year) medical students to these procedures.
Methods
This descriptive retrospective study was conducted at Regional Hospital, Limbe. This hospital is a level III institution with an emergency and casualty department, an outpatient department, a general surgery unit of 46 beds capacity at the time of the study, and a maternity and gynecology unit of 22 beds capacity. Most surgical procedures are performed in a theater unit with two operating rooms (ORs). Emergency procedures are performed around the clock every day. During the study period, these services were staffed by two general surgeons, two gynecologist-obstetricians, and two senior nurses specialized in anesthesia.
Limbe Regional Hospital is one of the two main newly designated university teaching hospitals attached to the Faculty of Health Sciences of the University of Buea. It received its first groups of medical students for their first clinical year in 2009.
The objectives of the surgical rotation in Buea University were organized as follows.
-
At the end of the curriculum, the graduate is expected to be able to perform correctly the procedures shown in Table 1.
Table 1 Surgical procedures a graduate of University of Buea Medical School is expected to perform at the end of training -
Fourth-year students are expected to observe selected major procedures and perform selected minor procedures under supervision.
-
Fifth-year students are expected to participate actively as first assistant for major procedures and confidently perform minor procedures under supervision.
-
Sixth-year students are expected to perform selected major procedures under supervision.
At this stage, the Limbe regional hospital is used only for the surgical rotation of fourth-year students. Fifth- and sixth-year students are posted to larger hospitals in the city of Douala located some 70 km from Limbe, where more specialized services are found and attendance is more important.
The study covered a period of 1 year, from January 1 to December 31, 2007. The source of information was the register of postoperative notes. All procedures performed in any of the ORs during the study period were included. For each procedure included, information regarding patient’s demographics, indication for operation, nature of the procedure performed, quality of the operator, and type of anesthesia were recorded using a data collection sheet. Procedures were then classified either as major or minor. A procedure was arbitrarily considered major if it required inpatient admission and/or observation for at least 12 h and/or general anesthesia. All other procedures were considered minor. For patients undergoing more than one procedure, each procedure was recorded separately.
The clinical program of our fourth-year medical students includes a rotation of 8 weeks in surgery and a rotation of 8 weeks in obstetrics/gynecology for each group of nine students. During these two rotations (16 weeks in total), students have access to the two ORs. We defined “appropriate exposure” to a procedure as watching it at least 10 times.
Our ORs can accommodate eight students as spectators for each procedure. The total number of times each procedure needed to be performed to satisfy adequate exposure during a rotation was calculated using the following formula.
[18 (no. of students) × 10 (no. of observations required)]/8 (no. of students admitted to the OR for each procedure) = 22.5
Exposure to each procedure was considered adequate if it was performed at least 23 times over a period of 16 weeks. The yearly minimum was then estimated to be 75 times (1 year includes 3.25 periods of 16 weeks). An exposure index was calculated for each procedure or type of procedure by dividing the number of times it was performed in a year by the yearly minimum needed to meet adequate exposure (75). An exposure index of ≥1 was thus considered as appropriate.
“Strengthening the Reporting of Observational Studies in Epidemiology” (STROBE) guidelines were used for reporting the study [12].
Results
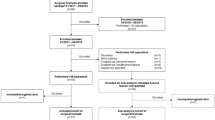
A total of 1,351 procedures were carried out in 1,323 patients during the study period—representing a mean of 113 procedures per month. There were 620 major procedures (52 per month) and 731 minor procedures (61 per month). As shown on Fig. 1, there seemed to be a peak during the months of March, May, and July for major procedures and in January, May, and December for minor procedures.

Monthly distribution of major and minor procedures
Table 2 illustrates the age and sex distribution of our patients for major and minor procedures. It indicates that most patients undergoing a surgical procedure were between 11 and 45 years of age. A large number of procedures were performed in male patients aged ≤5 years (almost always ritual circumcision). Defining patients aged ≤15 years as pediatric cases, the adult/pediatric ratio was 3.48:1. The overall male/female ratio was 0.91. It was 0.66 for major procedures and 1.2 for minor procedures.
Most procedures (n = 713) were performed as an emergency (381 major, 332 minor). There were 638 elective procedures (223 major, 415 minor). In all, 1110 (82.2 %) procedures were performed for a non-injury-related condition.
As shown in Fig. 2, most procedures were carried out by a surgeon or a gynecologist/obstetrician. There seemed to be more involvement of general practitioners in minor procedures. Paramedics also performed a number of minor procedures, mainly ritual circumcision.

Distribution of major and minor procedures by type of operator
The list of all procedures performed during the study period is shown in Table 3. The most commonly performed major procedures included cesarean section, laparotomy for various indications, hernia repair, and appendectomy. The most commonly performed minor procedures included ritual circumcision, wound suture, excision of benign lesions, and uterine revision/dilatation and curettage.
As Fig. 3 illustrates, a vast majority of major procedures were performed either under general or spinal anesthesia. The level of student exposure to general anesthesia, often with endotracheal tube insertion (exposure index 8.44) and spinal anesthesia (exposure index 1.76) was appropriate. Note that a significant number of minor procedures were performed without anesthesia. This was typically the case for ritual circumcision.

Distribution of major and minor procedures according to type of anesthesia used
Figure 4 illustrates the distribution of procedures according to system or specialty involved. Most procedures concerned the digestive system or abdominal wall, the urogenital tract, or obstetrics. It must be emphasized that ritual circumcision performed in 148 patients accounted for more than 44 % of all procedures of the urogenital system.

Distribution of major and minor procedures according to system involved. ENT ear/nose/throat, Resp respiratory, abd abdominal
Table 4 indicates the exposure index for each of the systems involved. There was appropriate exposure to digestive and abdominal wall surgery, urology, obstetrics, and bone and joint surgery.
In Table 5, the exposure index to some of the major procedures indicates appropriate exposure to laparotomy, cesarean section, appendectomy, and hernia repair. The exposure index to some selected minor procedures (Table 6) indicates appropriate exposure to wound suture, excision of an apparently benign lesion, and uterine revision/dilatation and curettage.
Discussion
Overall, 11 % of the world’s disability-adjusted life years (DALYs) are attributable to conditions that can be treated with surgery [13]. More than 234 million major surgical procedures are performed worldwide every year [3]. There is indication that the overall surgical workload is on the rise [1] while the workforce is decreasing [2]. It has been estimated that in United States between 2000 and 2020 the general surgery workload will increase by 35 % for a population increase of 18 % [14]. As a consequence, general surgeons, where available, often have to perform a wide range of procedures, sometimes encroaching on specialties beyond their normal scope [8, 9, 15]. In other areas, nonsurgeons are getting more and more involved in the practice of surgery [4, 5], even in developed countries [16]. In many African countries, this could go as far as including nonphysicians [6, 17].
The distribution of surgeons in the world is extremely variable from one area to another: It was estimated to be around 7/100,000 inhabitants in the United States [18] and less than 0.5/100,000 in many African countries [4, 5].
To date, little is known about the burden of surgical disease in sub-Saharan Africa, especially in rural areas [19]. Despite the fact that it is generally admitted that surgical training should be planned according to demonstrated local needs, these needs are generally poorly documented. A number of studies conducted so far in African countries have analyzed the pattern of practice over years [20–24]. Few have been specifically devoted to analyzing their implications for training [6].
It is generally recommended that surgical services and areas if competence be taken as close as possible to the district level where most of its potential beneficiaries are likely to be found [10, 11]. One of the goals of the medical curriculum in our faculty is to train general practitioners who are able to perform a number of selected procedures at the district level following these recommendations. The type of procedures we include in the clerkship booklets of our fourth-year medical students are comparable to what is usually considered at the reach of a staff with that level of training [6].
It is difficult to estimate the output of surgery in most African countries owing to the poor standardization and the inappropriate reporting already described by other authors [21]. We must admit that in our hospital a number of minor procedures performed in the emergency department under local or no anesthesia—mainly wound suturing and incision/drainage of suppurated lesions—are not registered and thus not reported. This major difficulty, only sometimes reported [25], is a source of bias in this report. On the other hand, a significant number of surgical procedures are performed in other heath facilities within the city of Limbe. They are not accounted for, and any community-based analysis would then be meaningless.
Our empirical definition of “major procedure” is based mainly on the duration of the hospital stay, which is usually contingent on the level of invasiveness of the procedure. Weiser et al. [3] proposed a more precise definition, which likely would include many of the procedures we considered minor. Our aim has been to widen the spectrum of procedures labeled “minor” that could be managed on an ambulatory basis.
We report an approximately equal number of minor and major operations. Similar figures have been previously reported [24, 25], but data in comparable settings usually include a larger number of major procedures [26]. These rates are still far below the rates reported in more developed countries, where 20–35 times more procedures are performed [20–24].
The young and the female are usually those who undergo major procedures in Africa and other low-income settings [4, 22, 25, 27, 28] with a few exceptions regarding the sex distribution [4, 25]. The low rate of pediatric cases (also reported elsewhere [22]) is indicative of little interest in pediatric surgery. These cases tend to be referred to more specialized centers. Children would be expected to be a major point of interest to African surgeons. For example, the cumulated risk of developing a surgical condition by the age of 15 years has been estimated to be >85 % in Gambia [29].
The high rate of emergency procedures are in contrast to the findings of more developed countries, where 80 % of procedures are elective [7]. This could be explained by the absence of a social system for financing health care in most African countries. Most patients come to a health facility only with complications of surgical conditions that require immediate attention at the time they finally decide to consult their physician. A typical example is incarceration of a known hernia.
The rate of patients undergoing general anesthesia is still quite high in Africa. Some authorities believe that this rate could be lowered by better training of existing staff about the use of less-aggressive anesthesia procedures [6].
The types of operations reported in our study are similar to those described in surveys in similar environments [5, 6, 30]. Many of these procedures are generally considered to be at the reach of nonsurgeons [6]. Many authors in black Africa and other low-income countries systematically report cesarean delivery as the most common major surgical procedure [5, 20–22, 24, 27, 28]. It is also one of the most commonly performed in many developed countries [7, 31]. Fingerhut et al. [32] noted that the most common procedures in a developed country were appendectomy and hernia repair, but their study focused on digestive surgery.
The distribution according to the anatomic system involved seems to indicate a low rate of exposure of medical students to orthopedics. Generally, with the exception of some of the emergency procedures on the locomotor system described in our study, orthopedic procedures are generally highly specialized and applicable for referral to more specialized centers [5]. This is true even for developed countries, where orthopedic procedures represent <10 % of operative activities in nonspecialized centers [8, 33, 34]. The rate of urogenital procedures in our study does not reflect the reality as ritual circumcision represented almost 45 % of procedures reported.
Conclusions
There is still much to be done to estimate the real burden of surgical diseases in underdeveloped countries, especially in sub-Saharan Africa. Available data seem to indicate clearly a severe shortage of surgeons in African countries. It is likely that a vast majority of patients in need of surgical services are not attended to in the absence of health insurance and social security.
There is, then, still a need to rely on general practitioners for a number of selected procedures that ideally are performed at the district level. It is recognized, however, that district hospitals are currently unable to meet the real surgical needs of the populations they serve [19].
Our new teaching hospital has the potential to provide students with appropriate exposure to cesarean section and abdominal surgical procedures, especially appendectomy and hernia repair, according to local standards. There is still a need to identify means of improving the exposure of students to emergency procedures for trauma and pediatric surgery.
There is also a clear need for further population-based research to assess the real output of surgery and the availability of surgical services in terms of equipment and manpower in African countries. Urgently needed also is the will to apply such analyses to implications for training medical students before programs or curricula are established.
References
Shoemaker CP Jr (2003) Changes in the general surgical workload, 1991–1999. Arch Surg 138:417–426
Stevermer JJ, Supattanasiri GJ, Williamson H Jr (2001) A survey of general surgeons in rural Missouri: potential for rapid decrease in work force. J Rural Health 17:59–62
Weiser TG, Regenbogen SE, Thompson KD et al (2008) An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet 372:139–144
Loutfi A, Pickering JL (1993) The spectrum of surgery in Ethiopia. Can J Surg 36:91–95
Lavy C, Tindall A, Steinlechner C et al (2007) Surgery in Malawi: a national survey of activity in rural and urban hospitals. Ann R Coll Surg Engl 89:722–724
Watters DA, Bayley AC (1987) Training doctors and surgeons to meet the surgical needs of Africa. Br Med J (Clin Res Ed) 295:761–763
Humber N, Frecker T (2008) Rural surgery in British Columbia: is there anybody out there? Can J Surg 51:179–184
Breon TA, Scott-Conner CE, Tracy RD (2003) Spectrum of general surgery in rural Iowa. Curr Surg 60:94–99
Tulloh B, Clifforth S, Miller I (2001) Caseload in rural general surgical practice and implications for training. ANZ J Surg 71:215–217
World Health Organization (2003) Surgical Care at the District Hospital. WHO, Geneva
Voss M, Duvenage R (2011) Operative surgery at the district hospital. S Afr Med J 101:521–522
Von Elm E, Altman DG, Egger M et al (2007) The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet 370:1453–1457
Myles PS, Haller G (2010) Global distribution of access to surgical services. Lancet 376:1027–1028
Liu JH, Etzioni DA, O’Connell JB et al (2004) The increasing workload of general surgery. Arch Surg 139:423–428
Hyman N (2002) How much colorectal surgery do general surgeons do? J Am Coll Surg 194:37–39
Humber N, Frecker T (2008) Delivery models of rural surgical services in British Columbia (1996–2005): are general practitioner-surgeons still part of the picture? Can J Surg 51:173–178
Wilhelm TJ, Thawe IK, Mwatibu B et al (2011) Efficacy of major general surgery performed by non-physician clinicians at a central hospital in Malawi. Trop Dr 41:71–75
Thompson MJ, Lynge DC, Larson EH et al (2005) Characterizing the general surgery workforce in rural America. Arch Surg 140:74–79
Grimes CE, Law RS, Borgstein ES et al (2012) Systematic review of met and unmet need of surgical disease in rural sub-Saharan Africa. World J Surg 36:8–23. doi:10.1007/s00268-011-1330-1
Nordberg E, Mwobobia I, Muniu E (2002) Major and minor surgery output at district level in Kenya: review and issues in need of further research. Afr J Health Sci 9:17–25
Nordberg E (1990) Surgical operations in eastern Africa: a review with conclusions regarding the need for further research. East Afr Med J 67(Suppl):1–28
Nordberg E, Holmberg S, Kiugu S (1996) Rates of major surgery by age and sex in a rural district in Kenya. Ann Trop Med Parasitol 90:213–221
Nordberg E, Mwobobia I, Muniu E (2001) Minor surgery at hospitals and clinics in a Kenyan district. East Afr Med J 78:102–106
Nordberg E, Hofman J (1994) Major and minor surgery at a rural African hospital. J Trop Med Hyg 97:138–144
Padrón-Arredondo G (2006) General surgery in a rural hospital in the state of Quintana Roo, Mexico. Cir Cir 74:115–120
Nabembezi JS, Nordberg E (2001) Surgical output in Kibaale district, Uganda. East Afr Med J 78:379–381
Damien P, Nabare C, Baiden F et al (2011) How are surgical theatres in rural Africa utilized? A review of 5 years of services at a district hospital in Ghana. Trop Dr 41:91–95
Rodríguez-Paz CA, González-De Blas Jde J, Carreón-Bringas RM (2009) Surgical experience and statistics at a rural hospital in San Luis Potosí, Mexico. Cir Cir 77:115–119
Bickler SW, Telfer ML, Sanno-Duanda B (2003) Need for paediatric surgery care in an urban area of The Gambia. Trop Dr 33:91–94
Blanchard RJ, Blanchard ME, Toussignant P et al (1987) The epidemiology and spectrum of surgical care in district hospitals of Pakistan. Am J Public Health 77:1439–1445
Rutkow IM (1987) Surgical operations in the United States: 1979 to 1984. Surgery 101:192–200
Fingerhut A, Hay JM, Millat B et al (1998) General and gastrointestinal tract surgery in France. Arch Surg 133:568–574
Sariego J (1999) Patterns of surgical practice in a small rural hospital. J Am Coll Surg 189:8–10
Landercasper J, Bintz M, Cogbill TH et al (1997) Spectrum of general surgery in rural America. Arch Surg 132:494–496
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chichom Mefire, A., Atashili, J. & Mbuagbaw, J. Pattern of Surgical Practice in a Regional Hospital in Cameroon and Implications for Training. World J Surg 37, 2101–2108 (2013). https://doi.org/10.1007/s00268-013-2116-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-013-2116-4