
Abstract
Background
The prognostic significance of lymph node metastases (LNM) in follicle cell-derived differentiated thyroid carcinoma (DTC) is still controversial. The management of cervical lymph nodes varies from “berry picking” to modified radical neck dissection (MRND). The incidence of LNM in papillary thyroid carcinoma varies from 27% to 80%. The importance of sentinel lymph node (SLN) biopsy for decisions about the surgical management of lymph nodes in DTC has been the subject of several previous studies.
Patients and Methods
In 40 patients with DTC methylene blue dye was applied peritumorally. Both SLN and non-SLN in the lower third of the jugulo-carotid chain were dissected prior to total thyroidectomy and routine dissection of the central neck compartment and examined by frozen-section and standard histology. MRND was performed in 9 cases of LNM in the lateral neck compartment.
Results
The SLN identification rate was 92.5%. Metastases in SLNs were revealed by frozen-section histology in 7 cases, leading to immediate MRND. The findings were confirmed on standard HE examination. In 2 false-negative cases SLN metastases were revealed on standard histology and MRND was performed 1 week later. The specificity of the method was 100%, sensitivity 77.7%, negative predictive value 94%, positive predictive value 100%, with overall accuracy of 95%.
Conclusion
Our results seem to imply that SLN biopsy in the jugulo-carotid chain using methylene blue dye mapping may be a feasible and valuable method for estimating lymph node status in the lateral neck compartment. It may be helpful in the detection of true-positive but nonpalpable lymph nodes, and in such cases may support the decision to perform MRND in patients with DTC.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The prognostic value of lymph node metastases (LNM) in differentiated thyroid carcinoma (DTC) is still controversial. Large retrospective studies have analyzed the prognostic influence of LNM. Some have shown that LNM are not associated with a decrease in survival.1,2 Other studies indicate that LNM increases the risk of locoregional relapse and may influence cancer-specific survival in some patients with papillary carcinoma.3–9
The reported incidence of LNM without evidence of gross cervical lymph node involvement in papillary thyroid carcinoma varies from 27% to more than 80%.9–12 Such differences in the incidence of LNM are the result of different approaches in the management of neck lymph nodes, which vary from “berry picking” to elective modified radical neck dissections (MRND). Although the management of neck lymph nodes has not always been standardized, it is generally recommended that in the presence of metastatic nodes the operative procedure should comprise MRND.13
The concept of sentinel lymph nodes (SLN) as the first node(s) to receive drainage from a tumor was introduced by Ramon Cabanas14 and later well established in skin melanoma15 and breast cancer.16,17 Controversies in the surgical management of lymph nodes in DTC, have led some authors to propose that SLN should be sampled in patients with thyroid cancer to support the decision whether to perform lymph node dissection or not. The technique is feasible and safe and may be used to select patients with true positive lymph nodes for selective lymph node dissection.18–24
Considering the results of previous studies of SLN biopsy in DTC, the objective of this study was to determine whether SLN biopsy of the first draining node(s) in the jugulo-carotid chain is an accurate technique to select patients with true-positive but nonpalpable lymph nodes for selective MRND.
PATIENTS AND METHODS
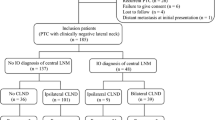
From January 2001 to February 2004, 40 patients with DTC underwent SLN biopsy in the lower jugulo-carotid chain. Preoperatively, all patients had clinical examination for suspicious thyroid tumors, ultrasonography of the neck and abdomen, fine needle aspiration biopsy, Tc99m scintigraphy of the neck, chest X-ray, and blood tests of thyroid hormones, thyrotrophin (TSH), serum thyroglobulin, and anti-thyroglobulin antibody levels. All patients signed an informed consent form. Patients with intrathyroid tumors and clinically non-enlarged lymph nodes (N0) were included in the study. Patients with locally invasive tumors (pT4), gross LNM in the neck, initial distant metastases, and with a history of allergic reactions to drugs were excluded.
The median age at diagnosis was 42 years (range 23–57), and there were 30 women and 10 men.
Detailed Surgical Procedure
The skin incision for thyroidectomy was made horizontally, 2 cm above the jugular notch. After preparing the myocutaneous flaps, the infrahyoid muscles were divided in the midline and separated, laterally from the thyroid gland. Before mobilization of the gland, approximately 0.2 ml of 1% methylene blue dye was injected peritumorally with a 27-gauge needle. In cases of bilateral tumors dye was injected into both lobes. No structures had been cut so far. Immediately after the lobe was stained, connective tissue between the sternohyoid and sternocleidomastoid muscles was sharply divided and the internal jugular vein exposed looking for the blue-stained lymphatic vessels and lymph nodes in the jugulo-carotid chain. After approximately 10 minutes the dissection was continued above and beyond the omohyoid muscle, toward the internal jugular vein and common carotid artery until the blue-stained lymph nodes were found and recognized as SLNs. If there were no stained nodes, the first node closest to the afferently stained lymphatic vessel was considered to be the SLN. An extended dissection of the surrounding non-SLNs above and beyond the omohyoid muscle was performed. In cases of multifocal, bilateral tumors the procedure was conducted on both sides. All dissected nodes were examined by frozen section and conventional (hematoxylin eosin [HE]) histopathological examination. If any of the nodes were positive on the frozen section, MRND was performed in the same operation after total thyroidectomy and dissection of the central neck compartment. In 2 false-negative cases of SLNs (negative findings on frozen-section examination but positive on conventional histopathological examination) after HE staining, and immunohistochemistry for thyroglobulin (anti-thyroglobulin antibody; DAKO, Copenhagen, Denmark; dilution 1:100; visualization LSAB+), MRND was performed as a reoperative procedure after 1 week.
After SLN biopsy, total thyroidectomy with dissection of the central neck compartment and clearance of pretracheal and paratracheal nodes was routinely performed. Prior to total thyroidectomy, all parathyroid glands were preserved on venous-arterial stalks and both recurrent laryngeal nerves were identified and followed to the entrance into the larynx. All thyroid glands and lymph node specimens were sent for conventional histopathological examination. There were no complications after surgery.
RESULTS
Among the 40 patients with DTC, papillary carcinoma was found in 34, Hürthle cell carcinoma in 5, and follicular carcinoma in 1 patient. Median tumor size was 15 mm. Fifteen patients had tumors less than 10 mm in diameter (pT1, microcarcinoma), 21 had tumors measuring 11–40 mm (pT2) and 4 patients had tumors greater than 40 mm in diameter (pT3). In 25 cases thyroid tumors were solitary, while multifocality was found in 15 cases. Tumor localization was as follows: in 1 lobe—23, in the isthmus—2, and multifocal in 15 cases (Table 1).
Identification and biopsy of blue-stained SLN in the ipsilateral jugulo-carotid chain was successful in 37 out of 40 cases. The identification rate (IR) of SLN was 92.5%. The median number of SNLs per draining area was 3 (mean 3.2).
In 7 cases, frozen section analysis of SLNs revealed metastases of the papillary thyroid carcinoma. The average number of LNM per draining area was 2.1. In all 7 cases metastases were also verified by conventional histopathology (HE staining). Metastases were also found in non-SLNs, obtained by MRND. In 2 cases out of 15 multifocal papillary carcinomas, we found bilateral jugulo-carotid LNM, and bilateral MRND was carried out after total thyroidectomy and dissection of the central neck compartment.
In 33 cases, SLNs were negative for metastases on frozen section examination. In 2 of these cases with papillary carcinoma, micrometastases in SLNs were revealed by conventional histopathology (HE staining) as well as immunohistochemical staining with anti-thyroglobulin antibody. In these patients metastases were revealed in 2 out of 4 SLNs in 1 patient, and in 1 out of 3 SLNs in the other patient. Further analysis revealed no metastases in other jugulo-carotid SLNs and non-SLNs obtained during the same operation. The findings indicate a rate of 6% false-negative results for the detection of micrometastases if nodes were initially negative for metastases on frozen section analysis.
In this study LNM in the lateral neck compartment were detected in 9 out of 40 patients with papillary thyroid carcinoma. In all cases therapeutic MRND was performed following total thyroidectomy with routine dissection of the central neck compartment. In 7 cases, which were positive on frozen section analysis, MRND was performed during the first operation, while in 2 false-negative cases, MRND was performed after 1 week when results of a conventional histopathological examination were available. In 5 cases of Hürthle cell carcinoma and in 1 follicular carcinoma we found no LNM in any of the dissected lymph nodes.
We found the IR of 92.5% (37 out of 40), with specificity (Sp) of 100% (31 out of 31) and sensitivity (Se) of 77.7% (7 out of 9). Negative predictive value (NPV) was 94% (31 out of 33), and positive predictive value (PPV) was 100% (7 out of 7), while overall accuracy of the method was 95% (38 out of 40; Table 2).
DISCUSSION
Surgery remains the therapy of choice for DTC in order to eradicate all tumor foci, and thereby reduce recurrence and mortality rates, facilitate postoperative I131 therapy, improve sensitivity of serum thyroglobulin measurement, and provide good quality of life. However, the extent of surgery has been a matter of discussion and should be dictated by stage of disease and prognostic factors.
Most authors suggested total or near total thyroidectomy for the majority of patients with DTC. 1,3,11,12 Cady2 claimed that younger patients with favorable prognostic factors may require only ipsilateral lobectomy.
Large retrospective studies have analyzed the prognostic influence of LNM. Some have shown that LNM are not associated with a decrease in survival and doubt the clinical significance of occult nodal disease.1,2 Other reports have shown that LNM have been associated with increased locoregional recurrence rates and may predict systemic disease and decreased survival in some patients with papillary carcinoma.3–9
Recommendations on the management of neck lymph nodes in patients with DTC have varied from simple removal of palpably enlarged nodes to routine central compartment dissection and elective MRND. But there is no consensus on the management of nonpalpable lymph nodes. In patients with papillary thyroid carcinoma the incidence of preoperatively and intraoperatively detected enlarged lymph nodes (27%–45%) has been markedly lower than the incidence of histologically confirmed LNM revealed by routine bilateral neck dissection, which has been as high as 80% in adults and 90% in children.9–12 Approximately the same incidence of lymph node involvement has been revealed in central and lateral neck compartments,8 and as many as 10%–24% of cases have had bilateral involvement.25 It has been shown that metastases in the lower third of the jugulo-carotid chain have a high predictive value (over 80%) for metastases in the upper two-thirds of the chain and for such cases with a high risk of nodal recurrence, some authors suggest routine, even bilateral MRND. 12,25–28
Considering these controversies, some authors have proposed to perform SLN biopsy in patients with DTC.
Therefore, different methods of lymphatic mapping (blue dye, radiocolloid) have been used so far. Kelemen and colleagues first applied the concept of SLN in 17 thyroid malignancies using patent blue V vital dye. The identification ratio was 88.2%, due to two retrosternal localized SLN, and false-negative cases constituted 8%.18 Fukui and coworkers analyzed the methylene blue staining of SLN in 22 patients with papillary thyroid carcinoma. IR was 95.5%, with 14.3% false-negative investigations. The authors reported that the sensitivity of the method was 77.8%, the Sp 100%, the NPV 90.4%, while the PPV was 100%, with an overall accuracy of the method of 86.3%.19
Arch-Ferrer et al. tested the method of isosulfan blue dye staining in 22 patients with PTC. The authors found an IR of 91%, with a false-negative proportion of 25% and Sp 100%, Se 71%, NPV 37%, and PPV 100%. Using immunohistochemistry for cytokeratin-7 (CK-7; DAKO) all values reached 100%, and the authors suggested that all SLN, which were negative on frozen section using the HE method, should be examined with immunohistochemistry for CK-7 intraoperatively.20
Catarci and coworkers performed a combined technique of SLN mapping in 6 cases of PTC. The overall IR using vital dye (patent blue V), preoperative lymphoscintigraphy (99mTc-labeled colloidal albumin), and intraoperative hand-held gamma probe detection was 100%, while IR was 66%, 50%, and 83% for each of the methods respectively. 21
In a recent study, Takami et al. 22 showed that SLN nodes were identified in 63 of 68 patients (92.6%) investigated with the use of isosulfan blue dye. There was concordance between the SLN status and the final regional lymph node status in 58 of the 63 patients (92.1%). There were 5 false-negative cases. SLN biopsy had a Se of 87.5% (35 out of 40), Sp of 100% (23 out of 23), PPV of 100% (35 out of 35), NPV of 82.1% (23 out of 28), and accuracy of 92.1% (58 out of 63). Similar results have been shown by Tsugawa et al., 23 who concluded that the SLN biopsy was available on detection of nonpalpable nodal metastases, underlining the need for further experience and refinement.
In a critical review, Wiseman et al. 29 summarized the results of several studies and found that the average rate of SLN identification was 91% (66%–100%) and when identified, the SLN accurately predicted the disease status of the neck in most patients (80%–100%).
Overall, the previous studies have shown that stained SLNs were found in the central or lateral neck compartments, or both. Taking into consideration these findings, our study was designed to trace the blue-stained nodes in the jugulo-carotid chain in respect of the fact that we routinely perform dissection of the central neck compartment in cases of DTC. The SLN biopsy was performed approximately 10 minutes after the injection of blue dye, while the color flowed into the jugulo-carotid lymph nodes.
In our study we used 1% methylene blue dye for intraoperative lymphatic mapping in 40 cases of DTC. IR was 92.5% with a false-negative rate of 6% (2 out of 33). The Sp of the method was 100%, the Se 77.7%, the NPV was 94% (31 out of 33), and the PPV 100% (7 out of 7), while overall accuracy was 95% (38 out of 40). However, the accuracy of detection of SLN in the central neck compartment was not evaluated since we routinely perform total thyroidectomy with central compartment dissection in patients with DTC.
When using methylene blue instead of Patent blue V, we took into consideration the lower incidence of peroperative allergic reactions as well as the lower price.30,31
At the time of dissection the majority of nodes in the central neck compartment were stained blue. This was helpful for more precise visualization of lymph nodes and also simplified discrimination from parathyroid glands. Nevertheless, Dixon et al. 24 reported staining of previously identified parathyroid gland in 1 out of 40 cases of SLN biopsy.
The results indicate that immunohistochemical staining with anti-thyroglobulin antibodies may increase the sensitivity for detection of LNM. This is required only when micrometastases are suspected on HE staining.
CONCLUSIONS
According to previous data, the status of the lower jugulo-carotid lymph nodes significantly predicts the status in the upper two-thirds of the chain. Our results imply that SLN biopsy in the lower jugulo-carotid chain using methylene blue dye mapping is a feasible, safe, and accurate method of estimating lymph node status in the lateral neck compartment. The method may be helpful in the detection of true-positive but nonpalpable lymph nodes and may support a decision to perform a selective MRND in patients with DTC.
References
Mazzaferri EL. Long-term outcome of patients with differentiated thyroid carcinoma: effect of therapy. Endocr Pract 2000;6:469–476
Cady B. Presidential address: beyond risk groups—a new look at differentiated thyroid cancer. Surgery 1998;124:947–957
Noguchi S, Yamashita H, et al. Changing trend of presentation of papillary carcinoma of the thyroid in the last 5 decades: experience in one institution. Int J Cancer 2002;13:216
Shaha AR. Thyroid cancer: extent of thyroidectomy. Cancer Control 2000;7:240–245
McHenry CR, Rosen IB, Walfish PG. Prospective management of nodal metastases in differentiated thyroid cancer. Am J Surg 1991;162:353–356
Akslen LA, Haldorsen T, Thoresen SO, et al. Survival and causes of death in thyroid cancer: a population-based study of 2479 cases from Norway. Cancer Res 1991;51:1234–1241
Ozaki O, Ito K, Kobayashi K, et al. Modified neck dissection for patients with nonadvanced, differentiated carcinoma of the thyroid. World J Surg 1988;12:825–829
Attie JN. Modified neck dissection in treatment of thyroid cancer: a safe procedure. Eur J Cancer 1988;24:315–324
Hay ID, Bergstralh EJ, Goellner JR, et al. Predicting outcome in papillary thyroid carcinoma: development of a reliable prognostic scoring system in a cohort of 1779 patients surgically treated at one institution during 1940 through 1989. Surgery 1999;114:1050–1058
Noguchi S, Murakami S, Yamashita H, et al. Papillary thyroid carcinoma. Modified radical neck dissection improves prognosis. Arch Surg 1998;133:276–280
Tubiana M, Schlumberger M, Rougier P, et al. Long-term results and prognostic factors in patients with differentiated thyroid carcinoma. Cancer 1985;55:794–804
Lacour J, L’Heritier M, Petit JY, et al. Surgical treatment of differentiated thyroid cancer at the Institut Gustave-Roussy. Ann Radiol (Paris) 1977;20:767–770
Scheumenn GFW, Gimm O, Wegner G, et al. Prognostic significance and surgical management of locoregional lymph node metastases in papillary thyroid cancer. World J Surg 1994;18:559–567
Cabanas RM. An approach for the treatment of penile carcinoma. Cancer 1977;39:456–466
Morton DL, Wen D-R, Wong JH, et al. Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg 1992;127:392–399
Giuliano AE, Kirgan DM, Guenther JM, et al. Lymphatic mapping and sentinel lymphadenectomy for breast cancer. Ann Surg 1994;220:391–401
Krag DN, Weaver DL, Alex JC, et al. Surgical resection and radio localisation of the sentinel node in breast cancer using gamma probe. Surg Oncol 1993;2:335–340
Kelemen PR, Van Herle AJ, Giuliano AE. Sentinel lymphadenectomy in thyroid malignant neoplasms. Arch Surg 1998;133:288–292
Fukui Y, Yamakawa T, Taniki T, et al. Sentinel lymph node biopsy in patients with papillary thyroid carcinoma. Cancer 2001;92:2868–2874
Arch-Ferrer J, Velazquez D, Fajardo R, et al. Accuracy of sentinel lymph node in papillary thyroid carcinoma. Surgery 2000;130:907–913
Catarci M, Zaraca F, Angeloni R, et al. Preoperative lymphoscintigraphy and sentinel lymph node biopsy in papillary thyroid carcinoma. A pilot study. J Surg Oncol 2001;77:21–24
Takami H, Sasaki K, Ikeda Y, et al. Detection of sentinel lymph nodes in patients with papillary thyroid cancer. Asian J Surg 2003;26:145–148
Tsugawa K, Ohnishi I, Nakamura M, et al. Intraoperative lymphatic mapping and sentinel lymph node biopsy in patients with papillary carcinoma of the thyroid gland. Biomed Pharmacother 2002;56(Suppl 1):100–103
Dixon E, McKinnon JG, Pasieka JL. Feasibility of sentinel lymph node biopsy and lymphatic mapping in nodular thyroid neoplasms. World J Surg 2000;24:1396–1401
Mirallie E, Visset J, Sagan C, et al. Localization of cervical node metastasis of papillary thyroid carcinoma. World J Surg 1999;23(9):970–973
Noguchi M, Kumaki T, Taniya T, et al. Bilateral cervical lymph node metastases in well-differentiated thyroid cancer. Arch Surg 1990;125:804–806
Noguchi S, Murakami N. The value of lymph-node dissection in patients with differentiated thyroid cancer. Surg Clin North Am 1987;67:251–261
Ohshima A, Yamashita H, Noguchi S, et al. Indications for bilateral modified radical neck dissection in patients with papillary carcinoma of the thyroid. Arch Surg 2000;135:1194–1198; discussion 1199
Wiseman S, Hicks W, Chu Q, et al. Sentinel lymph node biopsy in staging of differentiated thyroid cancer: a critical review. Surg Oncol 2002;11:137–142
Simmons R, Thevarajah S, Brennan MB, et al. Methylene blue dye as an alternative to isosulfan blue dye for sentinel lymph node localization. Ann Surg Oncol 2003;10:242–247
Cimmino VM, Brown AC, Szocik JF, Pass HA, Moline S, De SK, Domino EF. Allergic reactions to isosulfan blue during sentinel node biopsy—a common event. Surgery 2001;130:439–442
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article is available at http://dx.doi.org/10.1007/s00268-006-1001-9.
Rights and permissions
About this article
Cite this article
Dzodic, R. Sentinel Lymph Node Biopsy May Be Used to Support the Decision to Perform Modified Radical Neck Dissection in Differentiated Thyroid Carcinoma. World J. Surg. 30, 841–846 (2006). https://doi.org/10.1007/s00268-005-0298-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-005-0298-0