
Abstract
Nitric oxide is a short-lived free radical that acts at the molecular, cellular, and physiologic level. Since its discovery almost 20 years ago it has proven itself as an important element in wound healing. This review highlights many of the important aspects of nitric oxide in wound healing, including a review of the basic biology of nitric oxide, its role as part of the cytokine cascade and as a promoter of angiogenesis, as well as its more recently elucidated role in apoptosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
It has been known for over 20 years that arginine enhances wound collagen synthesis and wound breaking strength during normal and impaired healing. The exact mechanism of action is not known, but it is under intense study. One avenue that our laboratory has pursued is to study the expression and activity of the various metabolic pathways of arginine within the wound (Fig. 1). We know that wound arginine is metabolized via both the nitric oxide (NO) synthesis pathway and the urea synthesis pathway. The temporal expression and regulation of these degradative pathways may well explain the biological and pharmacological effect of arginine on wound healing. This article examines the current status of knowledge concerning the role of wound nitric oxide synthesis.

Arginine metabolism in wounds.
Nitric Oxide is a short-lived free radical formed from the terminal guanidino nitrogen atom of arginine. The guanidino nitrogen accepts five electrons in an oxidation process requiring molecular oxygen, resulting in formation of NO and citrulline. Nitric oxide synthases, the enzymes responsible for this conversion, are homodimeric flavoprotein enzymes (130–150 kDA subunits). Tetrahydrobiopterin, flavine mononucleotide (FMN), flavine adenine dinucleotide (FAD), nicotinamide-adenine-dinucleotide phosphate (NADPH), and oxygen are required as co-factors for full activity [1]. The NO synthases exist in three distinct isoforms, two constitutive (endothelial and neuronal) isoforms and one inducible isoform. The constitutive isoforms are permanently active, generating low concentrations of NO, and they are regulated by intracellular calcium fluxes or exogenous calmodulin. The expression, transcription, and function of the inducible isoform (iNOS) is induced by a variety of cytokines, growth factors, and inflammatory stimuli on target cells; their action leads to release of high levels of NO over and above the amounts generated by the constitutive isoforms.
The high amounts of NO formed by the inducible isoform account for some of its detrimental effects in inflammatory situations such as sepsis [2]. The inducible isoform of NO is also expressed during wound healing, burn injury, endotoxin exposure, arthritis, and inflammatory bowel diseases.
NO Expression in Healing Wounds
Levels of arginine, a semi-essential amino acid [3], become critically low after wounding. Arginase levels are high in wound fluid, and they increase with the age of the wound. Thus arginine competes with iNOS for substrate and may downregulate NO synthesis during wound healing. Indeed, NO synthesis in macrophages can be impaired by arginine consumption by arginase [4]. To date there are no data, however, on the interaction and competition of these two alternate pathways and their affects on wound healing. It should be noted that l-hydroxy-arginine and nitrite, the intermediate and end products, respectively, of NO synthesis, are both strong arginase inhibitors [5, 6]. Furthermore, urea, the end product of arginase activity, inhibits NO formation [7]. Distinct cytokines favor the various degradative pathways. For example, transforming growth factor-beta (TGF-β) and interleukin-4 (IL-4) increase arginase and inhibit iNOS activity, whereas gamma-interferon (IFN-γ), IL-1, and lipopolysaccharide(LPS) work inversely [8, 9, 10].
Because NO is difficult to measure directly, stable metabolites are used as surrogates for NO formation. Nitrite and nitrate, two widely used stable end products, can be measured in wound fluid [11]. However, these measurements should not be translated as equimolar formation of NO because non-enzymatic NO formation can occur [12]. Several other direct or indirect detection methods can be performed, such as immunohistochemistry, direct measurement of enzyme content and/or activity, peroxynitrite formation in tissue, gene expression and others. However, no study to date has investigated arginine kinetics after wounding taking into account local and systemic arginine metabolism [13, 14].
Before NO was known, Albina et al. investigated arginine metabolism in wounds and demonstrated increased citrulline formation, which was imputed to an arginine deiminase-like activity [15]. Up until that report, this pathway of arginine disposal had been described only in bacteria and fungi. Subsequently, generation of NO during wound healing was deduced by demonstrating increased urinary nitrate secretion after wounding [16]. Thereafter several studies confirmed these data and extended the findings to healing after burn injury [17, 18]. In these models, urinary nitrate levels remained elevated until complete healing had occurred. Later experiments confirmed that the highest NOS activity occurs during the early phases of wound healing [19].
With a polyvinyl alcohol sponge model in rats, a progressive accumulation of nitrate/nitrite in wound fluid can be demonstrated, suggesting sustained NO synthesis [20]. However species-specific differences in the kinetics of NO formation exist [21]. With the development of the inducible NOS isoform–specific antibodies and primers for transcriptional and translational analysis, it was demonstrated that iNOS expression is highest in the early phase after acute inflammation. Reverse-transcriptase polymerase chain reaction (RT-PCR) and Northern blotting detect iNOS during the first 5 days in rat models of healing [22, 23].
It is conceivable that the majority of NO synthesis is due to the inflammatory cells present during the early phase of healing, especially macrophages [24]. However, fibroblasts, keratinocytes, and endothelial cells contribute to ongoing NO synthesis, although to a lesser degree [25, 26]. Therefore the overall time course of iNOS activity and NO generation during wound healing has to be viewed as a decreasing curve over time (Fig. 2).

Time course of NO byproducts (citrulline, ornithine, and NO2) in wound fluid. Ornithine: dashed line; NO2: solid line; citrulline, dotted line.
Although the in vitro signals of iNOS induction are well elucidated, little is known of the in vivo signals during wound healing. Of the numerous cytokines and growth factors secreted and released into the wound environment, interleukin-1, tumor necrosis factor-alpha (TNF-α), and INF- γ are the most likely inducers of iNOS. Wound fluid, as a biological reflection of the wound environment, induces NO synthesis in a variety of cells [27].
Although iNOS expression is high during the early phases of wound healing, little is known about the downregulation of iNOS activity at the wound site during the later phases of healing. Presumably iNOS activity can be downregulated by the resolution of the inflammatory response or by cytokine signaling. It is likely that colonized or infected wounds with continued inflammatory responses would continue to generate large amounts of NO, although this has not been studied directly [28]. TGF-β1 is one of the strongest iNOS inhibitors during wound healing [29]. However even during the inflammatory phase of wound healing there is counter-regulation of NO synthesis, as demonstrated by the presence of an unknown factor that reduces iNOS activity, but not by substrate depletion [25].
Mechanism of Action of NO during Wound Healing
Nitric oxide acts via multiple and different mechanisms. Some of its effects are due to its chemical reaction with oxygen leading to formation of reactive radical species [30]. Others are due to its affinity with heme or metal-containing enzymes such as the iron in guanyl-cyclase. At the molecular level, NO has been shown to act as a signaling molecule that operates via guanylate cyclase to activate cGMP. In addition, NO acts as a cytostatic/cytotoxic molecule inhibiting cytochromes and aconitase, as well as ribonucleotide reductase. Nitric oxide also regulates gene expression by reacting with the thiol binding site of the transcription factor NF-kappa beta. By nitrosylating NF-kappa beta, NO prevents binding to the iNOS promoter, suggesting a feedback inhibition mechanism. Nitric oxide has been shown to induce apoptosis via p53 mechanisms in neuroblastoma cells [31]. Yet, at the same time, NO inhibits activation of caspases and thereby prevents apoptosis.
In higher concentrations NO is cytostatic to multiple cell types including endothelial cells, smooth muscle cells, hepatocytes, and fibroblasts [32, 33, 34]. Depending on the cell type, this effect can be cGMP dependent [35] or independent [36]. Target enzymes include the complex I and II of the respiratory chain [37] and ribonucleotide reductase [38], a rate-limiting enzyme in the DNA synthetic pathway. Conversely, NO can stimulate cell proliferation when added in low concentrations [39, 40]. Recent evidence suggests that NO inhibits ornithine-decarboxylase activity, the rate-limiting enzyme for polyamine formation, thus reducing cell proliferation [41].
Nitric oxide regulates gene expression [42, 43] and cellular differentiation [44, 45]. Regulation of gene expression by NO probably occurs indirectly, through amplification of other regulatory mechanisms [46]. For example, although NO is critical for wound collagen deposition, clear-cut enhancement of collagen synthesis or gene expression has not been found (see below). Collagen metabolism and accumulation are tightly regulated through the activity of collagenases and their inhibitors, tissue inhibitors of metalloproteinases (TIMP). Inhibiting the collagenolytic pathway can enhance collagen accumulation. Addition of the NO donor, SNAP, to rat mesangial cells increases gelatinase A activity [47], whereas rat fibroblasts collagenase activity is unaffected by SNAP [35]. Another potential mechanism of posttranslational collagen regulation by NO is regulation of protein kinase C (PKC) activity [48, 49]. By inhibiting PKC activity, NO could potentially downregulate PKC-related collagen synthesis in fibroblasts.
Platelet deposition and degranulation initiates a cytokine explosion of which NO release acts as both stimulant and inhibitor of the inflammation cascade. For instance, NO activates the promoter of the IL-8 gene in a human melanoma cell line. In turn, IL-8 suppresses the expression of iNOS in neutrophils [50]. Transforming growth factor-β1 is another chemoattractant that has been shown to be integrally related to NO; TGF-β suppresses NO production, and at the same time NO can lead to the activation of latent TGF-β1 [51]. Nitric oxide also acts as an immune modulator by attracting monocytes and neutrophils to the wound. Once neutrophils and monocytes are called to action, they become integral players in the cytokine cascade producing TNF-α [52, 53, 54]. Nitric oxide affects the expression of TNF-α directly in human peripheral blood monocytes through a cGMP-independent mechanism [55].
The expression of the monocyte-attracting macrophage chemoattractant protein-1, produced by hyperproliferative keratinocytes at the wound edge, appears to be downregulated by NO at the wound site [56]. This possibility supports a temporal relationship for NO in normal wound healing. Nitric oxide is initially involved in the upregulation of the cytokine cascade, acting as a chemoattractant for immune regulatory cells; thus it is vital to the early stage of wound healing. However, the inflammatory phase of wound healing must move into a proliferative phase for wound healing to progress to completion. Nitric oxide has been shown to be involved in this transition, further supporting a temporal role for NO during normal wound healing.
There is increasing evidence for a functional role of NO in wound healing. Inhibition of iNOS by competitive inhibitors decreases collagen deposition and breaking strength in incisional wounds and impairs the healing of other wound models [57, 58, 59]. When rats are fed an arginine-free diet, wound healing is impaired: conversely, when humans and animals are fed an arginine-enriched diet there is improved healing as measured by collagen deposition and breaking strength [60, 61, 62]. Arginine-supplemented rats have higher levels of NO metabolites in their wound fluid, strongly suggesting that the supplemental arginine is metabolized, at least in part, via NO synthesis [63]. Finally, use of NO donors also improves incisional and excisional wound healing in rats [64, 65, 66]. The data demonstrating that NO has a positive regulatory effect on repair is summarized in Table 1.
The mechanism of action of NO on wound healing remains unclear. However, there are data suggesting that at least some effects of NO on wound healing might be systemically mediated: (1) arginine-free nutrition inhibits LPS-induced NO synthesis in several organs, not only at the wound site [67]; (2) NO mediates inflammation-induced edema formation and inhibits cell infiltration into granulomas [68, 69]; (3) the effect of NO on wound healing is not only iNOS-mediated because eNOS knock-out mice also demonstrate impaired healing [70]; and (4) iNOS inhibitors have a high lethality when present in high concentration [54].
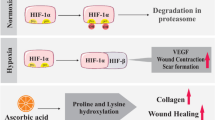
In vitro studies of fibroblasts derived from keloids and hypertrophic scars demonstrate low constitutive NOS expression, thus stimulating higher cell proliferation, which is responsible for the high cellularity characteristic of these disorders. In vivo, keratinocyte proliferation is iNOS-dependent [23] and wound reepithelialisation is also NO-dependent, probably mediated indirectly via vascular endothelial growth factor (VEGF) [71]. Interestingly, induction of iNOS in keratinocytes is paralleled by induction of GTP-cyclohydrolase I, the rate-limiting enzyme for tetrahydrobiopterin formation, which is essential for full iNOS activity [72]. Nitric oxide has been shown to increase angiogenesis in ischemic murine tissues, whereas eNOS inhibitors impair angiogenesis in granulation tissue. Vascular endothelial growth factor, a potent angiogenic growth factor, is closely linked to NO; VEGF increases NO production at the gene expression level [73, 74], and the angiogenic effects of VEGF appears to be dependent on NO [75, 76]. It has also been shown that NOS blockade prevents VEGF production, VEGF-induced endothelial cell proliferation, and VEGF-mediated activation of mitogen-activating protein kinase [77].
Endothelial cell migration, endothelial cell adhesion, and endothelial organization are dependent on NO via VEGF [78, 79, 80, 81], which is made primarily by keratinocytes during wound healing [82]. Nitric oxide increases VEGF expression by keratinocytes, and iNOS inhibitors can block this process both in vitro and in vivo [83]. Monocyte-induced angiogenesis is NO dependent [84], as is substance P–mediated angiogenesis [85]. Feedback mechanisms exist and appear to act by downregulating PKC-induced VEGF expression [86].
Collagen synthesis correlates with NO synthesis during wound healing. Matrix synthesis is impaired by iNOS inhibition, whereas NO administration and iNOS transfection enhance matrix synthesis [55, 61, 87]. Furthermore, wound-derived fibroblasts are characterized by a distinct phenotype where endogenous iNOS expression correlates with increased collagen synthesis [26].
Wound contraction is a major contributor to closure of open wounds. In excisional wounds closure is delayed by iNOS inhibition [68]. In vitro studies showed that NO induces a locomotor phenotype in keratinocytes [88].
Wound healing is characterized by the organized secretion of growth factors. This represents a potential target for regulating wound healing. Little is known about whether NO can directly affect growth factor or cytokine secretion, activation, or time of action. Arginine is known to downregulate TNF-α after trauma thereby affecting outcome [89]. Both TGF-β and EGF directly and indirectly downregulate NO or the NO-mediated effects [90].
Recently we have examined the possibility that a lack of iNOS gene expression alters wound cytokine expression. Using non-isotopic in situ hybridization quantitative analysis, we studied eNOS, basic fibroblast growth factor (bFGF), TGF-β1, TNF-α, VEGF, and IL-4 expression in incisional wounds and compared expression in wild-type and iNOS-KO mice. It was noted that eNOS and bFGF expression nearly doubled on postoperative day 7 in iNOS-KO incisions and remained two- to threefold elevated thereafter. In additon, TGF-β1 expression was increased approximately 50% to 100% in iNOS-KO wounds on postoperative days 5 and 7, and VEGF and IL-4 expression was 25% to 100% higher in wild-type animals than in iNOS-KO animals at all time points. We hypothesize that the overexpression of TGF-β1 and eNOS may represent mechanisms in iNOS-KO mice that compensate for their loss of functional iNOS, resulting in incisional wound healing equivalent to controls. The impaired expression of VEGF and IL-4, on the other hand, may partially explain the delayed excisional wound healing noted in these animals [91].
Large amounts of NO synthesis at the wound can impair wound healing. Sterile inflammation, as induced by turpentine sterile abscess, results in increased NO synthesis with subsequent impaired collagen production. In this setting iNOS inhibition restores collagen synthesis to normal without affecting the overall inflammatory response (Park et al., unpublished data) (Fig. 3).

Nitric oxide and wound healing.
Impaired Wound Models
After the discovery that NO is synthesized during wound healing and that inhibition of its production impairs healing, the next step was to investigate whether there is a correlation between NO and the outcome of healing. Several impaired wound models were used to seek such correlation.
In diabetes at least three studies have demonstrated decreased formation of NO metabolites in the wound environment [92, 93, 94]. It is not clear whether this decrease is due to the lesser inflammatory response characteristic of diabetes or to a net decrease in NO formation by all wound cells. l-arginine as well as NO donors can partially reverse the impaired healing of diabetes and in parallel restore wound NO levels toward more normal values [61, 87]. More work needs to be done to confirm whether these agents might serve as future treatment options.
Malnutrition and radiation-induced injury are other conditions associated with impaired or delayed healing [95]. Steroids, strong inhibitors of healing, alter arginine metabolism by impairing both the iNOS and the arginase pathways [96].
In one study, iNOS knock-out mice demonstrated delayed closure of excisional wounds, which could be reversed by transfection with iNOS-cDNA [97]. Surprisingly however, there was no effect on collagen deposition or breaking strength in incisional wounds in iNOS knock-out mice [98]. Supplemental l-arginine does not enhance wound healing in iNOS knock-out mice, suggesting that metabolism of arginine via iNOS is an essential pathway in the positive effects of arginine on healing [60].
The eNOS knock-out mice also demonstrated delayed healing in excisional wound models [67]. Wound fluid extracted from these wounds, induces a lesser angiogenic response in the cornea angiogenesis models than in controls, underscoring the importance of eNOS for neoangiogensis during wound healing.
The Future
In summary, l-arginine can be metabolized via distinct pathways during wound healing. Experimental animal models demonstrate a positive effect of NO on wound healing. Human studies are lacking, especially therapeutic studies. Influence of the arginase pathways remains to be elucidated.
Résumé.
L’oxyde nitrique est un radical libre de courte durée qui agit au niveau moléculaire, cellulaire et physiologique. Depuis sa découverte il y a plus de 20 ans, son rôle dans la cicatrisation s’est confirmé. Dans cet article on souligne la plupart de ses propriétés dans la cicatrisation des plaies et on fait une revue de la biologie de base de l’oxyde nitrique, son rôle dans la cascade des cytokines, son rôle prometteur dans l’angiogenèse, et son rôle élucidé plus récemment dans l’apoptose.
Resumen.
El óxido nítrico es un radical libre de corta vida que actúa a nivel molecular, celular y fisiológico. Desde su descubrimiento hace casi 20 años ha probado ser un elemento importante en el proceso de la cicatrización de heridas. Esta revisión resalta muchos de los más importantes aspectos del óxido nítrico en la cicatrización de heridas, incluyendo una revisión de la biología básica del óxido nítrico, su participación en la cascada de las citoquinas, la promoción de angiogenesis y el recientemente descubierto papel en la apoptosis.
References
RG Knowles S Moncada (1994) ArticleTitleNitric oxide synthases in mammals Biochem. J. 298 249–258 Occurrence Handle7510950
Y Tsukahara T Morisaki Y Horita et al. (1998) ArticleTitleExpression of inducible nitric oxide synthase in circulating neutrophils of the systemic inflammatory response syndrome and septic patients World J. Surg. 22 771–777 Occurrence Handle10.1007/s002689900468 Occurrence Handle1:STN:280:DyaK1czjvVegsQ%3D%3D Occurrence Handle9673545
E Seifter G Rettura A Barbul et al. (1978) ArticleTitleArginine: an essential amino acid for injured rats Surgery 84 224–230 Occurrence Handle1:CAS:528:DyaE1cXlt1yhs78%3D Occurrence Handle684614
CI Chang JC Liao L Kuo (1998) ArticleTitleArginase modulates nitric oxide production in activated macrophages Am. J. Physiol. 274 H342–H348 Occurrence Handle1:CAS:528:DyaK1cXnsFOhug%3D%3D Occurrence Handle9458885
JL Boucher J Custot S Vadon et al. (1994) ArticleTitleN-omega-hydroxyl-L-arginine, an intermediate in the L-arginine to nitric oxide pathway, is a strong inhibitor of liver and macrophage arginase Biochem. Biophys. Res. Commun. 203 1614–1621 Occurrence Handle10.1006/bbrc.1994.2371 Occurrence Handle1:CAS:528:DyaK2cXmt1Oju78%3D Occurrence Handle7945311
A Hrabak T Bajor A Temesi et al. (1996) ArticleTitleThe inhibitory effect of nitrite, a stable product of nitric oxide (NO) formation, on arginase FEBS Lett. 390 203–206 Occurrence Handle10.1016/0014-5793(96)00659-X Occurrence Handle1:CAS:528:DyaK28XkvVCru7c%3D Occurrence Handle8706860
SS Prahakar GA Zeballos ZM Montoya et al. (1997) ArticleTitleUrea inhibits inducible nitric oxide synthase in macrophage cell line Am. J. Physiol. 273 C1882–C1888 Occurrence Handle9435493
JD Shearer JR Richards CD Mills et al. (1997) ArticleTitleDifferential regulation of macrophage arginine metabolism: a proposed role in wound healing Am. J. Physiol. 272 E181–E190 Occurrence Handle1:CAS:528:DyaK2sXhvVCktbk%3D Occurrence Handle9124321
IM Corraliza G Soler K Eichmann et al. (1995) ArticleTitleArginase induction by suppressors of nitric oxide synthesis (IL-4, IL-10 and PGE-2) in murine bone-marrow-derived macrophages Biochem. Biophys. Res. Commun. 206 667–673 Occurrence Handle10.1006/bbrc.1995.1094 Occurrence Handle1:CAS:528:DyaK2MXjtFejsbc%3D Occurrence Handle7530004
M Modolell IM Corraliza F Link et al. (1995) ArticleTitleReciprocal regulation of the nitric oxide synthase/arginase balance in mouse bone marrow-derived macrophages by TH1 and TH2 cytokines Eur. J. Immunol. 25 1101–1104 Occurrence Handle1:CAS:528:DyaK2MXltFOmtL4%3D Occurrence Handle7537672
LC Green DA Wagner J Glogowski et al. (1982) ArticleTitleAnalysis of nitrate and [15N] nitrate in biological fluids Anal. Biochem. 126 131–138 Occurrence Handle1:CAS:528:DyaL38XlvFGgtLY%3D Occurrence Handle7181105
JL Zweier A Samouilov P Kuppusamy et al. (1999) ArticleTitleNon-enzymatic nitric oxide synthesis in biological systems Biochim. Biophys. Acta 1411 250–262 Occurrence Handle10.1016/S0005-2728(99)00018-3 Occurrence Handle1:CAS:528:DyaK1MXjsF2qtr8%3D Occurrence Handle10320661
L Castillo L Beaumier AM Ajami et al. (1996) ArticleTitleWhole body nitric oxide synthesis in healthy men determined from [15N] arginine-to-[15N] citrulline labeling Proc. Natl. Acad. Sci. U. S. A. 93 11460–11465 Occurrence Handle10.1073/pnas.93.21.11460 Occurrence Handle1:CAS:528:DyaK28Xmtlagsbg%3D Occurrence Handle8876157
L Beaumier L Castillo AM Ajami et al. (1995) ArticleTitleUrea cycle intermediate kinetics and nitrate excretion at normal and “therapeutic” intakes of arginine in humans Am. J. Physiol. 296 E884–E896
JE Albina CD Mills A Barbul et al. (1988) ArticleTitleArginine metabolism in wounds Am. J. Physiol. 254 E459–E467 Occurrence Handle1:CAS:528:DyaL1cXmtV2isLw%3D Occurrence Handle3354662
DJ Smith MJ Dunphy LN Strang et al. (1991) ArticleTitleThe influence of wound healing on urinary nitrate levels in rats Wounds 3 50–58
WK Becker RL Shippee AT McManus et al. (1993) ArticleTitleKinetics of nitrogen oxide production following experimental thermal injury in rats J. Trauma 34 855–862 Occurrence Handle1:CAS:528:DyaK3sXlsFOltr4%3D Occurrence Handle8315681
EA Carter WT Derojas S Tamir et al. (1994) ArticleTitleNitric oxide production is intensely and persistently increased in tissue by thermal injury Biochem. J. 304 201–204 Occurrence Handle1:CAS:528:DyaK2cXmslyjs7s%3D Occurrence Handle7528006
JE Albina CD Mills WL Henry et al. (1990) ArticleTitleTemporal expression of different of l-arginine metabolism in healing wounds J. Immunol. 144 3877–3880 Occurrence Handle1:CAS:528:DyaK3cXktlygsrk%3D Occurrence Handle2332635
MR Schaffer U Tantry RA Wesep Particlevan et al. (1997) ArticleTitleNitric oxide metabolism in wounds J. Surg. Res. 71 25–31 Occurrence Handle10.1006/jsre.1997.5137 Occurrence Handle1:CAS:528:DyaK2sXls1Oqtb8%3D Occurrence Handle9271274
BJ Dull RF Gittes P Goldman (1998) ArticleTitleNitrate production and phagocyte activation: differences among Sprague-Dawley, Wistar-Furth and Lewis rats Carcinogenesis 9 625–627
S Frank M Madlener J Pfeilschifter et al. (1998) ArticleTitleInduction of inducible nitric oxide synthase and its corresponding tetrahydrobiopterin-cofactor-synthesizing enzyme GTP-cyclohydrolase I during cutaneous wound repair J. Invest. Dermatol. 111 1058–1064 Occurrence Handle10.1046/j.1523-1747.1998.00434.x Occurrence Handle1:CAS:528:DyaK1cXnvFyit7o%3D Occurrence Handle9856817
MR Nill TM Oberyszyn MS Ross et al. (1995) ArticleTitleQuantification of inducible nitric oxide gene expression during incisional wound healing Surg. Forum XLVI 753–755
JS Reichner AJ Meszaros CA Louis et al. (1999) ArticleTitleMolecular and metabolic evidence for the restricted expression of inducible nitric oxide synthase in healing wounds Am. J. Pathol. 154 1097–1104 Occurrence Handle1:CAS:528:DyaK1MXislKrs7o%3D Occurrence Handle10233848
MR Schaffer PA Efron FJ Thornton et al. (1997) ArticleTitleNitric oxide, and autocrine regulator of wound fibroblast synthetic function J. Immunol. 158 2375–2381 Occurrence Handle1:STN:280:ByiC1cfktVY%3D Occurrence Handle9036987
SM Paulsen SH Wurster LB Nanney (1998) ArticleTitleExpression of inducible nitric oxide synthase in human burn wounds Wound Repair Regen. 6 142–148 Occurrence Handle10.1046/j.1524-475X.1998.60208.x Occurrence Handle1:STN:280:DyaK1M%2FmsFOhtg%3D%3D Occurrence Handle9776857
MB Witte DT Efron T Kiyama et al. (1998) ArticleTitleWound fluid regulates nitric oxide expression in fibroblasts Surg. Forum XLIX 623–624
E Mahoney J Reichner LR Bostom et al. (2002) ArticleTitleBacterial colonization and the expression of inducible nitric oxidesynthase in murine wounds Am. J. Pathol. 161 2143–2152 Occurrence Handle1:CAS:528:DC%2BD38Xpslemu74%3D Occurrence Handle12466130
Y Vodovotz C Bogdan J Paik et al. (1993) ArticleTitleMechanisms of suppression of macrophage nitric oxide release by transforming growth factor β J. Exp. Med. 178 605–613 Occurrence Handle1:CAS:528:DyaK3sXlsFyjsb0%3D Occurrence Handle7688028
JS Stamler DJ Singel J Loscalzo (1992) ArticleTitleBiochemistry of Nitric Oxide and its Redox-activated forms Science 258 1898–1902 Occurrence Handle1:CAS:528:DyaK3sXlsVChtA%3D%3D Occurrence Handle1281928
X Wang A Zalcenstein M Oren (2003) ArticleTitleNitric oxide promotes p53 nuclear retention and sensitizes neuroblastoma cells to apoptosis by ionizing radiation Cell Death Differ. 10 468–476 Occurrence Handle10.1038/sj.cdd.4401181 Occurrence Handle1:CAS:528:DC%2BD3sXjt1GjsLo%3D Occurrence Handle12719724
J Stadler TR Billiar RD Curran et al. (1991) ArticleTitleEffect of exogenous and endogenous nitric oxide on mitochondrial respiration of rat hepatocytes Am. J. Physiol. 260 C910–C916 Occurrence Handle1:CAS:528:DyaK3MXkt1KmurY%3D Occurrence Handle1903597
KR Thomae DK Nakayama TR Billiar et al. (1995) ArticleTitleThe effect of nitric oxide on fetal pulmonary artery smooth muscle growth J. Surg. Res. 59 337–343 Occurrence Handle10.1006/jsre.1995.1173 Occurrence Handle1:CAS:528:DyaK2MXosVCgu7Y%3D Occurrence Handle7643591
UC Garg A Hassid (1990) ArticleTitleNitric oxide-generating vasodilators inhibit mitogenesis and proliferation of BALB/C 3T3 fibroblasts by cyclic GMP-independent mechanism Biochem. Biophys. Res. Commun. 171 474–479 Occurrence Handle1:CAS:528:DyaK3cXlsV2ls74%3D Occurrence Handle1697465
MJ Patel DM Wypij DA Rose et al. (1995) ArticleTitleSecretion of cyclic GMP by cultured epithelial and fibroblast cell lines in response to nitric oxide J. Pharmacol. Exp. Ther. 273 16–25 Occurrence Handle1:CAS:528:DyaK2MXltVGltro%3D Occurrence Handle7536242
MB Witte FJ Thornton DT Efron et al. (2000) ArticleTitleEnhancement of fibroblast collagen synthesis by nitric oxide Nitric Oxide Biol. Chem. 4 572–582 Occurrence Handle10.1006/niox.2000.0307 Occurrence Handle1:CAS:528:DC%2BD3MXnsVah
J Stadler RD Curran JB Ochoa et al. (1991) ArticleTitleEffect of endogenous nitric oxide on mitochondrial respiration of rat hepatocytes in vitro and in vivo Arch. Surg. 126 186–191 Occurrence Handle1:CAS:528:DyaK3MXkvVKqsb8%3D Occurrence Handle1899557
NS Kwon DJ Stuehr CF Nathan (1991) ArticleTitleInhibition of tumor cell ribonucleotide reductase by macrophage-derived nitric oxide J. Exp. Med. 174 761–767 Occurrence Handle1:CAS:528:DyaK3MXmtVGrurk%3D Occurrence Handle1717630
M Du M Islam L Lin et al. (1997) ArticleTitlePromotion of proliferation murine Balb/C3T3 fibroblasts mediated by nitric oxide at lower concentrations Biochem. Mol. Biol. Int. 41 625–631 Occurrence Handle1:CAS:528:DyaK2sXisValt7k%3D Occurrence Handle9090471
DT Efron SJ Kirk MC Regan et al. (1991) ArticleTitleNitric oxide generation from l-arginine is required for optimal peripheral blood lymphocyte DNA synthesis Surgery 110 327–334 Occurrence Handle1:STN:280:By6A3MzltFI%3D Occurrence Handle1858040
GM Buga LH Wei PM Bauer et al. (1998) ArticleTitleNG-hydroxy-l-arginine and nitric oxide inhibit Caco-2 tumor cell proliferation by distinct mechanisms Am. J. Physiol. 275 R1256–R1264 Occurrence Handle1:CAS:528:DyaK1cXmvV2ru74%3D Occurrence Handle9756558
RW Park IS Kim JS Jo (1996) ArticleTitleBisindolylmaleimide inhibits the PMA-induced down-regulation of collagen synthesis in fibroblasts Biochem. Mol. Biol. Int. 40 101–109 Occurrence Handle1:CAS:528:DyaK28XlvVGmurk%3D Occurrence Handle8886275
RB Pilz M Suhasini S Idriss et al. (1995) ArticleTitleNitric oxide and cGMP analogs activate transcription from AP-1-responsive promoters in mammalian cells FASEB J. 9 552–558 Occurrence Handle1:CAS:528:DyaK2MXlsVOqu7g%3D Occurrence Handle7737465
GR Boss (1989) ArticleTitlecGMP-induced differentiation of the promyelocytic cell line HL-60 Proc. Natl. Acad. Sci. U. S. A. 86 7174–7178 Occurrence Handle1:CAS:528:DyaL1MXlvFaitrY%3D Occurrence Handle2550930
G Magrinat SN Mason PJ Shami et al. (1992) ArticleTitleNitric oxide modulation of human leukemia cell differentiation and gene expression Blood 80 1880–1884 Occurrence Handle1:CAS:528:DyaK3sXntlaisA%3D%3D Occurrence Handle1382708
N Penova G Enikolopov (1993) ArticleTitleAmplification of calcium-induced gene transcription by nitric oxide in neuronal cells Nature 364 450–453 Occurrence Handle10.1038/364450a0 Occurrence Handle8392663
H Trachtman S Futterweit P Garg et al. (1996) ArticleTitleNitric oxide stimulates the activity of a 72kDa neutral matrix metalloproteinase in cultured rat mesangial cells Biochem. Biophys. Res. Commun. 218 704–708 Occurrence Handle10.1006/bbrc.1996.0125 Occurrence Handle1:CAS:528:DyaK28XnslChug%3D%3D Occurrence Handle8579577
E Clementi C Sciorati G Nistico (1995) ArticleTitleGrowth factor-induced Ca2+ responses are differentially modulated by nitric oxide via activation of a cyclic GMP-dependent pathway Mol. Pharmacol. 48 1068–1077 Occurrence Handle1:CAS:528:DyaK28Xislejsw%3D%3D Occurrence Handle8848007
R Gopalakrishna ZH Chen U Gundimeda (1993) ArticleTitleNitric oxide and nitric oxide-generating agents induce a reversible inactivation of protein kinase C activity and phorbol ester binding J. Biol. Chem. 268 27180–27185 Occurrence Handle1:CAS:528:DyaK3sXmsVKltb4%3D Occurrence Handle8262958
TB McCall RMJ Palmer S Moncada et al. (1992) ArticleTitleInterleukin-8 inhibits the induction of nitric oxide synthase in rat peritoneal neutrophils Biochem. Biophys. Res. Commun. 186 680–685 Occurrence Handle1:CAS:528:DyaK38Xlt12lurw%3D Occurrence Handle1379804
Y Vodovotz H Chesler SJ Chong et al. (1999) ArticleTitleRegulation of transforming growth factor-β1 by nitric oxide Cancer Res. 59 2142–2149 Occurrence Handle1:CAS:528:DyaK1MXjtVWjsbs%3D Occurrence Handle10232601
SM Wahl H Wong McCartney-Francis (1989) ArticleTitleRole of growth factors in inflammation and repair J. Cell. Biochem. 40 193–199 Occurrence Handle1:CAS:528:DyaL1MXkslWjtr4%3D Occurrence Handle2670976
JC Ansel CA Armstrong I Song et al. (1997) ArticleTitleInteractions of the skin and nervous system J Investig Dermatol Symp Proc. 2 23–26 Occurrence Handle1:STN:280:DyaK1c7jt12kuw%3D%3D Occurrence Handle9487011
J Imanishi K Kamiyama I Iguchi et al. (2000) ArticleTitleGrowth factors: importance in wound healing and maintenance of transparency of the cornea Prog Retina Eye Res. 19 113–129 Occurrence Handle10.1016/S1350-9462(99)00007-5 Occurrence Handle1:CAS:528:DC%2BD3cXlslWnuw%3D%3D
HM Lander P Sehajpal DM Levine et al. (1993) ArticleTitleActivation of human peripheral blood mononuclear cells by nitric oxide-generating compounds J. Immunol. 150 1509–1516 Occurrence Handle1:CAS:528:DyaK3sXhvV2qsrc%3D Occurrence Handle8432991
C Wetzer H Kampfer J Pfeilschifter et al. (2000) ArticleTitleKeratinocyte-derived chemotactic cytokines: expressional modulation by nitric oxide in vitro and during cutaneous wound repair in vivo Biochem. Biophys. Res. Commun. 274 689–696 Occurrence Handle10.1006/bbrc.2000.3170 Occurrence Handle10924337
MR Shaffer U Tantry FJ Thornton et al. (1999) ArticleTitleInhibition of nitric oxide synthesis in wounds: pharmacology and effect on accumulation of collagen in wounds in mice Eur. J. Surg. 165 262–267 Occurrence Handle10.1080/110241599750007153 Occurrence Handle10231662
M Schaffer U Tantry SS Gross et al. (1996) ArticleTitleNitric oxide regulates wound healing J. Surg. Res. 63 237–240 Occurrence Handle10.1006/jsre.1996.0254 Occurrence Handle1:CAS:528:DyaK28XksVOmsrc%3D Occurrence Handle8661204
GA Murrell C Szabo JA Hannafin et al. (1997) ArticleTitleModulation of tendon healing by nitric oxide Inflamm. Res. 46 19–27 Occurrence Handle10.1007/s000110050027 Occurrence Handle1:CAS:528:DyaK2sXhsVCrur8%3D Occurrence Handle9117513
JP Bulgrin M Shabani DJ Smith (1993) ArticleTitleArginine-free diet suppresses nitric oxide production in wounds J Nutr Biochem. 4 588–593 Occurrence Handle10.1016/0955-2863(93)90027-T Occurrence Handle1:CAS:528:DyaK2cXntl2k
A Barbul RS Fishel S Shimazu et al. (1985) ArticleTitleIntravenous hyperalimentation with high arginine levels improves wound healing and immune function J. Surg. Res. 38 328–334 Occurrence Handle1:CAS:528:DyaL2MXksFejtLs%3D Occurrence Handle3923266
A Barbul SA Lazarou DT Efron et al. (1990) ArticleTitleArginine enhances wound healing and lymphocyte immune responses in humans Surgery 108 331–336 Occurrence Handle1:STN:280:By%2BA2c7psFY%3D Occurrence Handle2382229
HP Shi DT Efron D Most et al. (2000) ArticleTitleSupplementary dietary arginine enhances wound healing in normal but not inducible nitric oxide synthase knock-out mice Surgery 128 374–378 Occurrence Handle10.1067/msy.2000.107372 Occurrence Handle1:STN:280:DC%2BD3cvhsFOnug%3D%3D Occurrence Handle10923019
MB Witte FJ Thornton T Kiyama et al. (1997) ArticleTitleNitric oxide enhances wound collagen deposition in diabetic rats Surg. Forum XLVIII 665–667
M Shabani SK Pulfer JP Bulgrin et al. (1996) ArticleTitleEnhancement of wound repair with a topically applied nitric oxide-releasing polymer Wound Rep. Reg. 4 353–362 Occurrence Handle10.1046/j.1524-475X.1996.40312.x
JA Bauer W Rao DJ Smith (1998) ArticleTitleEvaluation of linear polythyleneimine/nitric oxide adduct on wound repair: therapy versus toxicity Wound Rep. Reg. 6 569–577 Occurrence Handle10.1046/j.1524-475X.1998.60609.x Occurrence Handle1:STN:280:DyaK1M7htlShtQ%3D%3D
G Wu NE Flynn SP Flynn et al. (1999) ArticleTitleDietary protein or arginine deficiency impairs constitutive and inducible nitric oxide synthesis by young rats J. Nutr. 129 1347–1354 Occurrence Handle1:CAS:528:DyaK1MXkt12ntb8%3D Occurrence Handle10395597
T Iuvone R Carnuccion M DiRosa (1994) ArticleTitleModulation of granuloma formation by endogenous nitric oxide Eur. J. Pharmacol. 265 89–92 Occurrence Handle10.1016/0014-2999(94)90227-5 Occurrence Handle1:CAS:528:DyaK2MXitFOms7k%3D Occurrence Handle7883033
T Iuvone ON Van F D’Acquisto et al. (1997) ArticleTitleDifferential effect of L-NAME and S-methyl-isothiourea on leukocyte emigration in carrageenin-soaked sponge implants in rat Br. J. Pharmacol. 121 1637–1644 Occurrence Handle1:CAS:528:DyaK2sXlslaqt7g%3D Occurrence Handle9283697
PC Lee AN Salyapongse GA Bragdon et al. (1999) ArticleTitleImpaired wound healing and angiogenesis in eNOS-deficient mice Am. J. Physiol. 277 H1600–H1608 Occurrence Handle1:CAS:528:DyaK1MXntF2hu7g%3D Occurrence Handle10516200
B Stallmeyer H Kampfer N Kolb et al. (1998) ArticleTitleThe function of nitric oxide in wound repair: inhibition of inducible nitric oxide-synthase severely impairs wound reepithelialization J. Invest. Dermatol. 113 1090–1098 Occurrence Handle10.1046/j.1523-1747.1999.00784.x
S Frank N Kolb ER Werner et al. (1998) ArticleTitleCoordinated induction of inducible nitric oxide synthase and GTP-cyclohydrolase I is dependent on inflammatory cytokines and interferon-gamma in HaCaT keratinocytes: implications for the model of cutaneous wound repair J. Invest. Dermatol. 111 1065–1071 Occurrence Handle10.1046/j.1523-1747.1998.00433.x Occurrence Handle1:CAS:528:DyaK1cXnvFyit7g%3D Occurrence Handle9856818
JD Hood CJ Meininger M Ziche et al. (1998) ArticleTitleVEGF upregulates ecNOS message, protein, and NO production in human endothelial cells Am. J. Physiol. 274 H1054–H1058 Occurrence Handle1:CAS:528:DyaK1cXitVSjs7c%3D Occurrence Handle9530221
ZR Vander T Murohara Z Luo et al. (1997) ArticleTitleVascular endothelial growth factor/vascular permeability factor augments nitric oxide release from quiescent rabbit and human vascular endothelium Circulation 95 1030–1037 Occurrence Handle9054767
M Ziche L Morbidelli R Chouhuri et al. (1997) ArticleTitleNitric oxide synthase lies downstream from vascular endothelial growth factor-induced but not basic fibroblastic growth factor-induced angiogenesis J. Clin. Invest. 99 2625–2634 Occurrence Handle1:CAS:528:DyaK2sXjs1Knurs%3D Occurrence Handle9169492
A Parenti L Morbidelli XL Cui et al. (1998) ArticleTitleNitric oxide is an upstream signal of vascular endothelial growth factor-induced extracellular signal-related kinase 1/2 activation in post-capillary endothelium J. Biol. Chem. 273 4220–4226 Occurrence Handle10.1074/jbc.273.7.4220 Occurrence Handle1:CAS:528:DyaK1cXht1ahsbk%3D Occurrence Handle9461619
L Morbidelli CH Chang JG Douglas et al. (1996) ArticleTitleNitric oxide mediates mitogenic effect of VEGF on coronary venular endothelium Am. J. Physiol. 270 H411–H415 Occurrence Handle1:CAS:528:DyaK28XhtFantb8%3D Occurrence Handle8769777
A Papapetropoulos G Garcia-Cardena JA Madri et al. (1997) ArticleTitleNitric oxide production contributes to the angiogenic properties of vascular endothelial growth factor in human endothelial cells J. Clin. Invest. 100 3131–3139 Occurrence Handle1:CAS:528:DyaK2sXotVyrs70%3D Occurrence Handle9399960
Y Shizukuda S Tang JA Yokota et al. (1999) ArticleTitleVascular endothelial growth factor-induced endothelial cell migration and proliferation depend on a nitric oxide-mediated decrease in protein kinase C delta activity Circ. Res. 85 247–256 Occurrence Handle1:CAS:528:DyaK1MXltFGgsL8%3D Occurrence Handle10436167
E Noiri Y Hu CR Bahou et al. (1997) ArticleTitlePermissive role of nitric oxide in endothelin-induced migration of endothelial cells J. Biol. Chem. 272 1747–1752 Occurrence Handle10.1074/jbc.272.3.1747 Occurrence Handle1:CAS:528:DyaK2sXls1Ggsw%3D%3D Occurrence Handle8999856
E Noiri E Lee J Testa et al. (1998) ArticleTitlePodokinesis in endothelial cell migration: role of nitric oxide Am. J. Physiol. 274 C236–C244 Occurrence Handle1:CAS:528:DyaK1cXotF2msA%3D%3D Occurrence Handle9458733
LF Brown KT Yeo B Berse et al. (1992) ArticleTitleExpression of vascular permeability factor (vascular endothelial growth factor) by epidermal keratinocytes during wound healing J. Exp. Med. 176 1375–1379 Occurrence Handle1:CAS:528:DyaK38XlvVGlsro%3D Occurrence Handle1402682
S Frank B Stallmeyer H Kamper et al. (1999) ArticleTitleNitric oxide triggers enhanced induction of vascular endothelial growth factor expression in cultured keratinocytes (HaCaT) and during cutaneous wound repair FASEB J. 13 2002–2014 Occurrence Handle1:CAS:528:DyaK1MXnt1Gntbc%3D Occurrence Handle10544183
SJ Leibovich PJ Polverini TW Fong et al. (1994) ArticleTitleProduction of angiogenic activity by human monocytes requires an L-arginine/nitric oxide-synthase-dependent effector mechanism Proc. Natl. Acad. Sci. U. S. A. 91 4190–4194 Occurrence Handle1:CAS:528:DyaK2cXktVKjtrk%3D Occurrence Handle7514298
M Ziche L Morbidelli E Masini et al. (1994) ArticleTitleNitric oxide mediates angiogenesis in vivo and endothelial cell growth factor and migration in vitro promoted by substance P J. Clin. Invest. 94 2036–2044 Occurrence Handle1:CAS:528:DyaK2cXmvFentb4%3D Occurrence Handle7525653
Y Tsurumi T Murohara K Krasinski et al. (1997) ArticleTitleReciprocal relation between VEGF and NO in the regulation of endothelial integrity Nat. Med. 3 879–886 Occurrence Handle1:CAS:528:DyaK2sXltVKqurg%3D Occurrence Handle9256279
FJ Thornton MR Schaffer MB Witte et al. (1998) ArticleTitleEnhanced collagen accumulation follows direct transfection of the inducible nitric oxide synthase gene in cutaneous wounds Biochem. Biophys. Res. Commun. 246 654–659 Occurrence Handle10.1006/bbrc.1998.8681 Occurrence Handle1:CAS:528:DyaK1cXjsFyisro%3D Occurrence Handle9618268
E Noiri T Peresleni N Srivastava et al. (1996) ArticleTitleNitric oxide is necessary for a switch from stationary to locomoting phenotype in epithelial cells Am. J. Physiol. 270 C794–C802 Occurrence Handle1:CAS:528:DyaK28XitVajsbg%3D Occurrence Handle8638659
XL Cui M Iwasa Y Iwasa et al. (2000) ArticleTitleArginine-supplemented diet decreases expression of inflammatory cytokines and improves survival in burned rats J. Parent. Ent. Nutr. 24 89–96 Occurrence Handle1:CAS:528:DC%2BD3cXlvFGmt7o%3D
DE Heck DL Laskin CR Gardner et al. (1992) ArticleTitleEpidermal growth factor suppresses nitric oxide and hydrogen peroxide production by keratinocytes J. Biol. Chem. 267 21277–21280 Occurrence Handle1:CAS:528:DyaK38Xls1Ckt78%3D Occurrence Handle1383221
D Most DT Efron HP Shi et al. (2002) ArticleTitleCharacterization of incisional wound healing in inducible nitric oxide synthase knockout mice Surgery 132 866–876 Occurrence Handle10.1067/msy.2002.127422 Occurrence Handle12464872
JP Bulgrin M Shabani D Chakravarthy et al. (1995) ArticleTitleNitric oxide synthesis is suppressed in steroid-impaired and diabetic wound healing Wounds 7 48–57
MR Schaffer U Tantry PA Efron et al. (1997) ArticleTitleDiabetes-impaired healing and reduced wound nitric oxide synthesis: a possible pathophysiologic correlation Surgery 121 513–519 Occurrence Handle9142149
MB Witte FJ Thornton U Tantry et al. (1999) ArticleTitlel-Arginine enhances diabetic wound healing Wound Rep. Reg. 7 A326
MR Schaffer U Tantry GM Ahrendt et al. (1997) ArticleTitleAcute protein-calorie malnutrition impairs wound healing: a possible role of decreased wound nitric oxide synthesis J. Am. Coll. Surg. 184 37–43 Occurrence Handle1:STN:280:ByiC2czivVM%3D Occurrence Handle8989298
AE Ulland JD Shearer C Coulter et al. (1997) ArticleTitleAltered wound arginine metabolism by corticosterone and retinoic acid J. Surg. Res. 70 84–88 Occurrence Handle10.1006/jsre.1997.5099 Occurrence Handle1:CAS:528:DyaK2sXlt1Cqs78%3D Occurrence Handle9228933
K Yamasaki HD Edington C McClosky et al. (1998) ArticleTitleReversal of impaired wound repair in iNOS-deficient mice by topical adenoviral-mediated iNOS gene transfer J. Clin. Invest. 101 967–971 Occurrence Handle1:CAS:528:DyaK1cXhs1yqs7o%3D Occurrence Handle9486966
DT Efron MB Witte U Tantry et al. (1999) ArticleTitleIncisional wound healing in two different strains of inducible nitric oxide synthase knock-out mice Wound Rep. Reg. 7 A295
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Rizk, M., Witte, M. & Barbul, A. Nitric Oxide and Wound Healing. World J. Surg. 28, 301–306 (2004). https://doi.org/10.1007/s00268-003-7396-7
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00268-003-7396-7