
Abstract
Background
The septal extension graft is one of the most commonly used grafts in Asian tip plasty techniques. However, the septal extension graft usually induces a hard and immobile nasal tip. The purpose of this study was to evaluate the esthetic outcomes of the modified septal extension graft with M-shaped auricular cartilage by three-dimensional anthropometric analysis.
Methods
A total of 36 patients received augmentation rhinoplasty with M-shaped auricular cartilage as septal extension graft combined with silicone implant. Thirteen measurement items were evaluated using three-dimensional anthropometric techniques, and the preoperative and postoperative results were compared.
Results
The majority of patients (91.7%) were satisfied with the postoperative nasal shape. No infection, gross absorption, graft exposure, implant exposure, or implant migration was observed. Compared with the preoperative value, the nasal length, nasal height, nasal depth, nasion height, columella width, nasolabial angle, nasofrontal angle, and nasal depth-nasal width index significantly increased. The nasal width, nasal tip width, and nasal index significantly decreased.
Conclusion
We performed tip plasty with the M-shaped auricular cartilage as modified septal extension graft, achieving a soft and mobile tip with satisfying tip projection in most patients.
Level of Evidence IV
This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rhinoplasty is becoming increasingly popular among Asians because most Asian noses suffer from a bulbous tip, low radix, low dorsum, short columella, and thick skin envelope [1]. Dorsal augmentation is a relatively well-developed procedure that involves synthetic implants to make a higher dorsum. With a multitude of procedures reported, nasal tip refinement is more complex compared to dorsal augmentation [2, 3]. Because of its availability, biocompatibility and anti-infectivity, autologous cartilage has been widely utilized for tip plasty instead of synthetic implants [4].
Septal extension graft (SEG) is a technique to control nasal tip projection, shape, rotation, and provide nasal lengthening, which is widely used in Asian rhinoplasty. For the patients with thicker skin and relatively weak lower lateral cartilage, SEG has been founded to maintain a greater projection of the nasal tip than columellar strut [5]. However, fixing the SEG to septum remains challenges, for insecure fixation between SEG and septum may result in tip drooping or bending of the graft, while rigid fixation may lead to an unnatural appearance. Various modified techniques, such as suture techniques, the junction types of septum and graft, and the designs of SEG, have been introduced to overcome these shortcomings [6].
Septal cartilage is most commonly used for the SEG due to its strong support, but the majority of Asians possess insufficient septal cartilage to meet the requirements [7]. Besides, it should be applied selectively on account of the excessive thickness and strength of the costal cartilage, as well as chest scars. Some studies have suggested that auricular cartilage is more suitable as a nasal tip graft, due to its adequate tissue and elasticity being close to that of alar cartilage [8]. Therefore, we designed a modified SEG with M-shaped auricular cartilage to overcome the shortcomings in Asian noses, which allowed for a closer reconstruction of the physiological nasal tip structure. Thus, the purpose of this study was to evaluate the esthetic outcomes of the modified SEG with M-shaped auricular cartilage by three-dimensional anthropometric analysis.
Methods
Patient Cohort
A total of 36 female patients with saddle nose deformity who underwent rhinoplasty with M-shaped auricular cartilage as modified SEG combined with silicone implant from February 2015 to June 2019 at Tongji Hospital, were included in this study. All patients underwent primary rhinoplasty for esthetic reasons and were evaluated using three-dimensional anthropometric analysis preoperatively and postoperatively. Cleft, syndromic and trauma-related patients were excluded. The age of patients ranged from 21 to 32 years, with an average of 26.2 years. All procedures performed in studies followed the 1964 Helsinki declaration.
Surgical Technique
Auricular cartilage was harvested through a retroauricular incision and was removed without damaging the anterior skin. An L-shaped auricular cartilage of approximately 2.5 cm in length was obtained (Fig. 1a). Two auricular cartilage strips, approximately 8 mm wide, were produced from harvested auricular cartilage. The two auricular cartilage strips were sutured back-to-back to form an M-shaped graft (Fig. 1b)

a An L-shaped auricular cartilage was harvested. b Two auricular cartilage strips were sutured back-to-back, forming an M-shaped graft. c Middle part of the M-shaped graft was fixed to the caudal septum. d The medial crura of lower lateral cartilages were fixed to the graft
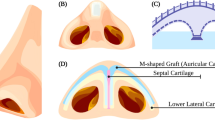
Through a transcolumellar inverted V-shaped incision, the skin envelope was elevated to expose lower lateral cartilages, septum, and upper lateral cartilages. As needed, correction of septal deviation or percutaneous, medial, and lateral osteotomies were performed. The middle part of the M-shaped graft was located to the caudal septum and fixed with sutures (Figs. 1c, 2c). The lower lateral cartilages were advanced as needed, and medial crura were fixed to the graft bilaterally (Figs. 1d, 2c). Then, the two wings of the graft were fixed to the domal segments of the lower lateral cartilage for tip projection and rotation, forming double arches (Fig. 2). The remaining cartilage could be used as onlay graft or alar base filler as need. Silicone implant was carved into suitable size and implanted into the dorsal subfascial space. Incisions were sutured finely, followed by packing of the nasal cavity and maintaining the nasal shape with plaster.

The two wings of M-shaped graft were fixed to the domal segments of the lower lateral cartilage. a Lateral view, b anteroposterior view, c, d diagram of the surgical procedure
Three-Dimensional Anthropometric Analysis
A handheld three-dimensional scanner (EinScan-Pro + , SHINING 3D, China) was used to perform three-dimensional imaging of the face. The model of the face was reconstructed by software Geomagic Studio 2013 (Geomagic Inc., USA). The nasal parameters were measured using 3-matic Research 9.0 software (Materialise Inc., USA). Anthropometric landmarks were defined according to the previous reports of Farkas [9]. Eight facial landmarks were identified on each facial image by the software (Fig. 3a). The landmarks were as follows: nasion point (n), nasal tip point (prn), subnasal point (sn), upper lip point (ls), bilateral outmost points of the nasal ala (al) and bilateral inner canthus points (en).

Three-dimensional anthropometric analysis of nose. a Nasal landmarks in frontal view. b Measurement of nasal angles in lateral view: α = nasofrontal angle, β = nasal tip angle, γ = nasolabial angle
Seven linear, four angular standard anthropometric measurements and two nasal indexes were obtained. Linear measurements were as follows: nasal length (distance between the nasion point and the nasal tip point), nasal height (distance between the nasion point and the subnasal point), nasal width (distance between bilateral outmost points of the nasal ala), nasal depth (distance between the subnasal point and the nasal tip point), nasion height (vertical distance between nasion point and the inner canthus plane), nasal tip width (distance between bilateral tip-defining points) and columella width (distance between bilateral midpoints of columella). Angular measurements were as follows (Fig. 3b): nasolabial angle (angle between the columella line and the line connecting the subnasal point and the upper lip point), nasofrontal angle (angle between the nasal dorsum line and the oblique plane from the forehead to the nasion), nasofacial angle (angle between nasion-to-pogonion line to with nasion-to-tip line), and nasal tip angle (angle between the nasal dorsum line and columella line). Nasal indexes, including nasal index (ratio of nasal width to nasal height) and nasal depth-nasal width index (ratio of nasal depth to nasal width) were calculated.
Assessment of Complications and Patient Satisfaction
Postoperative complications, including infection, gross absorption, graft exposure, implant exposure, or implant migration, were evaluated and recorded. Patient satisfaction was assessed by verbally questioning how patients rated their postoperative nasal appearance as satisfactory or unsatisfactory.
Statistical Analysis
The data were analyzed using Prism 8.0 (GraphPad Software, San Diego, CA) software. All data were expressed as mean ± SD. The paired student t-test was used to compare the difference between preoperative and postoperative nasal parameters. P < 0.05 was considered statistically significant.
Results
Characteristics of Patients
A total of 36 patients received augmentation rhinoplasty with M-shaped auricular cartilage as SEG combined with silicone implant. All patients underwent primary rhinoplasty. The mean follow-up was 16.3 months, with a range from 13 to 25 months. Thirty-three patients (91.7%) were pleased with the postoperative nasal contour and tip projection (Figs. 4, 5), while the other three patients (8.3%) felt little change in nasal appearance. No further complications were found in these patients, such as infection, gross absorption, graft exposure, implant exposure, or implant migration.

A 25-year-old Asian woman who underwent rhinoplasty M-shaped auricular cartilage and dorsal augmentation. Preoperative a and postoperative b facial profiles are shown

A 27-year-old Asian woman who underwent rhinoplasty M-shaped auricular cartilage and dorsal augmentation. Preoperative a and postoperative b facial profiles are shown
Comparison of Preoperative and Postoperative Nasal Measurements
The results of the three-dimensional anthropometric analysis are detailed in Table 1. The mean nasal lengths were 40.77 ± 4.22 mm preoperatively and 46.65 ± 5.57 mm postoperatively (P < 0.0001). The mean difference between preoperative and postoperative nasal lengths was 5.88 ± 4.65 mm. The average nasal depths were 16.31 ± 2.86 mm preoperatively and 18.22 ± 2.95 mm postoperatively (p = 0.0009), and the mean difference between preoperative and postoperative nasal depths was 1.91 ± 2.04 mm. The mean columella widths were 7.33 ± 1.02 mm preoperatively and 7.77 ± 1.01 mm postoperatively (P < 0.0001). The mean difference between preoperative and postoperative columella widths was 0.44 ± 0.52 mm. Compared with the preoperative values, the postoperative nasal heights and nasion heights increased significantly, by 4.73 ± 4.04 mm (p < 0.0001) and 2.48 ± 2.34 (p < 0.0001), respectively. Likewise, the nasal widths and nasal tip widths decreased significantly, by − 1.26 ± 2.12 mm (p = 0.0011) and − 0.92 ± 1.28 (p = 0.0092), respectively. The mean nasolabial angles were 97.33° ± 11.70° preoperatively and 100.00° ± 10.82° postoperatively (P = 0.0078). The mean difference between preoperative and postoperative nasolabial angles was 2.67° ± 1.63°. The mean nasofrontal angles were 140.4° ± 6.92° preoperatively and 145.8° ± 7.93° postoperatively (P = 0.0078). The mean difference between preoperative and postoperative nasofrontal angles was 5.41° ± 6.48°. However, the preoperative and postoperative nasofacial angles (p = 0.8016) and nasal tip angles (p = 0.3542) were not different. Compared with the preoperative value, the nasal index decreased (p < 0.0001) and nasal depth-nasal width index increased (p < 0.0001) significantly.
Discussion
Located in the center of the face, the nose plays a decisive role in the appearance. However, due to the thicker skin envelope, denser fibromuscular layer, and smaller lower lateral cartilages than those of Caucasians, the noses of Asians are characterized by a round or bulbous tip, less tip projection, lower dorsum, and wider nasal base [10, 11]. L-shaped silicone implants were once widely used in dorsal augmentation and tip plasty, but long-term follow-up revealed a high incidence of postoperative complications, such as infection and implant protrusion [12]. The prevailing concept is dorsal rhinoplasty using silicone implants and tip rhinoplasty using autologous cartilage.
Costal cartilage, auricular cartilage, and septal cartilage are all widely used in tip plasty. A large amount of tissue and the strong support of costal cartilage are advantageous for nasal tip shaping, but the disadvantages include chest damage and incisional scarring. With less septal cartilage available in Asians, it is difficult to complete tip plasty using septal cartilage alone. The mechanical properties of both the costal cartilage and the septal cartilage are stiff and straight, unlike those of the lower lateral cartilages [6, 13]. The matrix of the auricular cartilage contains a large amount of elastic fiber, so the auricular cartilage is soft and flexible, making it possible to withstand appropriate force without fracturing. The surface of the auricular cartilage is smooth and curves into a natural arch, resembling a physiological nasal tip. Besides, the advantages of hidden incisions, less injury, and sufficient amount of bilateral auricular cartilage tissue make it an ideal choice for rhinoplasty.
Reinforcement of the nasal tip is required in most Asian noses. Although the suture technique of lower lateral cartilages is a way to enhance nasal tip support, it is difficult to achieve the ideal nasal tip shape and projection simply by sutures due to the thick soft tissue envelope and underdeveloped medial crura in Asian noses. Structural supporting grafts such as the columellar strut graft or septal extension graft are essential techniques combined with the suture technique. The columellar strut graft can reinforce the medial crura of lower lateral cartilages to obtain sufficient nasal tip projection [14]. However, cephalic rotation of the dome caused by columellar strut graft would lead to nasal shortening and nostril exposure. The septal extension graft is an effective method to control nasal lengthening, tip projection and rotation, allowing to compensate for the shortcomings of the columellar strut graft [6, 15]. As the physiological nasal tip should be mobile, and the strength of auricular cartilage is similar to that of the low lateral cartilage, we designed a modified septal extension graft by using a back-to-back, M-shaped auricular cartilage graft. This technique is easy and effective to increase nasal tip protrusion and lengthen the nose.
The long-term follow-up results of the patients enrolled in the present study demonstrated that the M-shaped auricular graft as SEG could result in stable refinement of the nasal tip, with an average increase in nasal depth of 1.91 mm and an average decrease in nasal tip width of 0.92 mm. Besides, the nasal parameters such as nasal height, nasal length, nasofacial angle, and nasal tip angle increased postoperatively. However, the postoperative columella width increased slightly by 0.44 mm. The M-shaped SEG has refined the nasal profile, as reflected in the nasal index and nasal depth-nasal width index. Thus, reliable control of the nasal tip, such as projection, rotation, and nasolabial angle, is available with this efficient technique. The direction of the M-shaped SEG is adjustable, if the graft is positioned more perpendicular to the nasal dorsum, the mechanical advantage in tip projection is greater. By adjusting the M-shaped SEG to control the anterior end of the graft, it is feasible to simultaneously increase the nasal length and tip projection appropriately, which is suitable for short noses with low nasal tips in Asians.
There are several advantages to using this M-shaped septal extension graft. First, this auricular cartilage graft resembles the physiological nasal tip structure, which enables the elastic tip to withstand moderate external forces after surgery, even if rigid fixation between SEG and septum. Second, the nasal length and tip projection can be modified by adjusting the direction of the M-shaped SEG to suit the individual. Third, two wings of the strut are fixed to the domal segments of the lower lateral cartilage to form double arches, which further improves the tip projection. Due to the elasticity of the arches, the risk of the strut protruding is reduced. Fourth, the integrity of the nasal septal cartilage is not damaged, and the supporting strength of the nose is protected. Fifth, preserving the intact cartilage membrane and matrix, the auricular cartilage graft forms a strong unit that provides exact support for adequate tip projection and preventing the cephalic rotation of the dome. Finally, the procedure is simple enough to correct most mild to moderate short noses and bulbous tips.
Some limitations existed in this study. Firstly, due to the relatively small number of cases and the short follow-up period in this study, more patients and long-term follow-up are needed to verify the effectiveness and reliability of the graft. Furthermore, auricular cartilage provides less strength than costal cartilage which may not be sufficient to correct severe short and bulbous noses
Conclusions
M-shaped auricular cartilage as modified septal extension graft is relatively easy to master and simultaneously refines the projection and width of nasal tip and increases the nasal length in most Asian patients. The new technique not only allows for stable nasal tip support, but also makes the tip soft and mobile due to the elasticity of the auricular cartilage.
Reference
Kim EK, Daniel RK (2012) Operative techniques in asianrhinoplasty. Aesthet Surg J 32:1018–1030. https://doi.org/10.1177/1090820X12462716
Sands NB, Adamson PA (2015) Nasal tip deprojection with crural cartilage overlap. Facial Plast Surg Clin N Am. https://doi.org/10.1016/j.fsc.2014.09.007
Lee MR, Geissler P, Cochran S et al (2014) Decreasing nasal tip projection in rhinoplasty. Plast Reconstr Surg. https://doi.org/10.1097/PRS.0000000000000269
Araco A, Gravante G, Araco F et al (2006) Autologous cartilage graft rhinoplasties. Aesthetic Plast Surg. https://doi.org/10.1007/s00266-005-0184-z
Byrd HS, Andochick S, Copit S, Walton KG (1997) Septal extension grafts: a method of controlling tip projection shape. Plast Reconstr Surg. https://doi.org/10.1097/00006534-199709001-00026
Kim M, Choi J, Kim M et al (2014) An Introduction to the septal extension graft. Arch Plast Surg. https://doi.org/10.5999/aps.2014.41.1.29
Paik MH, Chu LS (2014) Correction of short nose deformity using a septal extension graft combined with a derotation graft. Arch Plast Surg. https://doi.org/10.5999/aps.2014.41.1.12
Suh YC, Jeong WS, Choi JW (2018) Septum-based nasal tip plasty: a comparative study between septal extension graft and double-layered conchal cartilage extension graft. Plast Reconstr Surg 141:49–56. https://doi.org/10.1097/PRS.0000000000003920
Farkas LG, Kolar JC, Munro IR (1986) Geography of the nose: a morphometric study. Aesthetic Plast Surg. https://doi.org/10.1007/BF01575292
Wu WT (1992) The Oriental nose: an anatomical basis for surgery. Ann Acad Med Singap 21:176–189
Zingaro EA, Falces E (1987) Aesthetic anatomy of the non-caucasian nose. Clin Plast Surg 14:749–765
Tham C, Lai YL, Weng CJ, Chen YR (2005) Silicone augmentation rhinoplasty in an oriental population. Ann Plast Surg. https://doi.org/10.1097/01.sap.0000141947.00927.49
Lee MJ, Song HM (2015) Asian rhinoplasty with rib cartilage. Semin Plast Surg. https://doi.org/10.1055/s-0035-1564815
Kim HI, Lee WJ, Roh TS, Suh MK (2019) A novel technique of Asian tip plasty: rein-shaped columellar strut graft. Aesthetic Plast Surg 43:1301–1309. https://doi.org/10.1007/s00266-018-1185-z
Hwang NH, Dhong ES (2018) Septal extension graft in asianrhinoplasty. Facial Plast Surg Clin North Am 26:331–341. https://doi.org/10.1016/j.fsc.2018.03.007
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest to disclose.
Human or Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
For this type of study informed consent is not required.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Wang, D., Hou, K. & Zeng, N. M-Shaped Auricular Cartilage as Modified Septal Extension Graft: A Study by Three-Dimensional Anthropometric Analysis in Asian Rhinoplasty. Aesth Plast Surg 45, 2287–2294 (2021). https://doi.org/10.1007/s00266-021-02217-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00266-021-02217-3