
Abstract
Purpose
Osteoarthritis (OA) is characterized by articular cartilage degeneration and subchondral bone sclerosis. OA can benefit of non-surgical treatments with collagenase-isolated stromal vascular fraction (SVF) or cultured-expanded mesenchymal stem cells (ASCs). To avoid high manipulation of the lipoaspirate needed to obtain ASCs and SVF, we investigated whether articular infusions of autologous concentrated adipose tissue are an effective treatment for knee OA patients.
Methods
The knee of 20 OA patients was intra-articularly injected with autologous concentrated adipose tissue, obtained after centrifugation of lipoaspirate. Patients’ articular functionality and pain were evaluated by VAS and WOMAC scores at three, six and 18 months from infusion. The osteogenic and chondrogenic ability of ASCs contained in the injected adipose tissue was studied in in vitro primary osteoblast and chondrocyte cell cultures, also plated on 3D-bone scaffold. Knee articular biopsies of patients previously treated with adipose tissue were analyzed. Immunohistochemistry (IHC) and scanning electron microscopy (SEM) were performed to detect cell differentiation and tissue regeneration.
Results
The treatment resulted safe, and all patients reported an improvement in terms of pain reduction and increase of function. According to the osteogenic or chondrogenic stimulation, ASCs expressed alkaline phosphatase or aggrecan, respectively. The presence of a layer of newly formed tissue was visualized by IHC staining and SEM. The biopsy of previously treated knee joints showed new tissue formation, starting from the bone side of the osteochondral lesion.
Conclusions
Overall our data indicate that adipose tissue infusion stimulates tissue regeneration and might be considered a safe treatment for knee OA.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis (OA) of the knee is a degenerative process of the cartilage leading to pain, stiffness, and loss of joint mobility [1]. OA often starts with a focal chondral or osteochondral lesion, spreading further over the rest of the joint [2]. Common non-surgical treatments for OA are represented by pain management using corticosteroids to reduce inflammation, injection of hyaluronic acid, or physiotherapy. However, none of these forms of palliative treatments is able to totally repair or revert the damage [3], and eventually patients are subjected to joint replacement. Many efforts have been spent to study effective ways to repair focal surface lesions, in order to spare the joint from further degeneration and recover pain free movement.
Regenerative medicine based on autologous mesenchymal stem cells (MSCs) is a promising frontier for OA treatment to switch off inflammation and promote the healing process [4]. MSCs can be retrieved from multiple tissues and adipose tissue is considered their largest source [5]. Adipose tissue-derived stem cells (ASCs) are considered ideal for application in regenerative therapies, since they show multilineage differentiation ability, and hence they can form bone and cartilage [6, 7]. ASCs reside in the stromal vascular fraction (SVF) of adipose tissue, which can be considered the non-cultured form of ASCs. Since cultured-expanded ASCs need high manipulation in laboratory setting, while SVF can be more easily harvested after collagenase treatment, SVF has been more commonly used for orthopaedic clinical settings. Nevertheless, it is crucial to deeply wash SVF after collagenase treatment to eliminate any collagenase trace before reinjection.
In this study, patients affected by arthritis of knee underwent arthroscopy and were treated with injection of autologous adipose tissue to promote healing of the joint lesion. We evaluated safety, feasibility and effectiveness of intra-articular delivery of adipose tissue.
Materials and methods
Study inclusion/exclusion criteria
The main characteristics of patients are reported in Table 1. Inclusion criteria were men and women, with body mass index (BMI) > 20 kg/m2, regular renal and coagulation conditions, and classified according to the Kellgren-Lawrence grading scale for the radiographic osteoarthritis classification (1 to 4 scale, with 1 for beginning signs of OA and 4 for end stages of OA). The majority of the population (11/20 patients) had grade II knee OA, 6/20 patients were grade III and 3/20 patients grade I. Exclusion criteria were end stage patients (grade IV) OA, (BMI) > 39 kg/m2; patients who underwent surgical procedures other than diagnostic arthroscopy (such as meniscectomy or anterior cruciate ligament reconstruction, synoviectomy, etc.); patients with osteochondral focal lesions, which we further treated with microfractures or nanotunneling (Mitek DePuy Synthes USA) or with clinically relevant axial defects, outcome of articular fractures; patients currently treated with corticosteroids and hyaluronic acid injection to the affected knee joint, within the previous six months. All patients underwent the surgical procedure after signing informed consent, according to the Local Independent Ethics Committee permission (IRB).
Surgical procedure
The selected patients underwent spinal anaesthesia and intra-operative antibiotic prophylaxis with a second generation cephalosporin. The procedure involves subcutaneous abdominal liposuction, diagnostic knee arthroscopy, and intra-articular injection of adipose tissue prepared according to a modified Coleman technique (see below).
Adipose tissue harvesting
Patients underwent liposuction of the sub-abdominal adipose tissue. Patients were infused with adrenaline (1 mg/ml) in 500 ml of NaCl 0.9% solution to mobilize adipose tissue through a mini sovra-pubic access. Low-pressure liposuction with fenestrated blunt cannula was used to harvest adipose tissue, according to Coleman technique [8, 9]. The lipoaspirates were centrifuged at 3000 rpm for three minutes to collect the fat phase: a mean volume of 35 ml of this processed adipose tissue, containing ASCs, was obtained.
Knee arthroscopy and infusion
The knee diagnostic arthroscopy was performed through antero-lateral and antero-medial portals with pneumatic tourniquet positioned at the root of the thigh. This procedure allowed to confirm the grading of the chondral damage as previously determined using MRI. During the arthroscopy, we further assessed the presence of associated lesions like meniscal tears, cruciate ligament lesions, synovitis, focal osteochondral lesions, loose bodies, etc. Before the suture of the portals, using intra-articular view, a drainage tube was positioned and secured. At the end of the procedure, 35 ml of processed adipose tissue containing ASC was injected intra-articularly through the drainage tube which was further removed.
Post-operative treatment
All patients were discharged in the first post-operative day. Weight-bearing was avoided, and the leg was immobilized for ten days post-operatively. In this period, only isometric exercises for the quadriceps were allowed. Patients were further sent to physiotherapy to recover full articulation of the joint, muscular tone, and the correct gait pattern.
Assessment of pain and mobility
Knee pain and function were evaluated using the Western Ontario and McMaster Universities Arthritis Index (WOMAC) questionnaire. It consists of 24 questions on pain, stiffness, and daily activity, and patients’ answers were converted to numeric value. Patients were also subjected to a VAS (visual analogue scale) pain scale questionnaire, values ranging from 0 (no pain) and 10 (worst possible pain). WOMAC and VAS were evaluated before and after treatment at intervals of three, six and 18 months.
X-ray and magnetic resonance imaging
Each patient underwent pre-operative X-ray by weight-bearing antero-posterior and lateral radiographs of the knee. Results were graded according to the Kellgren-Lawrence system. Moreover, before surgery and at 18 months from the adipose tissue injection, each patient underwent 1.5 T MRI examination of the knee. MRI images were reviewed by radiologist before surgery and were considered suitable for the Outerbridge grading system (1 to 4 scale, with 1 for softening of articular cartilage and 4 corresponding to exposed bone). The MRI protocol provided qualitative morphological sequences (sagittal T1 FSE, sagittal 3D Cube, axial T2 and coronal T2 MERGE for evaluation of chondropathy, and for any morphological assessment). A functional compositional evaluation of cartilages was done by axial and sagittal T2 mapping. The post-processing was done on Advantage Workstation 4.6 (General Electric).
SVF isolation from adipose tissue
To perform in vitro experiments, SVF was isolated as previously described [7]. Briefly, 10 ml of lipoaspirates were subjected to enzymatic digestion with Collagenase NB4 (0.3 U/ml, (Serva Electrophoresis) using a tube rotator for 40 minutes at 37 °C. The activity of the enzyme was neutralized by the addition of DMEM low glucose + 10% FBS (Aurogene). SVF pellet was then passed through cell strainers, washed by saline solution, collected, and counted.
Analysis of ASCs phenotype
Samples from SVF were stained for mesenchymal markers to analyze the ASCs phenotype. The following staining procedure was performed with monoclonal antibodies (moAb) fluorocrome-conjugated and isotypic controls: human CD105 PE (Invitrogen), CD73 FITC (kindly provided by Prof. Malavasi, University of Turin), CD44 FITC, CD45 PerCP, CD271 APC, IgG1 PE, IgG1 APC, and IgG2a PerCP (Miltenyi Biotech), CD90 PerCP (Biolegend), IgG1 FITC (Immunostep). About 104 events/sample were used for capture with CellQuest software. All data were analyzed with Flowlogic software (Miltenyi Biotec).
Evaluation of chondrogenic potential of ASCs in vitro
SVF cells were seeded in T25 flasks and cultured in DMEM low glucose with 10% FBS, 2 mM glutamine, 1% antibiotics (Gibco, Life Technologies) to obtain a pure population of ASCs. Next, ASCs were cultured with StemPro Chondrogenesis Differentiation kit (Gibco, Life technologies) to study their chondrogenic ability, according to the manifacturers’ instructions. After 60 days, cells were stained for aggrecan. As negative control, ASCs were maintained in DMEM. By scanning electron microscopy (SEM) analysis, according to previously published protocol [10], we tested the ability of ASCs and SVF to create cartilage on SmartBone®, a commercially available composite xenohybrid bone scaffold [11].
Staining procedures
Immunofluorescence staining with moAb Aggrecan (Clone 969D4D11 Invitrogen; 1:25) was performed using appropriate Rodamin (Chemicon 1:100) conjugated isotype-specific secondary antibody. Slides were examined; microphotographs were taken using a DMLA Leica microscope equipped with a digital camera (Leica DFC 425C). Images were acquired using LAS software (Leica Application Suite).
Alcyan Blue staining was performed to highlight generic glycosaminoglycans in cyan. Immunohistochemistry was performed on new formed tissue on SmartBone® and knee joint biopsy: tissue sections were incubated with the following primary mouse moAbs from Abcam: COLL-1 (ab34710, 1:400 dilution), OCN (ab93876, 1:250 dilution), TGF-β (ab92486, 1:150 dilution). The endogenous peroxidase activity was inhibited by the addition of ultraView Universal DAB Detection Kit (Ventana). All samples were counter-stained with Mayer’s hematoxylin solution (Roche) and mounted with a Kaiser’s glycerol gelatin. Slides were examined double-blind and microphotographs were taken using an Olympus BX51 microscope equipped with a digital camera (Nikon DCS E995).
Results
Concentrated adipose tissue injection is effective in pain control
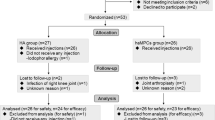
Eighteen patients completed the clinical follow-up at 18 months, whereas two patients left the study and underwent total knee replacement surgery respectively after 12 and 14 months from the treatment with adipose tissue. Overall, all patients reported an improvement of the VAS and the WOMAC scores, including the patients who subsequently decided to undergo arthroplasty. At pre-operative time, the mean VAS score was significantly reduced (7.053 ± 0.4) compared to the three post-operative time points examined: 3.321 ± 0.49; 3.011 ± 0.5 and 3.337 ± 0.6, p < 0.0001 (Fig. 1a). Similarly, the mean WOMAC score was also significantly reduced from pre-operative time (45.91 ± 2.8) to the three post-operative points examined: 27.47 ± 3.02, 15.84 ± 2.5, 12.97 ± 2.3, p < 0.0001 (Fig. 1b). The two patients who left the study were 65- and 67-year-old females with BMI respectively of 37 and 38, borderline to exclusion criteria. Both patients did not performed a correct physiotherapy post-operatively due to poor compliance.

Pre-operative VAS (a) and WOMAC scores (b) are significantly reduced at 3–6-18-month post-operative, * p < 0.0001
Radiological evaluation analysis
Regarding morphological assessment of chondropathy, there was no change between the Outerbridge grade assigned to each patient before and after infusion of adipose tissue in the MRI studies at 18 months post-operation. In ten patients, the T2 mapping was performed on the medial femoral-tibial compartment, and the lateral compartment was investigated in five patients. T2 mapping evaluations were kept independent in all compartments. The images analyses were performed on the compartment where most of the cartilage damage was documented. At 18 months, the two patients who underwent knee arthroplasty did not perform MRI.
Adverse events
Most patients reported the feeling of a “tied knee,” unable to move freely, but this symptom progressively waned one month after the operation. One patient complained of the appearance of an indolent swelling in suprapatellar area two months after surgery. Ultrasounds showed a thickening of synovial layer of suprapatellar recess, surrounded by a thick rim of adipose tissue that progressively reduced at further ultrasound controls performed three and six months later. No cases of infection, thrombo-embolism, adverse reaction at knee level, and worsening of the arthritic symptoms have been reported. Two patients decided to undergo knee replacement and abandoned the study 12 and 14 months after the concentrated adipose tissue infusion, due to persistent albeit decreased pain, as previously described.
ASCs and SVF show osteochondral differentiation ability in vitro
The number of ASCs contained in the adipose SVF can vary widely, as previously reported [12, 13]. We obtained nucleated cells ranging from 560,000 to 3,000,000 cells per gram of adipose tissue (Supplementary Table 1). Infusions in OA knee were performed with 35 ml of concentrated adipose tissue, containing a mean number of SVF cells of 31.220.000 ± 268.426, with a mean ASC percentage of 14.2% (range: 2.7 to 18%), expressing CD105, CD44, CD90, CD73, CD271 expression, and CD45 negative (Fig. 2a–f). These cells showed in vitro ability to differentiate into osteoblasts (Obs) and chondrocytes, according to the different stimuli received. Indeed, after 15 days of culture in osteogenic medium, ASCs differentiated into Obs, expressing ALP (Fig. 2g), and were able to mineralize after 60 days (Fig. 2h). ASCs cultured with chondrogenic medium, differentiated into aggrecan positive chondrocytes (Fig. 2i). SVF cells were also able to form cartilage when plated on SmartBone ® (Fig. 3a), which was positive for Alcian Blue and TGF staining (Fig. 3b–c). The presence of newly formed tissue was also confirmed by SEM analysis (Fig. 3d).

In SVF the presence of ASCs was analyzed by flow cytometry, ASCs expressed CD105, CD44, CD90, CD73, and CD271 and were CD45 negative (a–f). These ASCs showed ability to differentiate into Obs, expressing ALP, after culture in osteogenic medium (g) and mineralize (h, Von Kossa staining). ASCs cultured with chondrogenic medium, differentiated into Aggrecan positive chondrocytes as shown by immunofluorescence (i, red for Aggrecan and blue for DAPI)

SVF cells, plated on SmartBone ® were also able to form cartilage (A), which was positive for Alcian Blue (b) and TGF staining (c). SEM analysis confirmed the presence of new formed tissue (d)
Immunohistochemical analyses of knee joint biopsies
The knee joints of the two patients who underwent knee prosthesis procedure after adipose tissue infusion were collected, histologically studied, and compared with those of OA patients (matched for age, sex, and OA grading) subjected to arthroplasty alone. In both the joints previously treated with adipose tissue infusion, we detected the presence of new tissue formation starting from the bone side of the osteochondral lesion (Fig. 4a), whereas this type of neo-tissue formation was not detectable in joints of untreated cases (Fig. 4b). Looking at the bone compartment of the joint, we showed a strong bone remodeling (Fig. 5a): the active cells were Obs expressing TGF-β and OCN, and negative for collagen I (Fig. 5b–d).

H&E staining showed the presence of new tissue formations in knee biopsy of patient previously treated with concentrated adipose tissue injection (a). Neo-tissue formation was not evident in joint of untreated patients (b)

A strong bone remodeling is present in the bone compartment of the joint (a). A deep magnification of the indicated area showed the presence of active Obs expressing TGF-β (b) and OCN (c) and negative for collagen I (d)
Discussion
Many recent studies had demonstrated the safety and efficacy of the use of autologous adipose-derived SVF and ASCs for treatment of OA [14,15,16]. Those therapeutic approaches significantly improved the cartilage and subchondral bone formation, protecting against arthritic processes [12, 13]. Since isolation of both SVF and ASCs requires sample manipulation, as collagenase treatment or in vitro cell expansion, we decided to investigate the safety and efficacy of knee OA treatment with infusion of lightly manipulated adipose tissue. This procedure requires a centrifugation of the lipoaspirate according to the principles of the Coleman technique, reducing the possible disadvantages correlated to any further manipulation of samples. To date, adipose tissue transfer is commonly used in plastic surgery, particularly for mammary augmentation or tissue reconstruction [17,18,19]. In this study, we report that patients treated with concentrated adipose tissue injection showed a significant improvement of VAS and WOMAC scores, with a significant pain reduction and increased mobility at 3, 6, and 12 months from the infusion. We further observed that rehabilitation was more effective in active patients than in sedentary ones, confirming recent experimental data, obtained in animal model, showing that exercise may enhance proliferative ability and decrease adipogenic ability of MSCs [20]. As further confirmation of the importance of mechanical stretch and load, recent data demonstrated that they promote in MSCs both osteogenesis and chondrogenesis [21].
We did not register adverse events, such as infection, thrombo-embolism, adverse reaction at knee level, and worsening of the arthritic symptoms, confirming recent literature data, which report safety of MSC-based therapies for orthopaedic conditions [16].
All the patients enrolled in the study underwent diagnostic arthroscopy to identify lesions known or undiagnosed at previous imaging examinations and eventually amenable to further treatment. There is a relevant amount of studies regarding the placebo effect of arthroscopy alone in patients affected by knee OA, reporting a decrease in the pain score of average 10%, while the functional results do not improve over 10% in most grading system used [22, 23]. Furthermore, our unpublished observations show that the arthroscopic thorough articular wash allows a complete removal of inflammatory synovial fluid, which strongly interferes with ASC adhesion in vitro. Based on the reported parameters of pain and function, we consider the obtained results, albeit preliminary, a positive input for further insights.
Regarding morphological assessment of chondropathy, we did not observe any increase in the thickness of cartilage after 18 months from infusion. T2 mapping was largely applied to evaluate the response to regenerative treatment of knee chondropathy, including ASC infusion. However, there is a lack of general agreement about when the regenerative chondral response becomes appreciable at morphological or compositional MRI evaluation. Indeed, some authors refer that it would be appreciable at least 24 months after the treatment [24, 25], unless studied by miniaturized MRI equipment [26].
We isolated and characterized SVF from the patients’ adipose tissue samples, reporting a variable number of ASCs. One of the reasons for such variation is represented by the individual differences: physiologically, patients have different adipose texture and density. Thus, equal to the same volume of adipose tissue infused, the number of ASCs may vary, suggesting that the regeneration does not correlate directly with the number of ASCs, but it might depend on interaction between cells and factors in the adipose tissue and local precursors present in the joints [27]. Moreover, a visco-elastic effect of the infused adipose extract was previously discussed [28]. Indeed, we envision a simple feeder layer activity of the extracellular components for the vitality of ASCs after infusion.
A fundamental barrier for the restoration of cartilage integrity is its low intrinsic repair capacity, which depends on poor vascularization, low cellularity in adult tissue, and the presence of a dense hydrated extracellular matrix hindering cell migration to and from the injury site. Moreover, in OA patients, MSCs’ differentiative and proliferative potential decreases [29]. Thus, in an early phase, the adipose tissue infusion can disrupt this OA “vicious circle” boosting the local precursors and inhibiting the local inflammation through its immunomodulatory effects. We previously showed that SVF cells can differentiate into Obs [10], and now, we reported their chondro-differentiation ability, responding to the different conditioned medium. To further confirm the ability of ASCs to form new cartilage, we plated them on a bone surface with chondrogenic medium, showing the formation of new cartilaginous tissue, as demonstrated by different stainings. This result supports the histological data derived from the knee joint intra-operative biopsy. Indeed, in knee joints previously treated with concentrated adipose tissue infusion, we detected the presence of new tissue formation starting from the bone side of the osteochondral lesion, with the presence of a strong bone remodeling, whereas in joint of untreated cases, this neo-tissue formation was not evident. The effective subchondral bone formation has also been shown in knee condyle osteonecrosis, where treatment with bone marrow-derived MSCs showed improvement on cartilage and bone marrow lesions observed at the site of bone marrow subchondral injection [30]. The reported data suggest an initial subchondral healing process, which could be followed by reconstruction of the chondroid matrix. This process is slow, and it is detectable with the normal imaging techniques only after 24 months, as reported by literature data. Therefore, our study is still unable to clarify it, and it requires further future analyses. The availability to examine adipose tissue-treated knee joint was unexpected and occurred for two patients only; thus, the observations reported must be considered as descriptive, suggesting, at most, a healing effect when compared to untreated patients. Our proposed treatment, with concentrated adipose tissue injection in the knee joint, could represent an alternative to the implantation with autologous chondrocyte or the synovium-derived stem cell, which need ex vivo expansion before their use to treat cartilage defects [31].
In conclusion, treatment of knee OA with concentrated adipose tissue infusion resulted safe as a diagnostic arthroscopy and led to an improvement both in terms of pain and function in all patients of this study.
References
Dunlop DD, Manheim LM, Song J, Chang RW (2003) Health care utilization among older adults with arthritis. Arthritis Rheum 49(2):164–171. https://doi.org/10.1002/art.11003
Braman JP, Bruckner JD, Clark JM, Norman AG, Chansky HA (2005) Articular cartilage adjacent to experimental defects is subject to atypical strains. Clin Orthop Relat Res (430):202–207
Coleman CM, Curtin C, Barry FP, O'Flatharta C, Murphy JM (2010) Mesenchymal stem cells and osteoarthritis: remedy or accomplice? Hum Gene Ther 21(10):1239–1250. https://doi.org/10.1089/hum.2010.138
Caplan AI (1991) Mesenchymal stem cells. J Orthop Res 9(5):641–650. https://doi.org/10.1002/jor.1100090504
Zuk PA, Zhu M, Ashjian P, De Ugarte DA, Huang JI, Mizuno H, Alfonso ZC, Fraser JK, Benhaim P, Hedrick MH (2002) Human adipose tissue is a source of multipotent stem cells. Mol Biol Cell 13(12):4279–4295. https://doi.org/10.1091/mbc.E02-02-0105
Zuk PA, Zhu M, Mizuno H, Huang J, Futrell JW, Katz AJ, Benhaim P, Lorenz HP, Hedrick MH (2001) Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng 7(2):211–228. https://doi.org/10.1089/107632701300062859
Roato I, Alotto D, Belisario DC, Casarin S, Fumagalli M, Cambieri I, Piana R, Stella M, Ferracini R, Castagnoli C (2016) Adipose derived-mesenchymal stem cells viability and differentiating features for orthopaedic reparative applications: banking of adipose tissue. Stem Cells Int 2016:4968724. https://doi.org/10.1155/2016/4968724
Coleman SR, Saboeiro AP (2007) Fat grafting to the breast revisited: safety and efficacy. Plast Reconstr Surg 119(3):775–785; discussion 786–777. https://doi.org/10.1097/01.prs.0000252001.59162.c9
Pu LL, Coleman SR, Cui X, Ferguson RE Jr, Vasconez HC (2008) Autologous fat grafts harvested and refined by the Coleman technique: a comparative study. Plast Reconstr Surg 122(3):932–937. https://doi.org/10.1097/PRS.0b013e3181811ff0
Roato I, Belisario DC, Compagno M, Verderio L, Sighinolfi A, Mussano F, Genova T, Veneziano F, Pertici G, Perale G, Ferracini R (2018) Adipose-derived stromal vascular fraction/xenohybrid bone scaffold: an alternative source for bone regeneration. Stem Cells Int 2018:4126379. https://doi.org/10.1155/2018/4126379
Pertici G, Rossi F, Casalini T, Perale G (2014) Composite polymer-coated mineral grafts for bone regeneration: material characterisation and model study. Ann Oral Maxillofac Surg 2(1):4
Pak J, Lee JH, Park KS, Park M, Kang LW, Lee SH (2017) Current use of autologous adipose tissue-derived stromal vascular fraction cells for orthopedic applications. J Biomed Sci 24(1):9. https://doi.org/10.1186/s12929-017-0318-z
Perdisa F, Gostynska N, Roffi A, Filardo G, Marcacci M, Kon E (2015) Adipose-derived mesenchymal stem cells for the treatment of articular cartilage: a systematic review on preclinical and clinical evidence. Stem Cells Int 2015:597652. https://doi.org/10.1155/2015/597652
Pers YM, Rackwitz L, Ferreira R, Pullig O, Delfour C, Barry F, Sensebe L, Casteilla L, Fleury S, Bourin P, Noel D, Canovas F, Cyteval C, Lisignoli G, Schrauth J, Haddad D, Domergue S, Noeth U, Jorgensen C (2016) Adipose mesenchymal stromal cell-based therapy for severe osteoarthritis of the knee: a phase i dose-escalation trial. Stem Cells Transl Med 5(7):847–856. https://doi.org/10.5966/sctm.2015-0245
Nguyen PD, Tran TD, Nguyen HT, Vu HT, Le PT, Phan NL, Vu NB, Phan NK, Van Pham P (2017) Comparative clinical observation of arthroscopic microfracture in the presence and absence of a stromal vascular fraction injection for osteoarthritis. Stem Cells Transl Med 6(1):187–195. https://doi.org/10.5966/sctm.2016-0023
Centeno CJ, Al-Sayegh H, Freeman MD, Smith J, Murrell WD, Bubnov R (2016) A multi-center analysis of adverse events among two thousand, three hundred and seventy two adult patients undergoing adult autologous stem cell therapy for orthopaedic conditions. Int Orthop 40(8):1755–1765. https://doi.org/10.1007/s00264-016-3162-y
Del Vecchio D (2009) Breast reconstruction for breast asymmetry using recipient site pre-expansion and autologous fat grafting: a case report. Ann Plast Surg 62(5):523–527. https://doi.org/10.1097/SAP.0b013e3181a23f08
Al Sufyani MA, Al Hargan AH, Al Shammari NA (2016) Autologous fat transfer for breast augmentation: a review. Dermatol Surg 42(11):1235–1242. https://doi.org/10.1097/DSS.0000000000000791
Laloze J, Varin A, Gilhodes J, Bertheuil N, Grolleau JL, Brie J, Usseglio J, Sensebe L, Filleron T, Chaput B (2018) Cell-assisted lipotransfer: friend or foe in fat grafting? Systematic review and meta-analysis. J Tissue Eng Regen Med 12(2):e1237–e1250. https://doi.org/10.1002/term.2524
Liu SY, He YB, Deng SY, Zhu WT, Xu SY, Ni GX (2017) Exercise affects biological characteristics of mesenchymal stromal cells derived from bone marrow and adipose tissue. Int Orthop 41(6):1199–1209. https://doi.org/10.1007/s00264-017-3441-2
Song Y, Tang Y, Song J, Lei M, Liang P, Fu T, Su X, Zhou P, Yang L, Huang E (2018) Cyclic mechanical stretch enhances BMP9-induced osteogenic differentiation of mesenchymal stem cells. Int Orthop 42(4):947–955. https://doi.org/10.1007/s00264-018-3796-z
Moseley JB, O'Malley K, Petersen NJ, Menke TJ, Brody BA, Kuykendall DH, Hollingsworth JC, Ashton CM, Wray NP (2002) A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med 347(2):81–88. https://doi.org/10.1056/NEJMoa013259
Amin NH, Hussain W, Ryan J, Morrison S, Miniaci A, Jones MH (2017) Changes within clinical practice after a randomized controlled trial of knee arthroscopy for osteoarthritis. Orthop J Sports Med 5(4):2325967117698439. https://doi.org/10.1177/2325967117698439
Koh YG, Choi YJ, Kwon SK, Kim YS, Yeo JE (2015) Clinical results and second-look arthroscopic findings after treatment with adipose-derived stem cells for knee osteoarthritis. Knee Surg Sports Traumatol Arthrosc 23(5):1308–1316. https://doi.org/10.1007/s00167-013-2807-2
Krusche-Mandl I, Schmitt B, Zak L, Apprich S, Aldrian S, Juras V, Friedrich KM, Marlovits S, Weber M, Trattnig S (2012) Long-term results 8 years after autologous osteochondral transplantation: 7 T gagCEST and sodium magnetic resonance imaging with morphological and clinical correlation. Osteoarthr Cartil 20(5):357–363
Lalande C, Miraux S, Derkaoui SM, Mornet S, Bareille R, Fricain JC, Franconi JM, Le Visage C, Letourneur D, Amedee J, Bouzier-Sore AK (2011) Magnetic resonance imaging tracking of human adipose derived stromal cells within three-dimensional scaffolds for bone tissue engineering. Eur Cell Mater 21:341–354
Mussano F, Genova T, Corsalini M, Schierano G, Pettini F, Di Venere D, Carossa S (2017) Cytokine, chemokine, and growth factor profile characterization of undifferentiated and osteoinduced human adipose-derived stem cells. Stem Cells Int 2017:6202783. https://doi.org/10.1155/2017/6202783
Bosetti M, Borrone A, Follenzi A, Messaggio F, Tremolada C, Cannas M (2016) Human lipoaspirate as autologous injectable active scaffold for one-step repair of cartilage defects. Cell Transplant 25(6):1043–1056. https://doi.org/10.3727/096368915X689514
Murphy JM, Dixon K, Beck S, Fabian D, Feldman A, Barry F (2002) Reduced chondrogenic and adipogenic activity of mesenchymal stem cells from patients with advanced osteoarthritis. Arthritis Rheum 46(3):704–713. https://doi.org/10.1002/art.10118
Hernigou P, Auregan JC, Dubory A, Flouzat-Lachaniette CH, Chevallier N, Rouard H (2018) Subchondral stem cell therapy versus contralateral total knee arthroplasty for osteoarthritis following secondary osteonecrosis of the knee. Int Orthop. https://doi.org/10.1007/s00264-018-3916-9
Kubosch EJ, Heidt E, Niemeyer P, Bernstein A, Sudkamp NP, Schmal H (2017) In-vitro chondrogenic potential of synovial stem cells and chondrocytes allocated for autologous chondrocyte implantation - a comparison: sSynovial stem cells as an alternative cell source for autologous chondrocyte implantation. Int Orthop 41(5):991–998. https://doi.org/10.1007/s00264-017-3400-y
Acknowledgments
This work was supported by Compagnia di San Paolo and CRT Foundations, Banca d’Italia, and Fondazione Ricerca Molinette ONLUS. The authors thank Dr. Dario Picenoni, at SAMM (Politecnico di Milano), for his technical contribution to SEM analyses, Dr. Francesca Veneziano for immunohistochemistry.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Giuseppe Perale is affiliated to the Company manufacturing the bone substitute used in this study
Electronic supplementary material
Supplementary Table 1
(DOCX 13 kb)
Rights and permissions
About this article

Cite this article
Roato, I., Belisario, D.C., Compagno, M. et al. Concentrated adipose tissue infusion for the treatment of knee osteoarthritis: clinical and histological observations. International Orthopaedics (SICOT) 43, 15–23 (2019). https://doi.org/10.1007/s00264-018-4192-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-018-4192-4