
Abstract
Purpose
Three-dimensional computerised tomography (3DCT) can provide comprehensive patho-anatomy of complex bone on a single image. Though important, the key articular quadrilateral [Q] surface has not been a part of the systems developed for classifying acetabulum fractures. The purpose of the study was to simplify the complexity of classification by the direct sign of the broken Q surface which lies opposite the entire floor of the acetabulum.
Methods
The study reviewed 84 acetabular fractures using 3DCT images of the interior lateral view (IL) taken between June 2002 to December 2009. Fractures were traditionally classified using the anatomical disruption, plane of the fracture line breaking through or not through the bone column described by Judet and Letournel.
Results
The 3D images clearly show the primary site of impaction acting on the acetabulum and the whole course of fracture. The image could not illustrate disruption of the lips of acetabulum and congruity of hip joints in 20 cases of wall (W) fracture. There were 30 transverse (T) fractures classified when the acetabulum was divided horizontally from front to back into upper and lower parts and 34 cases of column (C) fracture when the main vertical lines run and collide along the anterior and posterior column.
Conclusions
This study showed that the well-known complex fractures can be satisfactorily classified with the broad flat inner plane of the Q surface.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The acetabulum, vinegar-cruet in Latin [1], is a cup-shaped cavity located within an arch produced by two columns of bone. Judet and Letournel, whose treatise analyses fractures of the acetabulum, named the columns in reference to their double embryological origin [2–4]. The iliopubic column (anterior column) extends from the superior iliac crest to the pubic symphysis. The thicker structure of the ilioischial column (posterior column) extends from the inferior sacroiliac joint and sciatic notch to the ischial tuberosity. The described column resembles (λ) the eleventh letter of the Greek alphabet (Fig. 1a) (the inverted Modern English Y letter). The iliac wing stands for the forked holder connecting with the component of the anterior and posterior columns. The roof (superior dome) of the acetabulum is located at the summit of the two columns. The floor of the acetabulum is found between the columns and provides most of the articular surface for the femoral head. The corresponding surface on the opposite side of the acetabular floor is the quadrilateral (Q) surface (Fig. 1b). Even though the quadrilateral surface is an important anatomical structure and essential to surgical reduction of fractures of the acetabulum, it has not been a part of the systems developed for classifying these fractures [5–10].

a The whole column of innominate bone resembles the inverted modern English Y letter. The iliac wing stands for the forked holder connecting with the component of the anterior and posterior columns. b The thin flat quadrilateral surface lies just opposite the floor of acetabulum
Considerable radiological data and measurements have been used to describe the characteristic pattern of the fractures [11–17]. However, this evidence was indirect and always incomplete. Recently, three-dimensional computerised tomography (3DCT) radiographs have become more readily available and have been enthusiastically accepted [8–28]. The technique’s ability to provide comprehensive evidence on a single radiographic image reduces the amount of imaging and the extensive mental imagery required. In the preface to the second edition of his textbook, Letournel stated that the traditional tracing of the lines on plain films was inadequate for an understanding of the fracture. Later, he used 3DCT tomography to confirm his proposed ten categories and began to use the scan routinely after 1989 [4].
Although numerous studies on 3D imaging of acetabular fractures have been published, the number of reported cases are quite few and imperfect [18, 19]. The purpose of this study aimed to simplify the complexity of acetabular fractures with findings of the broken quadrilateral (Q) surface seen on 3D images of the isolated ilium, the interior lateral (IL) view.
Materials and methods
The 3DCT images of 84 acetabular fractures were taken between June 2002 and December 2009 at Lerdsin Hospital in Bangkok, Thailand. The research protocol was approved by the Hospital Ethical and Research Review Board. The images used in the study were created by reformatting Somatom Plus and Plus S Computed Tomography System (Siemens) images. The scanning parameters were: slice thickness (collimation) 5 mm, table feed 5 mm (pitch = 1), threshold value 150 Hounsfield units, resolution 512 matrix.
The isolated ilium bone by segmentation process has two views, i.e. the interior lateral view (IL) and the exterior lateral view (EL) (Fig. 2). The IL view was used to illustrate the broad flattering inner surface of innominate bone with its Q surface which lies opposite the acetabular floor. The whole breaking configuration of the broken Q surface and the intact columnar architecture were the main characters used in the differentiation. The image can be simply verified as follows: the primary site of impaction seen as maximum bone comminution, and the primary fracture line breaking along the anterior or posterior column horizontally to be a transverse fracture or vertically to be a column fracture. The incomplete fracture line can be described as a single column fracture; an extended secondary fracture line or lines beyond the acetabulum or the Q surface into its adjacent column can be described as both columns fracture along with details of all detached fragments such as number, size, shape and amount of displacement.

The images of interior lateral (IL) view (a) and exterior lateral view (b) clearly show boundaries and dimensions of the inner and outer sides of the ilium bone, respectively. Fracture lines splitting the whole ilium can be better verified on IL view
Fractures were then classified into wall (W), transverse (T) and column (C) using anatomical disruption and plane of the fracture line breaking through or not through bone columns described by Judet and Letournel [2, 4].
Results
There were 68 males and 16 females in the study with an average age of 38.6 years (range 18–68 years). The fractures were caused by motorcycle accidents (44 patients), automobile or truck accidents (30 patients) and falls from significant height (ten patients). Fifty-two fractures involved the right acetabulum and 32 fractures involved the left acetabulum. Associated long bone fractures were found in 41 cases, four of which were open fractures. Four patients had associated facial fractures and three had skull fractures. Thirty patients had multiple organ injuries and nine patients had primary nerve injuries. Urethral injuries and blunt abdominal trauma were reported in ten and 12 patients, respectively. One was associated with open tendon injury of the index finger.
The images of the interior lateral (IL) view clearly show greater detail of the whole course of the fracture breaking the Q surface with or without involvement of its two adjacent structural columns and the obturator foramen. By the imaging characters, fractures were arranged into
-
- Wall fractures (20 cases):
-
These fractures can be clearly shown on plain radiographs and their corresponding 3DCT images. There was no involvement of the Q surface. The IL view can not illustrate the disruption of the lips of acetabulum and congruity of hip joints. Only two cases of associated fractures that involved the posterior column were clearly noted.
- T fractures (30 cases):
-
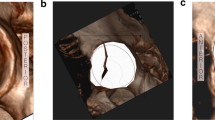
These were classified when the acetabulum was divided horizontally from front to back into upper and lower parts. The striking primary site of impaction was located at the superior dome of acetabulum or at the pubo-acetabular junction of the anterior column. Subtypes were graded by the primary line extending and breaking through or not through the posterior column. There were 15 pure T fractures, of which six could be graded as single anterior column (Fig. 3a) while nine were both columns by the complete emerging line (Fig. 3b). The more serious injury of four cases had T—or Y—shaped fractures of the Q surface (acetabular floor) by a secondary line running toward the obturator ring (Fig. 3c). Eleven cases had associated fractures of the posterior wall and comminuted iliac crest (Fig. 3b) seen on plain radiographs in eight and three cases, respectively.
Fig. 3 
Pure T fracture of left acetabulum in the interior lateral (IL) view (a) shows incomplete transverse fracture line not emerging through the Q surface. IL view (b) shows complete transverse fracture line emerging through the Q surface into the posterior column. The IL views C1–3 show more severe T- or Y-shaped fractures by secondary fracture line(s)
- C fractures (34 cases):
-
These occur when the main vertical lines run along the iliopectineal or iliopelvic component of the anterior column and divide the innominate bone into main medial and lateral parts (Fig. 4). The centre of impaction was clearly located at the Q surface. Fractures can be arranged in order of severity with the character of the Q surface and its extension outside the surface (Fig. 5):
-
C 1—Less severe or mild impaction (4 cases, Fig. 4a). Initial site of impaction can be located as a triangular-shaped fragment of the Q surface formed by the bisection of two incomplete fracture lines.
-
C 2—Moderate impaction (11 cases, Fig. 4b) is more severe by the extension of a second horizontal fracture lines into adjacent columns. The primary fracture line is more aggressive with an intact obturator foramen (Fig. 4b 2).
-
C 3—Most severe impaction (19 cases) (Fig. 4c). The extended vertical line passes along the anterior column and crashes completely from the iliac crest through the obturator ring (Fig. 4c 2). The severity of the impaction can be indicated by the extension of primary vertical fracture lines, secondary horizontal fracture lines, elevation of the Q surface, the presence of bone gap and the disruption of the obturator ring. Intrapelvic medial displacement of the actabular floor is better seen on 3DCT of the whole pelvis (Fig. 4b 1). Eight of these show the vertical line passing far anteriorly with no involvement and involvement of the Q surface in an equal number of four cases each (Fig. 6).
Fig. 4 
a Less severe C fracture, 3D AP image (A 1 ) shows left central hip dislocation. Interior lateral (IL) view (A 2 ) shows a triangular shaped fragment of broken Q surface or acetabular floor. b Moderate severe C fracture (B 1 ) 3D AP image and IL view (B 2 ) show a moderate severe injury by the extension of the primary vertical fracture line. c Most severe C fracture (C 1 ) 3D AP image and IL view (C 2 ) show severe impaction by the aggressive extension of primary and secondary fracture lines breaking through columns
Fig. 5 
Interior lateral views showing striking characters of various impaction of C fractures in ascending order of severity
Fig. 6 
Most severe pure superior C fracture, 3D AP view (A 1 and A 2 ) show complete vertical fracture line breaking along anterior part of ilium through acetabular roof; the anterior femoral head is exposed with intact Q surface. 3D AP view (B 1 ) shows separated fragment of anterior ilium with exposed right femoral head. The IL view (B 2 ) shows transverse fracture line dividing the Q surface
-




Discussion
The landmark classification of acetabular fractures as proposed by Letournel and Judet (established in1961–4) has survived the test of time and is the most comprehensive and most widely used system. However, the classification scheme is relatively complex with a wide variation in the interpretation [13, 14, 17, 22, 29–32]. Some authors have suggested that the system might be too complicated and too difficult for average orthopaedic surgeons [29–33]. The reasons have been due to high variation of the multidirectional acting force, complexity of the articular acetabular cup with its adjacent connection and the imperfect radiographic evidence to trace multiple fracture lines overlaid with the well defined structural columns [4, 12, 17, 22].
Certainly, one-dimensional radiological evidence has poor sensitivity in the detection of complicated types of fractures. Missing evidence by underestimation is inevitable. Both column fracture, according to the universal classification, can be mistaken as single column fracture by misinterpreted ambiguous findings. The proposed arrangement of fractures (W, T, C), which is based on 3D images of consecutive series of patients, is not new. The simple to complex pattern of the presented fractures are, for the most part, consistent with those previously reported [15, 30, 31, 34]. The associated types, according to Letournel’s description, are more severe and confirmed to be the combination of various one column fractures.
Unlike the common description and drawing, this study illustrated a more informative data previously inaccessible by conventional radiographic techniques. With the imaging character of the broken Q surface, all cases of T and C fracture were substantiated to have primary acetabular involvement. The findings do localise the site of impaction with its extension, which is directly related to the magnitude and direction of the acting force as described in the text. Simple differentiation of the well-known complex fractures can be easily performed with precise location and true extent of the fracture line. The images also delineated the severity of the medially displaced fragment of floor of the acetabulum in C fracture, commonly considered as the central hip dislocation [2, 5]. Localisation of the initial site of impaction (centre of impaction) is simple and can be used as a reference point to differentiate acetabular fracture from pelvis fracture.
This interpretable information strengthens the existing knowledge by seeing things as they are. The technique can differentiate the exact primary site of impaction, particularly in the complex bony anatomy. Shape and size of each broken articular fragment as well as virtual displacement of bone and joint from different views can be directly and easily seen. The striking characteristic patterns increase knowledge and provide better understanding about the findings, as seen on plain radiographs. However, it is not the objective of this presentation to suggest 3DCT as a routine clinical practice for actabulum fracture cases. Various indirect signs on plain radiograph should be better recognised and comprehended. Apart from giving the surgeon precise fracture characters prior to surgery, the technique has been modified and used to assist screw placement in various bone procedures [35–39].
There are several limitations. The image can only outline two of the four bony fundamental landmarks (anterior and posterior column). It cannot detect any disruption of the acetabulum rim (lip or wall fracture), femoral head injury with or without dislocation, exact amount of hip joint incongruity, non displaced fracture and minimal articular impaction. The technique is useful only when fracture involves the Q surface. Recently, Pascarella et al. [40] reported an undescribed pattern of acetabular injury. There was osteochondral impaction of the posterior acetabular surface without cortical fracture of any wall or column. The impacted articular fragment of Q lamina could not be seen on IL view of 3DCT. Though the current study did not include the evaluation of inter-observer agreement, there was substantial evidence supporting the superiority of 3D images [16, 22, 26, 32, 33]. As studied by Ohashi et al. [41], the agreement of readers using radiography alone was moderate. Significant improvement was found when 3DCT was used. From the findings, significant observer difference is based on the complexity of the classification system and levels of expertise.
Conclusion
By retaining the original concept, acetabular fracture of the current 3D study are arranged by the appearance of fracture lines seen on the interior view showing the broad flattering inner surface of innominate bone. Fractures are shown to vary from mild to severe injury with multiple organ involvement. The study has addressed the first appearance of primary site of impaction acting on the acetabulum seen as broken Q surface which lies opposite to the floor of acetabulum. The image can not detect Wall fracture which is the result of force acting on rim of the acetabulum. A variety of complex T and C fractures can be accurately simplified by the true extent of fracture and its extension. Localisation the primary site of acetabular involvement is extremely important in the differentiation of fracture types.
References
Dorland (1994) Dorland’s Illustrated medical dictionary, 28th edition. Saunders, Philadelphia
Judet R, Judet J, Letournel E (1964) Fractures of the acetabulum: classification and surgical approaches for open reduction, preliminary report. J Bone Joint Surg Am 46:1615–1646
AO Foundation (2008) A short history of pelvic trauma surgery. http://www.ao-asif.ch/portal/AOFileServer/PortalFiles?FilePath=/Extranet2007/Active/_att//wor/act/Dialogue/2003_2/History_pelvic_trauma.pdf. Accessed 19 June 2008
Letournel E, Judet R (1993) Fractures of the acetabulum, 2nd edn. Springer, Berlin
Werner CM, Copeland CE, Ruckstuhl T, Stromberg J, Turen CH, Bouaicha S (2012) Acetabular fracture types vary with different acetabular version. Int Orthop 36:2559–2563
Sun BH, Li KH, Zhu Y (2011) Comment on Sen et al.: posterior wall reconstruction using iliac crest strut graft in severely comminuted posterior acetabular wall fracture. Int Orthop 35:1903–1904
Sen RK, Tripathy SK, Aggarwal S, Tamuk T (2011) Posterior wall reconstruction using iliac crest strut graft in severely comminuted posterior acetabular wall fracture. Int Orthop 35:1223–1228
Vrahas MS, Tile M (2001) Fractures of the acetabulum. In: Bucholz RW, Heckman JD (eds) Rockwood and Green’s fractures in adults, vol 2, 5th edn. Lippincott Williams & Wilkins, Philadelphia, pp 1513–1545
Matta JM (2002) Surgical treatment of acetabular fractures. In: Browner BD, Jupiter JB (eds) Skeletal trauma, volume1, 3rd edn. Saunders, Philadelphia, pp 1109–1149
Brandser E (2002) The pelvis. In: Rogers LF (ed) Radiology of skeletal trauma, 3rd edn. Churchill Livingstone, Philadelphia, pp 930–1029
Rice J, Kaliszer M, Dolan M, Cox M, Khan H, McElwain JP (2002) Comparison between clinical and radiologic outcome measures after reconstruction of acetabular fractures. J Orthop Trauma 16:82–86
Saks BJ (1986) Normal acetabular anatomy for acetabular fracture assessment: CT and plain film correlation. Radiology 159:139–145
Harris JH, Coupe KJ, Lee JS, Trotscher T (2005) Acetabular fractures revisited: a new CT-based classification. Semin Musculoskelet Radiol 9:150–160
Harris JH Jr, Coupe KJ, Lee JS, Trotscher T (2004) Acetabular fractures revisited: part 2, a new CT-based classification. AJR Am J Roentgenol 182:1367–1375
Durkee NJ, Jacobson J, Jamadar D, Karunakar MA, Morag Y, Hayes C (2006) Classification of common acetabular fractures: radiographic and CT appearances. AJR Am J Roentgenol 187:915–925
Harley JD, Mack LA, Winquist RA (1982) CT of acetabular fractures: comparison with conventional radiography. AJR Am J Roentgenol 138:413–417
Potok PS, Hopper KD, Umlauf MJ (1995) Fractures of the acetabulum: imaging, classification, and understanding. Radiographics 15:7–23
Burk DL Jr, Mears DC, Kennedy WH, Cooperstein LA, Herbert DL (1985) Three-dimensional computed tomography of acetabular fractures. Radiology 155:183–186
Pozzi Mucelli RS, Muner G, Pozzi Mucelli F, Pozzi Mucelli M, Marotti F, Dalla Palma L (1986) Three-dimensional computed tomography of the acetabulum. Eur J Radiol 6:168–177
Fishman EK, Magid D, Ney DR, Chaney EL, Pizer SM, Rosenman JG, Levin DN, Vannier MW, Kuhlman JE, Robertson DD (1991) Three-dimensional imaging. Radiology 181:321–337
White MS (1991) Three-dimensional computed tomography in the assessment of fractures of the acetabulum. Injury 22:13–19
Martinez CR, Di Pasquale TG, Helfet DL, Graham AW, Sanders RW, Ray LD (1992) Evaluation of acetabular fractures with two- and three-dimensional CT. Radiographics 12:227–242
Guy RL, Butler-Manuel PA, Holder P, Brueton RN (1992) The role of 3D CT in the assessment of acetabular fractures. Br J Radiol 65:384–389
Gautsch TL, Johnson EE, Seeger LL (1994) True three dimensional stereographic display of 3D reconstructed CT scans of the pelvis and acetabulum. Clin Orthop Relat Res 305:138–151
Haveri M, Junila J, Suramo I, Lähde S (1998) Multiplanar and 3D CT of acetabular fractures. Acta Radiol 39:257–264
Kickuth R, Laufer U, Hartung G, Gruening C, Stueckle C, Kirchner J (2002) 3D CT versus axial helical CT versus conventional tomography in the classification of acetabular fractures: a ROC analysis. Clin Radiol 57:140–145
Pretorius ES, Fishman EK (1999) Volume-rendered three-dimensional spiral CT: musculoskeletal applications. Radiographics 19:1143–1160
Attias N, Lindsey RW, Starr AJ, Borer D, Bridges K, Hipp JA (2005) The use of a virtual three-dimensional model to evaluate the intraosseous space available for percutaneous screw fixation of acetabular fractures. J Bone Joint Surg Br 87:1520–1523
Brandser E, Marsh JL (1998) Acetabular fractures: easier classification with a systematic approach. AJR Am J Roentgenol 171:1217–1228
Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H (2005) Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J Bone Joint Surg Br 87:2–9
Laird A, Keating JF (2005) Acetabular fractures: a 16-year prospective epidemiological study. J Bone Joint Surg Br 87:969–973
Beaulé PE, Dorey FJ, Matta JM (2003) Letournel classification for acetabular fractures. Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am 85-A:1704–1709
Visutipol B, Chobtangsin P, Ketmalasiri B, Pattarabanjird N, Varodompun N (2000) Evaluation of Letournel and Judet classification of acetabular fracture with plain radiographs and three-dimensional computerized tomographic scan. J Orthop Surg (Hong Kong) 8:33–37
Kumar A, Shah NA, Kershaw SA, Clayson AD (2005) Operative management of acetabular fractures. A review of 73 fractures. Injury 36:605–612
Brown GA, Willis MC, Firoozbakhsh K, Barmada A, Tessman CL, Montgomery A (2000) Computed tomography image-guided surgery in complex acetabular fractures. Clin Orthop Relat Res 370:219–226
Brown GA, Firoozbakhsh K, Gehlert RJ (2001) Three-dimensional CT modeling versus traditional radiology techniques in treatment of acetabular fractures. Iowa Orthop J21:20–24
Cimerman M, Kristan A (2007) Preoperative planning in pelvic and acetabular surgery: the value of advanced computerised planning modules. Injury 38:442–449
Vannier MW, Hildebolt CF, Gilula LA, Pilgram TK, Mann F, Monsees BS, Murphy WA, Totty WG, Offutt CJ (1991) Calcaneal and pelvic fractures: diagnostic evaluation by three-dimensional computed tomography scans. J Digit Imaging 4:143–152
Chen KN, Wang G, Cao LG, Zhang MC (2009) Differences of percutaneous retrograde screw fixation of anterior column acetabular fractures between male and female: a study of 164 virtual three-dimensional models. Injury 40:1067–1072
Pascarella R, Digennaro V, Grandi G (2011) Osteochondral impaction of the posterior acetabular surface without cortical fracture of any wall or column: an undescribed pattern of acetabular injury. J Orthop Traumatol 12:101–105
Ohashi K, El-Khoury GY, Abu-Zahra KW, Berbaum KS (2006) Interobserver agreement for Letournel acetabular fracture classification with multidetector CT: are standard Judet radiographs necessary? Radiology 241:386–391
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Prasartritha, T., Chaivanichsiri, P. The study of broken quadrilateral surface in fractures of the acetabulum. International Orthopaedics (SICOT) 37, 1127–1134 (2013). https://doi.org/10.1007/s00264-013-1845-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-013-1845-1