
Abstract
Purpose
We investigated the contact pressure and area of the patellofemoral joint both before and after different meniscectomies to provide a biomechanical basis for selecting meniscectomy and its clinical application for meniscus injuries.
Methods
Six fresh cadaveric knees were used in the study. Using Staubli robots and an ultra-low-min-type pressure-sensitive tablet, changes in contact area and stress in the patellofemoral joint were measured at various flexion angles following different parts and degrees of meniscectomy.
Results
The patellofemoral contact area enlarged with the increase of knee flexion angle. From the values obtained from contact areas and average contact pressure of the patellofemoral joint, we found no significant difference between partial meniscectomy and intact knees, but a significant difference was found between total meniscectomy and intact knees. The contact area after lateral meniscectomy was statistically less than that of intact knees. The mean patellofemoral contact pressure after lateral meniscectomy was larger than in intact knees at each angle of flexion. No significant difference in contact area was observed between intact knees and medial meniscectomy. The average patellofemoral contact pressure after medial meniscectomy was larger than in intact knees from 0° ~ 30° of knee flexion, and no significant differences were found between intact knees and medial meniscectomy while knee bending from 60° to 90°.
Conclusions
Different meniscectomies result in high contact pressure or disordered distribution of contact pressure, which may be the cause of postoperative patellofemoral degenerative arthrosis.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Stress change at articular surfaces has been clinically and experimentally confirmed to be the key reason for knee osteoarthritis after meniscectomy. Other factors contributing to degenerative changes include knee stability and alignment. In in vitro studies, a 350% increase in contact forces has been shown, simply due to removal of 16–34% of the meniscal tissue [1]. In clinical practice, numerous studies have documented that the progressive degenerative changes often occur in meniscus-deficient knees. The degree of degenerative change is directly proportional to the amount of meniscus removed [2]. Generally, degenerative changes following partial meniscectomy progress less rapidly than following total meniscectomy, and more rapidly in the lateral compartment following lateral meniscectomy [1]. Investigating cartilage stress is technically challenging, especially in testing cartilage stress of knee joints following various meniscectomies. As the knee joint is tricompartmental [patellofemoral joint (PFJ) and medial and lateral tibiofemoral joint (TFJ)] [3, 4], different meniscal deficiency at various flexion angles of knee joints may result in different stress changes at the PFJ and TFJ. In addition, many factors influence cartilage stress, including joint contact force, material properties of the tissue, geometry of articular surfaces and cartilage thickness. Previous researchers have calculated average PFJ stress by estimating the joint contact force and dividing this by a contact area measured with magnetic resonance imaging (MRI). This method has been used to illustrate increased average joint stress in patients with patellofemoral pain [3].
In this study, by using 12 fresh knee specimens from six cadavers, Staubli robots and an ultra-low-min-type pressure-sensitive tablet, we present a new biomechanical method to evaluate changes in contact area and stress in the PFJ at various flexion angles following different parts and degrees of meniscectomy. This is useful to illustrate the mechanism of patellofemoral arthritis following various parts and degrees of meniscectomy and provides theoretical evidence for selection of meniscectomy in the treatment of meniscal injuries or other meniscal diseases.
Materials and methods
Preparation of specimens
All six fresh cadavers used for this study were adults (male or female) from the Anatomy Department of Guangzhou Medical College, with the age range from 25 to 50 years. Knee joints with congenital malformation, fracture or tumour were excluded by radiography. All 12 knee joints were harvested 30 cm below and above the knee-joint line. Cutaneous and subcutaneous tissues around knee joints were removed, and complete surrounding tissue of the knee, quadriceps tendon and iliotibial tract were preserved. The prepared specimens were wrapped in saline-soaked gauze, stored at −20°C and defrosted at 20°C 12 hours before the day of testing. Twelve knee joints were randomly assigned into two groups: control (group A) and experimental (B, C, D, E, F). Group A consisted of four intact knee joints; group B, four knee joints with the anterior horn of medial meniscectomy; group C, four knee joints with the posterior horn of medial meniscectomy; group D, four knee joints with the anterior horn of lateral meniscectomy; group E, four knee joints with the medial meniscectomy; group F, four knee joints with the lateral meniscectomy. (group C was made from group A; group E from group B; group F from group D.)
Mechanical test
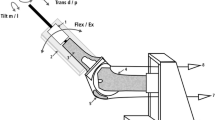
The tibiofibular bone was fixed 2 cm below the TFJ plane with a cortical bone screw (315 mm long and 24 mm diameter) to maintain the normal tension of the lateral collateral ligament and then fixed to the table with a steel clamp in a vertical and neutral position in both frontal and sagittal planes; the femur was held by a Staubli arm with a clamp. The ends of the vastus medialis muscle, vastus lateralis muscle, rectus femoris and vastus intermedius were clamped by three steel clamps (810 cm × 310 cm × 110 cm; rectus femoris and vastus intermedius muscles were fixed with a clamp) and were respectively attached to three steel cables in the same direction as their muscles, whereas the iliotibial tract was held by a clamp (610 cm × 215 cm × 110 cm ) connected to another steel cable(Fig. 1).

Steel clamps held the ends of vastus medialis, vastus lateralis, rectus femoris and vastus intermedius muscles and the iliotibial tract and were respectively attached to steel cables in the same direction as the muscles
Forces of 27 N, 67 N, 98 N and 111 N were respectively loaded on the iliotibial tract and vastus medialis, vastus lateralis, rectus femoris and vastus intermedius muscles with the steel cables after adjusting the axis of flexion and extension of the specimen to coincide with the loading rotation centre of the testing device. In the load mode, the knee specimen was passively flexed and extended with preloading five times, with an interval of ten minutes. Tests were carried out with the knee flexed at 0°, 10°, 20°, 30°, 40°, 60° and 90°, respectively. The ultra-low-min-type pressure-sensitive tablets (Fujitsu Corporation, Japan) were inserted into the PFJ via a small incision in the patellar bursa when the knee specimens were passively flexed and maintained at a target angle in the unload mode, and then the contact area and average stress were measured after two minutes of continuous loading and tested three times at each target angle (Fig. 2).

Knee-test model of the multiplane load based on the robot. Activity of a knee specimen was simulated for testing using the Staubli robotic/UFS testing system
Statistical analyses
Software package SPSS version 12.0 was used for analysis. Mean contact area or mean pressure on the PFJ among groups under different flexion angles were analysed statistically using analysis of variance (ANOVA) after the homogeneity of variance test. P < 0.05 was considered statistically significant.
Results
-
1.
Test results of mean contact area on the PFJ among groups under different flexion angles were as follows (Table.1):
Table 1 Comparison of mean contact area on the patellofemoral joint among groups under different flexion angle [mean standard deviation (SD), cm2] -
(a)
Mean contact area on the PFJ among groups of partial or total excision of lateral or medial meniscus was significantly different.
-
(b)
There was no significant difference among the mean contact area on the PFJ with different parts of meniscal resection.
-
(a)
-
2.
ANOVA on mean contact area of the PFJ under different angles is shown in Table 2.
Table 2 Analysis of variance of average contact area on the patellofemoral joint -
(a)
Mean contact area of the PFJ in different resection statuses was significantly different.
-
(b)
Mean contact area of the PFJ under different flexion angles was significantly different.
-
(a)
-
3.
Comparison and statistical analysis of mean pressure on the PFJ among groups under different flexion angles are shown in Table 3. Statistically significant difference of mean pressure on the PFJ was found among groups with flexion at 0°, 10°, 20°, 30°, 40°, 60° and 90° .
Table 3 Comparison of average pressure on the patellofemoral joint among groups under different flexion angles [mean standard deviation (SD), Mpa] -
4.
Analysis of variance of mean pressure efficiency on the PFJ under different flexion angles and resection status are shown in Table 4.
Table 4 Snalysis of variance of average pressure on the patellofemoral joint -
(a)
Mean contact area of the PFJ in different resection statuses was significantly different.
-
(b)
Mean contact area of the PFJ under different flexion angles was significantly different.
-
(a)
Discussion
-
1.
Robot in biomechanical study of knees
The challenging task of biomechanical tests on knee specimens is how to simulate knee action and loading status properly to understand the real stress state of the human knee joint during action in the physiological or pathological state in vivo. With continual advancement, several robots have been used by Chinese and Western scholars for this challenging task, and good results were obtained from properly simulating human knee activity [5–8]. In our experiment, we used the Staubli robotic/UFS testing system, a 6-DOF (degress of freedom) robotic manipulator, to simulate the 3D activity of the human knee joint in a force–displacement control mode. This robotic testing system, with both control and measurement function, provides a high-precision measurement of both force (power and torque) and displacement (linear displacement and rotation angle) and avoids errors of respective measurement of force and displacement that occurred in previous studies.
-
2.
Loading selection
Loading model of biomechanical test in human knee joints remains controversial. Powers et al. [9] indicated that multiplanar loading was better than axial loading in stimulating movement of the PFJ. Wickiewicz et al. [10] suggested that loading was closely related to the cross-sectional area of corresponding muscles, and the greater the cross-sectional area, the larger the loading. In this test, following Powers’s biomechanical testing model of human knee joints, we clamped the ends of vastus medialis, vastus lateralis, rectus femoris and vastus intermedius muscles and the iliotibial tract along their fibre direction and loaded forces of 27 N, 67 N, 98 N and 111 N, respectively, on the iliotibial tract and vastus medialis, vastus lateralis, rectus femoris and vastus intermedius using steel cables, according to Wickiewicz et al.’s experiments [10].
-
3.
Correlation between the osteoarthritis of the PFJ and various menisectomies of knee joints
The change trend of contact area of the PFJ after various meniscectomies was similar to that of normal PFJs. Usually, the contact area of the PFJ gradually increases while the TJ flexes from 0° to 90°(Fig. 3). The contact area of the PFJ with total lateral menisectomy was smaller and its mean stress was greater than that of normal the PFJ at any flexed angle.

Contact area at the patellofemoral joint (PFJ) of normal knee and the knee joint with anterior horn resection of the lateral meniscus or total lateral menisectomy
Usually, the valgus angle is about 10° to 15° at the normal TFJ, and the tibial tubercle is located laterally to the long axis of the femur and lateral quadriceps, so the patella always tends towards lateral dislocation. The valgus degree is increased after lateral menisectomy, which results in a Q-angle increase and an lateral relocation of the patella. As a result, stress distribution is excessively concentrated on the lateral PFJ and leads to PFJ osteoarthritis characterised by cartilage wear, softening, cracking and loss. No statistically significant difference between the contact area at the PFJ of normal knee joints and knee joints with total medial menisectomy was observed (Fig. 4). The mean stress was greater at the PFJ with total medial menisectomy than at the normal PFJ in the flexed angle from 0° to 30°. Schutzer et al. [11] proposed that most of the abnormal patellar tracks emerged at the PFJ within the flexed angle from 0° to 30°, and they believed that the PFJ would show normal performance of knee flexing, patella gradually sliding into the femoral condyle concave and ligament tightening, so that subtle abnormalities of the PFJ can be ignored. The severity of genu varum is increased after total medial meniscectomy, which leads to stress concentrating on the medial PFJ, followed by patellofemoral osteoarthritis characterised by cartilage wear and degeneration. There was also no statistically significant difference in the contact area or mean stress at the PFJ between normal knee joints and knee joints following removal of the anterior or posterior horn of the medial meniscus or the anterior horn of the lateral meniscus. Patellofemoral arthritis occurred after partial excision of the meniscus reached 21% clinically [12]. By experimentally comparing the colouring site of pressure-sensitive tablets inserted into the PFJ before and after partial meniscectomy, we found that the contact region of the PFJ changed in the flexed angle from 0° to 40°, indicating a “wrong grid phenomenon” arose in the PFJ. Mow et al. [13] reported that the patellar cartilage is a two-phase material, with not only a freeable and liquid mobile phase, but also with a porous, permeable, fibre-reinforced solid phase, which creates its biomechanical properties of resistance to tension, compression and shear. The local stress concentration at the articular cartilage destroys the internal molecules and microstructures of the cartilage collagen and matrix proteins, which leads to cartilage surface injury and softening. Although the stress was far less than the material’s ultimate strength, arthritic cartilage could not prevent fatigue and wear from the accumulation of minor damage caused by repeated pressure.

Contact area at the patellofemoral joint (PFJ) of a normal knee joint, and the knee joint with posterior horn resection of the medial meniscus or total medial menisectomy
In conclusion, our experiment expounded on the fact that osteoarthritis of the PFJ after meniscectomy was closely related to the higher or lower or uneven stress in the PFJ with total lateral or medial meniscectomy or partial meniscectomy.
References
Cole BJ, Cartwe AT, Rodeo SA (2002) Allograft Meniscal Transplantation Background, Techniques, and results. J Bone Joint Surg Br 84:1235–1250
Cox JS, Nye CE, Schaefer WW, et al. (1975) The degenerative effects of partial and total resection of the medial meniscus in dogs' knees. Clin Orthop Relat Res 178–183
Hinman RS, Crossley KM (2007) Patellofemoral joint osteoarthritis: an important subgroup of knee osteoarthritis. Rheumatology (Oxford) 46:1057–1062
Kalichman L, Zhang Y, Niu J et al (2007) The association between patellar alignment and patellofemoral joint osteoarthritis features—an MRI study. Rheumatology 46:1303–1308
Li G, Papannagari R, DeFrate LE et al (2006) Comparison of the ACL and ACL graft forces before and after ACL reconstruction: an in-vitro robotic investigation. Acta Orthop 77:267–274
Li G, Papannagari R, DeFrate LE et al (2007) The effects of ACL deficiency on mediolateral translation and varus-valgus rotation. Acta Orthop 78:355–360
Tang Z, Sun ZQ, Zhou CG (2007) Reference trajectory generation for 3-dimensionalwalking of a humanoid robot. Tsinghua Sci Technol 12:577–584
Ihn JC, Kim SJ, Park IH (1993) In vitro study of contact area and pressure distribution in the human knee after partial and total meniscectomy. Int Orthop 17:214–218
Powers CM, Lilley JC, Lee T (1998) The effects of axial and multi-plane loading of the extensor mechanism on the patellofemoral joint. Clin Biomech 13:616–624
Wickiewitz TL, Roy RR, Powell P et al (1983) Muscle architecture of the human lower limb. Clin Orthop Relat Res 179:275–283
Schutzer SF, Ramsby GR, Fulkerson JP (1986) The evaluation of patellofemoral pain using computerized tomography: a p reliminary study. Clin Orthop Relat Res 204:286–293
Englund M, Lohmander LS (2005) Patellofemoral osteoarthritis coexistent with tibiofemoral osteoarthritis in a meniscectomy population. Ann Rheum Dis 64:1721–1726
Mow VC, Ratcliffe A, Poole AR (1992) Cartilage and diarthrodial joints as paradigms for hierarchical materials and structures. Biomaterials 13:67–69
Financial disclosure
The authors gratefully acknowledge the National Natural Science Foundation of China (30570458) for the financial support of this research project.
Conflict of interest
None of the authors have any financial interest in any products, devices or drugs used in this study. There is no conflict of interest related to any commercial association or financial relationship (consultancy, stock ownership, equity interest, patent licensing arrangements or payments for conducting or publicising the study contained in the manuscript).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bai, B., Shun, H., Yin, Z.X. et al. Changes of contact pressure and area in patellofemoral joint after different meniscectomies. International Orthopaedics (SICOT) 36, 987–991 (2012). https://doi.org/10.1007/s00264-011-1450-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-011-1450-0