
Abstract
Selection of suitable tumor-associated antigens is a major challenge in the development of effective cancer vaccines. Intratumoral (i.t.) immunotherapy empowers the immune system to mount T cell responses against tumor-associated antigens which are most immunogenic. To mediate systemic tumor regression, i.t. immunotherapy must generate systemic T cell responses that can target distant metastases beyond the initially treated tumor mass. Now that promising preclinical results and some initial success in clinical trials have been obtained, we here review i.t. immunotherapy-related preclinical and clinical studies, their mechanisms of action and future prospects.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cancer immunotherapy is based on the recognition of tumor-associated mutant or non-mutant antigens (peptides) on cancer cells by the patient’s T cells. Cancer vaccines have successfully increased the number and activity of T cells that recognize tumor-associated antigens (TAAs) in many cases, but robust clinical responses remain anecdotal [1]. In contrast, US Food and Drug Administration-approved immunotherapies such as high-dose interleukin (IL)-2, interferon (IFN)-α, anti-CTLA-4 (cytotoxic T lymphocyte antigen-4) monoclonal antibodies and anti-PD-L1 (programmed death-ligand) therapies all appear to activate and/or expand tumor-specific T cells of largely unknown antigen specificity. This process allows the immune system to “decide” which antigen to target and may prove particularly fruitful as an approach to cancer immunotherapy. However, this approach requires the delivery of appropriate signals that convert immune responses from being ineffective to capable of rejecting established tumors. Using the tumor itself as a vaccine by introducing an immunomodulator or adjuvant can activate innate immunity and lead toward immunizing patients against shared (usually “self”) or patient-specific, mutated antigens. Besides generating tumor-specific immunity through T cell priming, intratumoral (i.t.) immunotherapy can also target the tumor by affecting innate immune cells like myeloid-derived suppressor cells (MDSC) and M2 macrophages, for example by polarizing them into tumor-suppressive phenotypes such as M1 macrophages [2, 3]. This modification of the tumor microenvironment and generation of systemic tumor-specific immunity by i.t. immunotherapy is not only useful to destroy the injected tumor but also suppresses distant metastasis. Intratumoral immunotherapy has been attempted for many years to treat solid tumors, especially melanoma due to its easily accessible cutaneous nature and high immunogenicity compared to most other malignancies. The majority of data on i.t. immunotherapy therefore involve melanoma. Here, we review various i.t. immunotherapy strategies to treat metastatic melanoma.
I.t. immunotherapy with bacteria
William B. Coley observed that patients with bacterial infections sometimes underwent spontaneous remissions of their cancers. Based on this observation, in 1891, he began treating bone sarcoma by injecting virus or bacteria into the tumors, resulting in some remarkable cures [4]. Since then, many bacteria and bacterial products have been used to activate the immune system to kill cancer cells. Activation of the toll-like receptor (TLR) pathway of immune cells by bacterial cell walls and their nucleic acids makes some bacteria useful in cancer treatment. I.t. bacillus Calmette–Guerin (BCG) alone and in combination with chemotherapy and other immunotherapies has been used to treat melanoma [5–8]. This bacterial therapy provides immunostimulatory DNA and activates the TLR9-MyD88 pathway [9], which leads to activation of macrophages and dendritic cells (DCs) and the production of various cytokines [9, 10]. These activated innate immune cells can also prime tumor-specific T cells against various TAAs and generate anti-tumor immunity. Recombinant BCG (rBCG 3A) has anti-tumor properties equivalent to those of wild-type BCG, but is a safer alternative for patients, because it does not contain infectious bacteria [11]. Udagawa et al. [12] reported that intratumoral administration of DCs stimulated with the BCG cell wall skeleton (BCG-CWS) suppressed the growth of not only the cryoablative tumors into which they were injected but also tumors at distant sites, which suggests that i.t. BCG can be an effective treatment for metastasis.
I.t. injection of the Salmonella enterica serovar typhimurium vaccine has also been shown to produce anti-tumor activity through transformation of MDSCs into tumor necrosis factor (TNF)-alpha-secreting neutrophils, reducing the generation of regulatory T (Treg) cells and increasing cytotoxic T cell infiltration [13]. This therapy is an example of i.t. therapy that not only generates tumor-specific T cells but also changes the tumor microenvironment from tumor promoting to tumor suppressive.
I.t. administration of attenuated Toxoplasma gondii parasites treated B16.F10 melanoma because it stimulated systemic anti-tumor immunity and tumor-specific memory CD8+ T cells [14, 15]. The results of these studies suggest that activation of tumor-associated innate immune cells by attenuated bacteria or parasites is a promising, safe and inexpensive approach to treat metastatic melanoma. However, efficacy is largely anecdotal at this point in time.
I.t. immunotherapy with oncolytic viruses
Tumor cell killing by genetically engineered and naturally occurring oncolytic viruses is another approach for cancer treatment that has been studied for decades [16]. These viruses selectively replicate in tumor cells because viral receptors are overexpressed on the surface of those cells or because specific anti-viral pathways, such as the type I IFN pathway, are disrupted in tumor cells or tumor stromal cells. Viruses can also be genetically modified for selective homing to tumor cells, for example, by genetic alterations in viral capsids or envelops, generating viruses that specifically recognize only tumor-associated surface markers and infect tumor cells [17]. Many DNA and RNA viruses have been used in melanoma treatment, including Newcastle disease virus (NDV) [18], adenovirus [19], herpes simplex virus [20], influenza virus [21], coxsackievirus [22], reovirus [23], vesicular stomatitis virus (VSV) [24], parvovirus [25], vaccinia virus [26, 27], measles virus [28] and myxoma virus [29].
Oncolytic viruses typically infect only a fraction of all tumor cells in the injected tumor mass. However, these viruses induce anti-tumor immunity through antigen release from lysed tumor cells, in combination with virus-induced local innate immune activation. As a result, much of the eventual cancer cell death is mediated by the host’s adaptive immune system. It has been reported that most oncolytic viruses trigger innate immune responses because they produce factors that can specifically bind to toll-like receptors (TLR) on host cells resulting in signaling through the MyD88 pathway [24, 30, 31]. The resulting activation of the IRF and NF-kB pathways causes DCs to produce large amounts of cytokines including type I IFNs [32, 33], which promotes the activation and tumor infiltration of tumor-specific T cells [34, 35]. Wild-type coxsackievirus A21 is a common cold virus that selectively infects and kills melanoma cells through its interaction with intercellular adhesion molecule (ICAM-1) and decay accelerating factor (DAF). These molecules are overexpressed on the surface of malignant melanoma cells compared to the surrounding benign tissue [36]. ICAM-1 is also recognized as a viral attachment receptor for many enteroviruses including CVA13, CVA15 and CVA18 [22]. Phase I/II trials using oncolytic A21 coxsackievirus (Cavatak) have been conducted and found effective and safe [37].
To further enhance the activation of innate, and subsequently adaptive immunity, many oncolytic viruses are modified to express immunostimulatory molecules. A recent study used i.t. therapy with a genetically modified adenovirus, encoding CD40 ligand (Ad-CD40L) in murine melanoma, resulting in tumor regression that was associated with specific T cell responses against TAAs, including the melanocyte differentiation antigen, TRP-2 and the model antigen, chicken Ovalbumin [38]. In another study, the novel oncolytic adenovirus Ad5/3-hTERT-E1A-hCD40L, which includes chimeric Ad5/3 capsid for enhanced tumor transduction, a human telomerase reverse transcriptase (hTERT) promoter for tumor selectivity, and human CD40L for increased efficacy, caused tumor destruction and generated a significantly stronger tumor-specific CD8 T cell response than wild-type adenovirus [39]. Similar to Ad-CD40L, i.t. immunotherapy with an adenovirus vector expressing OX40L (AdOX40L) generated anti-tumor immunity mediated by cytotoxic CD8 T lymphocytes (CTLs) [40]. Furthermore, an adenoviral vector expressing siRNA against the mouse IL-17A gene (Ad-si-IL-17) significantly inhibited both MC38 and B16 tumor growth and induced a Th1-dominant environment, which selectively eliminated MDSCs and Tregs at tumor sites but not in the spleen [41].
A recent study compared i.t. lipopolysaccharide (LPS) plus i.t. VSV to i.t. LPS plus i.v. VSV. Administration of both drugs i.t. synergized well and generated a profound anti-tumor immune response, whereas the combination of i.t. LPS with systemically delivered VSV resulted in rapid morbidity and mortality in the majority of mice [42]. This study highlights the benefits of i.t. over systemic treatment in terms of reduced toxicity. Another recent study showed that combination therapy with i.t. NDV and systemic CTLA-4 blockade regressed distant tumors and developed long-term CD8 T cells memory against poorly immunogenic B16 tumors. The therapeutic effect was dependent on CD8+ cells, natural killer cells and type I IFN [43].
Clinical trials of i.t. immunotherapy with oncolytic viruses
Mastrangelo et al. [44] used i.t. vaccinia virus encoding recombinant granulocyte–macrophage colony-stimulating factor (GM-CSF) and found it to be safe and effective in patients with metastatic melanoma. Similarly, in a phase II trial of talimogene laherparepvec (T-VEC), an oncolytic herpes simplex virus encoding GM-CSF, the virus was administered i.t. to patients with metastatic melanoma and caused complete regression of injected and uninjected lesions in eight of 50 patients [45] (Table 1). T-VEC also showed improvement in durable response rate (DRR) and improvement in overall survival approached statistical significance in a Phase III trial when compared to systemic GM-CSF control treatment [46]. Phase I/II trial based on intratumoral injections of adenovirus-IL-2 (TG1024) have been conducted on patients with melanoma. The virus induced pronounced inflammation in the treated lesions with predominant CD8+, TIA+ (a granule-associated protein of cytotoxic T cells) lymphocytic infiltrates [47]. In a phase I clinical trial, i.t. injections of adenovirus-delivered mda-7/IL-24 (Ad.mda-7) proved safe, elicited tumor-suppressive and immune-enhancing processes including Th1 cytokines production and CD8 T cells activation and provided clinically significant anti-tumor activity [48]. Herpes simplex virus (HSV) have also been used to treat mouse and human glioblastoma and found to be a promising treatment for patients with glioblastoma [49].
Naturally occurring or genetically modified oncolytic viruses are thus promising agents for the treatment of melanoma. The host-induced primary immune response against the virally infected tumor cells causes limited tumor destruction and cytokine production, and APC are activated, take up tumor antigen from killed tumor cells and prime tumor-specific CD8 T cells that may ultimately cause systemic anti-tumor immunity.
I.t. immunotherapy with synthetic immunoagonists
Synthetic TLR agonists can stimulate the TLR-MyD88 pathway, activate innate immune cells and lead to tumor-specific adaptive immunity. Combination therapy with i.t. poly I:C (a TLR-3 agonist) and CpG (a TLR-9 agonist) with adoptive T cell transfer eradicated established melanoma through an IFN-gamma-dependent mechanism [50]. We and others have shown that i.t. and peritumoral CpG administration routes are superior to intravenous and subcutaneous routes for the activation of innate immune cells leading to induction of tumor-specific CTLs and long-lasting tumor protection [51–53]. It has also been reported that TLR-9 expression on plasmacytoid DC is critical for the therapeutic effect of CpG [53]. A recent preclinical study showed that combination therapy with anti-CTLA-4 and anti-OX40 antibodies together with CpG was able to modify the tumor microenvironment by depleting tumor-infiltrating Tregs; this increased the therapeutic efficacy of CpG and generated a systemic anti-tumor immune response that eradicated distant tumors, including in the brain [54]. Shirota et al. reported that i.t. administration of CpG oligodeoxynucleotides (ODNs) reduced the immunosuppressive activity of monocytic MDSCs (CD11b+Ly6G−Ly6Chi) which differentiated into tumoricidal macrophages (CD11b+F4/80+Ly6Chi). Monocytic MDSCs are present in high numbers in many tumors and suppress anti-tumor T cell function; therefore, switching the phenotypes of these cells from tumor promoting to tumor suppressing may enhance anti-tumor immunity. These studies provide insight into a novel mechanism by which CpG ODNs contribute to tumor regression and also provide an example of how local treatment by a TLR agonist can convert a tumor-promoting microenvironment to a tumor-suppressing one [55]. I.t. injection of polyguanosine ODNs boosted anti-tumor immunity mediated through direct phosphorylation of Lck in CD8 T cells, resulting in expansion of CD8 T cells and IL-2 production [56].
I.t. injection of plasmid DNA encoding CD40L (pSP-D-CD40L) with TLR-9 and TLR-3 agonists (CpG and poly I:C) changed the tumor microenvironment by increasing the number of cytotoxic CD8+ T cells and decreasing the number of DCs (it may due to the activation and migration of DCs to tumor-draining lymph nodes): These changes slowed tumor growth and prolonged mouse survival [57]. It has been shown that i.t. treatment with GVAX (GM-CSF secreting whole-cell tumor cell vaccine) plus LPS (TLR-4 agonist) was more efficient at generating anti-tumor responses than GVAX alone [58]. An i.t. TLR-2 agonist switched mast cell phenotypes from tumor promoting to tumor inhibiting and secreted cytokines IL-6 from activated mast cells causing B16 melanoma regression [59]. These studies suggest that direct activation of the tumor-infiltrating TLR+ innate immune cells by TLR agonists induces effective innate immune response and also prime tumor-specific CD8 T cell responses that could be long lasting and systemic if combined with T cells activating drug.
The synthetic TLR-7 agonist imiquimod showed synergy with live recombinant listeria vaccine and significantly enhanced its anti-tumor effects against murine melanoma [60]; similarly, this TLR-7 agonist also enhanced the anti-melanoma effects of IL-2 [61]. Recently, two studies [62, 63] showed that topical treatment with imiquimod suppressed tumor growth by converting pDCs into granzyme B-expressing, tumor-killing effector cells. In addition, we found that i.t. treatment with a tissue-retained, injectable form of a TLR-7/8 agonist, 3M-052, suppressed melanoma growth through T and B cell-dependent mechanisms. It also stimulated tumor-associated macrophages and polarized them from M2 to M1 phenotypes, and these macrophages contributed to the anti-tumor activity [3].
CD137 or 4-1BB is a member of the TNF receptor family that is expressed on activated T cells and crosslinking of CD137 with its ligand enhances T cell proliferation and cytokine production. It has been shown that CD137 agonist antibodies enhance the cytolytic function and proliferation of CD8 T cells and leads to regression of established tumors [64] I.t. delivery of liposome-coupled anti-CD137 plus IL-2-Fc fusion protein appeared very effective against B16 melanoma and did not cause toxicity [65]. I.t. SFV-IL-12 (Semliki Forest virus encoding IL-12) and systemic anti-CD137 agonist antibodies therapy generated robust anti-tumor immunity against B16 melanomas (B16-OVA and B16.F10) and TC-1 lung carcinomas. I.t. injection of SFV-IL-12 induced strong expression of CD137 on CD8+ T lymphocytes, providing targets for the action of the CD137 agonist antibody [66]. Recently, Marabelle et al. described that pattern recognition receptor agonists including TLR agonists and immunostimulatory monoclonal antibodies like anti-CD137 and anti-CTLA-4 showed synergistic effect when delivered intratumorally and stimulated the tumor-infiltrating leukocytes. This suggests that i.t. immunotherapy would be a better option to generate systemic anti-tumor immune response with lower toxicity than after systemic administration [67, 68]. Another report also compared local delivery of slow release formulation of anti-CTLA-4 or anti-CD40 near to tumor lesion with systemic therapy and found that controlled local delivery of immunomodulating antibodies generates systemic anti-tumor CD8 T cells immunity but minimal toxicity compared to systemic treatment [69]. Interestingly, peritumoral route of treatment initiated different types of immune response than intratumoral treatment, likely because of differences in the immune environment of tumors versus normal tissues such as skin. Therefore, it is important to understand which immune cells initiate and modulate effective adaptive anti-tumor immune response.
I.t. immunotherapy by synthetic STING agonist
STING (stimulator of interferon genes) is a transmembrane containing protein that is localized in the endoplasmic reticulum (ER) of numerous cell types such as macrophages, dendritic cells, endothelial and epithelial cells [70]. It induces type I interferon production through recognition of pathogen or tumor-derived cytosolic DNA metabolites [71, 72]. It has been shown to activate downstream transcription factors STAT6 and IRF3 through TBK1, resulting in anti-viral and innate immune responses against intracellular pathogens [73]. CD8α+DCs and type I interferons are required for spontaneous T cell priming in growing tumors [74], and a major defect in both type I IFN induction and T cell priming was observed in STING−/− mice, as well in mice lacking the downstream transcription factor IRF3 [75]. Presence of tumor cell DNA in host APCs correlated with STING pathway activation and IFN-β production [76].
DMXAA is a known strong agonist of the mouse STING pathway, and i.t. injection of DMXAA-induced tumor antigen-specific CD8+ T cells had robust anti-tumor activity via a mechanism that was dependent on the host STING [77]. Intratumoral administration of a different STING agonist (cyclic diguanylate monophosphate; c-di-GMP) improved the survival of glioma-bearing mice associated with enhanced type I IFN signaling and T cell migration into the brain [78].
Thus, activation of STING pathway by naturally occurring tumor DNA is the main source of type I interferon production in tumor, which initiates tumor-specific immunity at some extent, and that immune response can be enhanced multifold by direct i.t. delivery of synthetic STING agonists and can have profound therapeutic efficacy. However, all known murine STING agonists do not bind to human STING which may limit their use clinically. New generations of STING agonist are under development that binds murine as well as all known human STING variants.
Clinical trials of i.t. immunotherapy with synthetic immunoagonists
Food and Drug Administration-approved synthetic TLR7 agonist imiquimod is a cream formulation for the treatment of cutaneous basal cell carcinoma, actinic keratosis and genital warts, and has limited activity against cutaneous melanoma and breast tumors [79–82]. The cream formulation of imiquimod limits its application for deep, non-cutaneous tumors and systemic administration of TLR agonists is limited by severe toxicity, including cytokine storm [83]. Thus, the newly developed injectable, lipid-modified TLR7/8 dual agonist 3M-052 that is shown to have therapeutic efficacy against mice melanoma, could be a better option for future clinical trials of i.t. therapy of melanoma [3, 84].
A phase I trial of i.t. treatment with a TLR-9 agonist, PF-3512676, showed local tumor regression in patients with basal cell carcinoma (one complete regression and four partial regressions out of five treated patients) and metastatic melanoma (one complete regression out of five treated patients). All patient’s post-treatment biopsies showed moderate to abundant cellular infiltrates of lymphocytes in injected and uninjected lesions [85]. Carpentier et al. [86] conducted a phase II trial to test the efficacy of i.t. CpG ODNs in patients with recurrent glioblastoma after radiotherapy and chemotherapy; the median overall survival was 28 weeks; however, this trial did not meet the targeted progression-free survival benefit in patients with recurrent GBM. Recently, Salazar et al. [87] treated a patient with facial embryonal rhabdomyosarcoma by i.t. and intramuscular injections of a stabilized dsRNA viral mimic, polyinosinic-polycytidylic acid-polylysine-carboxymethyl cellulose (poly-ICLC, Hiltonol) and reported tumor regression with extended survival. Thus, there is some evidence of clinical success with i.t. TLR agonists in specific settings, particularly superficial cutaneous disease.
TLR agonists are very promising adjuvants for i.t. immunotherapy because most tumor-associated innate immune cells express TLRs and can easily be activated in response to these agonists. Some of these cells are able to switch their phenotypes from immunosuppressive to immune enhancing and kill tumor cells directly and/or prime tumor-specific T cells. If these tumor-specific T cells receive further stimulation through TNF receptor super family (TNFRSF) members such as 4-1BB or OX40, which keeps them in the activated stage and enhances their functions, the result can be a strong, long-lasting, systemic anti-tumor immunity. Therefore, combination therapy with TLR agonists and 4-1BB/OX40 agonists may be a promising strategy to treat established tumors.
I.t. immunotherapy with cytokines
I.t. administration of cytokines such as IL-2, IL-21, IFN-alpha/beta and IL-12 can also generate anti-tumor immunity and suppress tumor growth. Combination therapy with i.t. IL-12 and systemic anti-CTLA-4 led to eradication of murine glioblastoma in mouse [88]. I.t. administration of IL-21 showed better treatment effect than subcutaneous injection and caused superior CD8 T cell proliferation [89]. I.t. delivery of plasmid DNA encoding IL-12 by in vivo electroporation induced systemic immunity that was able to kill both injected and uninjected, distant tumors without the systemic toxicity commonly observed after systemic administration of cytokine protein [90]. The combination of i.t. IL-12 with T cells redirected against vascular endothelial growth factor receptor-2 had therapeutic efficacy in mice with a variety of solid tumor types, including melanoma [91]. I.t. hu14.18-IL-2 showed better anti-tumor activity in mouse models compared with i.v. hu14.18-IL-2 [92]. I.t. DC-IFN-gamma efficiently induced cross-presentation of tumor antigens to specific CD8+ T cells and generated anti-tumor immunity against pre-established B16 melanoma [93]. Van der Jeught et al. [94] showed that i.t. administration of mRNA encoding a fusion protein consisting of interferon-β and the ectodomain of the transforming growth factor-β receptor II induced anti-tumor immunity in mice by enhancing the antigen-presenting capacity of dendritic cells and reducing the suppressive activity of myeloid-derived suppressor cells.
Clinical trials of i.t. immunotherapy with cytokines
In a clinical trial, i.t. administration of plasmid encoding IL-12 was found to be effective in melanoma. Two of nine patients showed stable disease, and one had a complete response. Patients, especially responders, generated antigen-specific immunity against MAGE-1 and MART-1 antigens [95]. L19-IL-2, an immunocytokine made up of the recombinant human antibody fragment L19 (specific to the alternatively spliced EDB domain of fibronectin, a well-characterized marker of tumor neo-vasculature) and of human IL-2, has shown therapeutic efficacy in animal cancer models. Twenty-five patients with stage IIIB/IIIC melanoma and cutaneous/subcutaneous injectable metastases were treated i.t. with L19-IL-2, resulting in complete response (CR) in 25 % of patients by modified immune-related response criteria (irRC) [96] (Table 1).
Overall, i.t. cytokine therapy is a rapid and effective method to generate tumor-specific adaptive immunity in several mouse models, with some evidence of efficacy in patients with melanoma.
I.t. immunotherapy with activated immune cells
Activated antigen-presenting cells are needed to prime tumor-specific T cells and develop long-lasting immunity. In this regard, many studies have been performed to determine the effectiveness of in vitro activated DCs in in vivo tumor killing. While most of these studies used antigen-loaded DCs as vaccines for subcutaneous, intravenous or intranodal delivery, some studies directly introduced DCs i.t. to promote uptake of tumor antigen and T cell priming. Okano et al. reported that i.t. delivery of Fas-inhibited allogeneic DCs had anti-tumor effects similar to those of autologous DCs, and this approach offers an alternative in patients where autologous DCs cannot be used. This study suggests that blocking the Fas–FasL interaction between allogeneic DC and host T cells may be an useful strategy to overcome the rejection response against alloantigens on the DCs [97]. We have shown that i.t. administration of TLR9-triggered pDCs induced robust anti-tumor immunity that resulted in regression of the treated tumor as well as distant tumors by natural killer cells and CD8 T cell-mediated mechanisms [98]. I.t. injection of immature DCs and IFN-gamma into malignant tumors in dogs produced anti-tumor immunity including four complete responses and two partial responses out of seven treated dogs [99]. In B16 melanoma, i.t. injection of poly I:C-treated DCs generated anti-tumor immunity and led to infiltration of TRP-2-specific IFN-gamma-producing CD8+ T cells [100].
Other i.t. immunotherapy
Recently, i.t. injections of recombinant heat-shock protein (Hsp)70 were used to treat malignant brain tumors in children; the therapy was safe but not highly effective (one of 12 children had a complete response, and one had a partial response). However, an increased number of Th1 T cells and decreased number of B and Treg cells were seen in the blood of all children in response to Hsp70 treatment [101], suggesting that locally injected Hsp70 may generate a systemic anti-tumor immune response that could be further enhanced with additional immunomodulators such as the T cell checkpoint blockade agents approved for the treatment of metastatic melanoma, anti-CTLA-4 (ipilimumab) and anti-PD-1 (pembrolizumab).
In a study of i.t. therapy in mice, injection of alpha-gal glycolipids into experimental melanomas induced CD8 T cell-mediated protective immunity that was not only effective against the treated tumor but also suppressed distant metastasis [102].
Allovectin (velimogene aliplasmid) is an immunotherapeutic drug for direct i.t. administration. It is a plasmid that encodes both major histocompatibility complex (MHC) class I heavy (HLA-B7) and light chains (β2-microglobulin) and i.t. administration of this plasmid stimulates both local and systemic anti-tumor immune responses [103]. Phase II and III trials were conducted using allovectin in 127 and 375 patients, respectively. However, in the phase III trial, allovectin failed to improve overall survival [37].
Sandin et al. [104] have suggested that local administration of anti-CTLA-4 monoclonal antibodies is a better option to treat pancreatic adenocarcinoma than systemic treatment because local treatment had similar treatment efficacy to systemic treatment and did not cause accumulation of Treg cells in secondary lymphoid organs. However, i.t. therapy of tumors at visceral sites such as the pancreas is more challenging than systemic therapy due to the need for image-guided i.t. administration, requiring specific equipment and expertise.
Perspectives
The induction of anti-tumor immunity by immune activation within tumors is an effective method to generate immune responses against multiple (self and non-self) tumor antigens and modify the tumor microenvironment. A great advantage is the possibility of producing “off-the-shelf” reagents that can be applied across patient populations and tumor types, since antigens do not need to be identified. This approach could therefore be a more rapid, broadly applied and cost-effective therapeutic option than personalized immunotherapy. However, care should be taken in choosing the specific i.t. immunotherapy method because strong immune activation results in the up-regulation of chemokines within a tumor and may cause an influx of immune cells only in treated tumors and a lack of immunity or cell killing in untreated tumors. At this time, a wealth of approaches is being tried, and it is as of yet unclear which of these are most potent in their ability to induce systemic anti-tumor immunity and therapeutic benefit. Therefore, well-designed preclinical studies should be conducted to observe the effect of a particular drug and its mechanisms of action in metastatic disease models and especially in clinical trials. Administration of a reproducible amount of therapeutic agent into tumors and immune-suppressive tumor environments can be challenging; however, i.t. immunotherapy could be safer than systemic treatment, with its local nature giving rise to fewer side-effects such as systemic tissue inflammation or cytokine storm. As an exciting prospect, i.t. therapy can enhance the effect of the FDA-approved checkpoint blockade therapeutics, anti-CTLA-4 and anti-PD-1, by promoting the generation of activated, tumor-specific T cells that can then become the targets for checkpoint blockade.
Conclusion
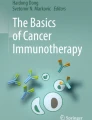
Many local tumor immunomodulation therapies to generate systemic anti-tumor immunity are emerging. The benefits of i.t. immunotherapy depend not only on the generation of tumor-specific immunity but also on changing the tumor microenvironment from immunosuppressive to immunostimulatory (Fig. 1). This approach holds great promise in combination with chemotherapy and systemic immunotherapies. Opportunities include (1) i.t. immunotherapy with adoptive T cell transfer, (2) i.t. oncolytic viruses encoding immunomodulatory molecules and (3) combination of i.t. immunoagonists with i.t. or systemic anti-CTLA-4 or anti-PD1/PD-L1 blockade. These synergistic combinations may provide a promising approach to generate systemic anti-tumor immunity for the treatment of metastatic melanoma with superior efficacy over single-agent approaches.

Activation of tumor-associated immune cells by i.t. immunotherapy generates strong local and systemic immunity: (i) i.t. delivery of immunoagonists, cytokines and other immune activating agents, (ii) activation of tumor-associated innate immune cells through toll-like receptor, CD40 or cytokine pathway leads to conversion of M2 macrophages, MDSC, DCs/pDCs and B cell to M1 macrophages, killer pDC/DC and B1 cells, respectively. (iii) These activated cells produce many cytokines or/and lytic molecules and kill tumor cells directly. (iv) They can also act as an antigen-presenting cells and (v) migrate to TDLN where they process and present tumor antigens to CD8 T cells to (vi) expand tumor-specific CD8 T cells and generate long-lasting tumor-specific immunity. (vii, viii, ix) Secondary co-stimulation or blocking of inhibitory pathway further activates and facilitates migration of these tumor-specific CD8 T cells to injected and uninjected tumor and cause tumor lysis
Abbreviations
- APC:
-
Antigen-presenting cells
- BCG:
-
Bacillus Calmette–Guerin
- CTLA-4:
-
Cytotoxic T lymphocyte antigen-4
- DCs:
-
Dendritic cells
- IFN:
-
Interferon
- IT:
-
Intratumoral
- MDSC:
-
Myeloid-derived suppressor cells
- NDV:
-
Newcastle disease virus
- ODNs:
-
Oligodeoxynucleotides
- PD-1:
-
Programmed death-1
- PD-L1:
-
Programmed death-ligand
- pDCs:
-
Plasmacytoid dendritic cells
- poly-ICLC:
-
Polyinosinic-polycytidylicacid-polylysine-carboxymethylcellulose
- TAAs:
-
Tumor-associated antigens
- TLR:
-
Toll-like receptor
References
Rosenberg SA, Yang JC, Restifo NP (2004) Cancer immunotherapy: moving beyond current vaccines. Nat Med 10:909–915. doi:10.1038/nm1100
van den Boorn JG, Hartmann G (2013) Turning tumors into vaccines: co-opting the innate immune system. Immunity 39:27–37. doi:10.1016/j.immuni.2013.07.011
Singh M, Khong H, Dai Z, Huang XF, Wargo JA, Cooper ZA, Vasilakos JP, Hwu P, Overwijk WW (2014) Effective innate and adaptive antimelanoma immunity through localized TLR7/8 activation. J Immunol 193:4722–4731. doi:10.4049/jimmunol.1401160
Nauts HC, Swift WE, Coley BL (1946) The treatment of malignant tumors by bacterial toxins as developed by the late William B. Coley, M.D., reviewed in the light of modern research. Cancer Res 6:205–216
Stewart JH, Levine EA (2011) Role of bacillus Calmette–Guerin in the treatment of advanced melanoma. Expert Rev Anticancer Ther 11:1671–1676. doi:10.1586/era.11.163
Kidner TB, Morton DL, Lee DJ, Hoban M, Foshag LJ, Turner RR, Faries MB (2012) Combined intralesional Bacille Calmette–Guerin (BCG) and topical imiquimod for in-transit melanoma. J Immunother 35:716–720. doi:10.1097/CJI.0b013e31827457bd
Bast RC Jr, Zbar B, Borsos T, Rapp HJ (1974) BCG and cancer. N Engl J Med 290:1458–1469. doi:10.1056/NEJM197406272902605
Paterson AH, Willans DJ, Jerry LM, Hanson J, McPherson TA (1984) Adjuvant BCG immunotherapy for malignant melanoma. Can Med Assoc J 131:744–748
Akazawa T, Masuda H, Saeki Y et al (2004) Adjuvant-mediated tumor regression and tumor-specific cytotoxic response are impaired in MyD88-deficient mice. Cancer Res 64:757–764
Freedman VH, Gorrell TE, Nathan CF, Copeland CS, Silverstein SC (1984) Bacillus Calmette–Guerin-activated murine macrophages kill syngeneic melanoma cells under strict anaerobic conditions. J Exp Med 160:94–107
Duda RB, Yang H, Dooley DD, Abu-Jawdeh G (1995) Recombinant BCG therapy suppresses melanoma tumor growth. Ann Surg Oncol 2:542–549
Udagawa M, Kudo-Saito C, Hasegawa G et al (2006) Enhancement of immunologic tumor regression by intratumoral administration of dendritic cells in combination with cryoablative tumor pretreatment and Bacillus Calmette–Guerin cell wall skeleton stimulation. Clin Cancer Res 12:7465–7475. doi:10.1158/1078-0432.CCR-06-1840
Hong EH, Chang SY, Lee BR, Pyun AR, Kim JW, Kweon MN, Ko HJ (2013) Intratumoral injection of attenuated Salmonella vaccine can induce tumor microenvironmental shift from immune suppressive to immunogenic. Vaccine 31:1377–1384. doi:10.1016/j.vaccine.2013.01.006
Fox BA, Sanders KL, Chen S, Bzik DJ (2013) Targeting tumors with nonreplicating Toxoplasma gondii uracil auxotroph vaccines. Trends Parasitol 29:431–437. doi:10.1016/j.pt.2013.07.001
Baird JR, Byrne KT, Lizotte PH et al (2013) Immune-mediated regression of established B16F10 melanoma by intratumoral injection of attenuated Toxoplasma gondii protects against rechallenge. J Immunol 190:469–478. doi:10.4049/jimmunol.1201209
Alemany R (2013) Viruses in cancer treatment. Clin Transl Oncol 15:182–188. doi:10.1007/s12094-012-0951-7
Ayala-Breton C, Barber GN, Russell SJ, Peng KW (2012) Retargeting vesicular stomatitis virus using measles virus envelope glycoproteins. Hum Gene Ther 23:484–491. doi:10.1089/hum.2011.146
Sinkovics JG, Horvath JC (2000) Newcastle disease virus (NDV): brief history of its oncolytic strains. J Clin Virol 16:1–15
Maass G, Bogedain C, Scheer U et al (1998) Recombinant adeno-associated virus for the generation of autologous, gene-modified tumor vaccines: evidence for a high transduction efficiency into primary epithelial cancer cells. Hum Gene Ther 9:1049–1059. doi:10.1089/hum.1998.9.7-1049
Russell SJ, Peng KW, Bell JC (2012) Oncolytic virotherapy. Nat Biotechnol 30:658–670. doi:10.1038/nbt.2287
van Rikxoort M, Michaelis M, Wolschek M, Muster T, Egorov A, Seipelt J, Doerr HW, Cinatl J Jr (2012) Oncolytic effects of a novel influenza A virus expressing interleukin-15 from the NS reading frame. PLoS ONE 7:e36506. doi:10.1371/journal.pone.0036506
Au GG, Beagley LG, Haley ES, Barry RD, Shafren DR (2011) Oncolysis of malignant human melanoma tumors by Coxsackieviruses A13, A15 and A18. Virol J. 8:22. doi:10.1186/1743-422X-8-22
Prestwich RJ, Errington F, Ilett EJ et al (2008) Tumor infection by oncolytic reovirus primes adaptive antitumor immunity. Clin Cancer Res 14:7358–7366. doi:10.1158/1078-0432.CCR-08-0831
Wongthida P, Diaz RM, Galivo F, Kottke T, Thompson J, Melcher A, Vile R (2011) VSV oncolytic virotherapy in the B16 model depends upon intact MyD88 signaling. Mol Ther 19:150–158. doi:10.1038/mt.2010.225
Moehler MH, Zeidler M, Wilsberg V, Cornelis JJ, Woelfel T, Rommelaere J, Galle PR, Heike M (2005) Parvovirus H-1-induced tumor cell death enhances human immune response in vitro via increased phagocytosis, maturation, and cross-presentation by dendritic cells. Hum Gene Ther 16:996–1005. doi:10.1089/hum.2005.16.996
Brun J, Mahoney DJ, Le Boeuf F, Lefebvre C, Sanaei CA, Falls T, McCart JA, Stojdl DF (2013) Oncolytic Vaccinia virus safely and effectively treats skin tumors in mouse models of xeroderma pigmentosum. Int J Cancer 132:726–731. doi:10.1002/ijc.27695
MacTavish H, Diallo JS, Huang B et al (2010) Enhancement of vaccinia virus based oncolysis with histone deacetylase inhibitors. PLoS ONE 5:e14462. doi:10.1371/journal.pone.0014462
Donnelly OG, Errington-Mais F, Steele L et al (2013) Measles virus causes immunogenic cell death in human melanoma. Gene Ther 20:7–15. doi:10.1038/gt.2011.205
Stanford MM, Shaban M, Barrett JW et al (2008) Myxoma virus oncolysis of primary and metastatic B16F10 mouse tumors in vivo. Mol Ther 16:52–59. doi:10.1038/sj.mt.6300348
Prestwich RJ, Ilett EJ, Errington F et al (2009) Immune-mediated antitumor activity of reovirus is required for therapy and is independent of direct viral oncolysis and replication. Clin Cancer Res 15:4374–4381. doi:10.1158/1078-0432.CCR-09-0334
Cerullo V, Seiler MP, Mane V, Brunetti-Pierri N, Clarke C, Bertin TK, Rodgers JR, Lee B (2007) Toll-like receptor 9 triggers an innate immune response to helper-dependent adenoviral vectors. Mol Ther 15:378–385. doi:10.1038/sj.mt.6300031
Andoniou CE, van Dommelen SL, Voigt V et al (2005) Interaction between conventional dendritic cells and natural killer cells is integral to the activation of effective antiviral immunity. Nat Immunol 6:1011–1019. doi:10.1038/ni1244
Edukulla R, Woller N, Mundt B et al (2009) Antitumoral immune response by recruitment and expansion of dendritic cells in tumors infected with telomerase-dependent oncolytic viruses. Cancer Res 69:1448–1458. doi:10.1158/0008-5472.CAN-08-1160
Wongthida P, Diaz RM, Pulido C et al (2011) Activating systemic T-cell immunity against self tumor antigens to support oncolytic virotherapy with vesicular stomatitis virus. Hum Gene Ther 22:1343–1353. doi:10.1089/hum.2010.216
Bridle BW, Stephenson KB, Boudreau JE et al (2010) Potentiating cancer immunotherapy using an oncolytic virus. Mol Ther 18:1430–1439. doi:10.1038/mt.2010.98
Shafren DR, Au GG, Nguyen T, Newcombe NG, Haley ES, Beagley L, Johansson ES, Hersey P, Barry RD (2004) Systemic therapy of malignant human melanoma tumors by a common cold-producing enterovirus, coxsackievirus a21. Clin Cancer Res 10:53–60
Hersey P, Gallagher S (2014) Intralesional immunotherapy for melanoma. J Surg Oncol 109:320–326. doi:10.1002/jso.23494
Galivo F, Diaz RM, Thanarajasingam U et al (2010) Interference of CD40L-mediated tumor immunotherapy by oncolytic vesicular stomatitis virus. Hum Gene Ther 21:439–450. doi:10.1089/hum.2009.143
Diaconu I, Cerullo V, Hirvinen ML et al (2012) Immune response is an important aspect of the antitumor effect produced by a CD40L-encoding oncolytic adenovirus. Cancer Res 72:2327–2338. doi:10.1158/0008-5472.CAN-11-2975
Andarini S, Kikuchi T, Nukiwa M et al (2004) Adenovirus vector-mediated in vivo gene transfer of OX40 ligand to tumor cells enhances antitumor immunity of tumor-bearing hosts. Cancer Res 64:3281–3287
Hayata K, Iwahashi M, Ojima T et al (2013) Inhibition of IL-17A in tumor microenvironment augments cytotoxicity of tumor-infiltrating lymphocytes in tumor-bearing mice. PLoS ONE 8:e53131. doi:10.1371/journal.pone.0053131
Rommelfanger DM, Compte M, Diaz RM, Ilett E, Alvarez-Vallina L, Thompson JM, Kottke TJ, Melcher A, Vile RG (2013) The efficacy versus toxicity profile of combination virotherapy and TLR immunotherapy highlights the danger of administering TLR agonists to oncolytic virus-treated mice. Mol Ther 21:348–357. doi:10.1038/mt.2012.204
Zamarin D, Holmgaard RB, Subudhi SK, Park JS, Mansour M, Palese P, Merghoub T, Wolchok JD, Allison JP (2014) Localized oncolytic virotherapy overcomes systemic tumor resistance to immune checkpoint blockade immunotherapy. Sci Transl Med 6:226ra32. doi:10.1126/scitranslmed.3008095
Mastrangelo MJ, Maguire HC Jr, Eisenlohr LC, Laughlin CE, Monken CE, McCue PA, Kovatich AJ, Lattime EC (1999) Intratumoral recombinant GM-CSF-encoding virus as gene therapy in patients with cutaneous melanoma. Cancer Gene Ther 6:409–422. doi:10.1038/sj.cgt.7700066
Senzer NN, Kaufman HL, Amatruda T et al (2009) Phase II clinical trial of a granulocyte-macrophage colony-stimulating factor-encoding, second-generation oncolytic herpesvirus in patients with unresectable metastatic melanoma. J Clin Oncol 27:5763–5771. doi:10.1200/JCO.2009.24.3675
Goins WF, Huang S, Cohen JB, Glorioso JC (2014) Engineering HSV-1 vectors for gene therapy. Methods Mol Biol 1144:63–79. doi:10.1007/978-1-4939-0428-0_5
Dummer R, Rochlitz C, Velu T et al (2008) Intralesional adenovirus-mediated interleukin-2 gene transfer for advanced solid cancers and melanoma. Mol Ther 16:985–994. doi:10.1038/mt.2008.32
Gupta P, Su ZZ, Lebedeva IV et al (2006) mda-7/IL-24: multifunctional cancer-specific apoptosis-inducing cytokine. Pharmacol Ther 111:596–628. doi:10.1016/j.pharmthera.2005.11.005
Ning J, Wakimoto H (2014) Oncolytic herpes simplex virus-based strategies: toward a breakthrough in glioblastoma therapy. Front Microbiol 5:303. doi:10.3389/fmicb.2014.00303
Amos SM, Pegram HJ, Westwood JA et al (2011) Adoptive immunotherapy combined with intratumoral TLR agonist delivery eradicates established melanoma in mice. Cancer Immunol Immunother 60:671–683. doi:10.1007/s00262-011-0984-8
Lou Y, Liu C, Lizee G et al (2011) Antitumor activity mediated by CpG: the route of administration is critical. J Immunother 34:279–288. doi:10.1097/CJI.0b013e31820d2a05
Nierkens S, den Brok MH, Roelofsen T, Wagenaars JA, Figdor CG, Ruers TJ, Adema GJ (2009) Route of administration of the TLR9 agonist CpG critically determines the efficacy of cancer immunotherapy in mice. PLoS ONE 4:e8368. doi:10.1371/journal.pone.0008368
Nierkens S, den Brok MH, Garcia Z et al (2011) Immune adjuvant efficacy of CpG oligonucleotide in cancer treatment is founded specifically upon TLR9 function in plasmacytoid dendritic cells. Cancer Res 71:6428–6437. doi:10.1158/0008-5472.CAN-11-2154
Marabelle A, Kohrt H, Sagiv-Barfi I et al (2013) Depleting tumor-specific Tregs at a single site eradicates disseminated tumors. J Clin Invest 123:2447–2463. doi:10.1172/JCI64859
Shirota Y, Shirota H, Klinman DM (2012) Intratumoral injection of CpG oligonucleotides induces the differentiation and reduces the immunosuppressive activity of myeloid-derived suppressor cells. J Immunol 188:1592–1599. doi:10.4049/jimmunol.1101304
Kobayashi N, Hong C, Klinman DM, Shirota H (2013) Oligodeoxynucleotides expressing polyguanosine motifs promote antitumor activity through the upregulation of IL-2. J Immunol 190:1882–1889. doi:10.4049/jimmunol.1201063
Stone GW, Barzee S, Snarsky V, Santucci C, Tran B, Langer R, Zugates GT, Anderson DG, Kornbluth RS (2009) Nanoparticle-delivered multimeric soluble CD40L DNA combined with Toll-Like Receptor agonists as a treatment for melanoma. PLoS ONE 4:e7334. doi:10.1371/journal.pone.0007334
Davis MB, Vasquez-Dunddel D, Fu J, Albesiano E, Pardoll D, Kim YJ (2011) Intratumoral administration of TLR4 agonist absorbed into a cellular vector improves antitumor responses. Clin Cancer Res 17:3984–3992. doi:10.1158/1078-0432.CCR-10-3262
Oldford SA, Haidl ID, Howatt MA, Leiva CA, Johnston B, Marshall JS (2010) A critical role for mast cells and mast cell-derived IL-6 in TLR2-mediated inhibition of tumor growth. J Immunol 185:7067–7076. doi:10.4049/jimmunol.1001137
Craft N, Bruhn KW, Nguyen BD, Prins R, Lin JW, Liau LM, Miller JF (2005) The TLR7 agonist imiquimod enhances the anti-melanoma effects of a recombinant Listeria monocytogenes vaccine. J Immunol 175:1983–1990
Hayashi T, Chan M, Norton JT et al (2011) Additive melanoma suppression with intralesional phospholipid-conjugated TLR7 agonists and systemic IL-2. Melanoma Res 21:66–75. doi:10.1097/CMR.0b013e328340ce6c
Kalb ML, Glaser A, Stary G, Koszik F, Stingl G (2012) TRAIL(+) human plasmacytoid dendritic cells kill tumor cells in vitro: mechanisms of imiquimod- and IFN-alpha-mediated antitumor reactivity. J Immunol 188:1583–1591. doi:10.4049/jimmunol.1102437
Drobits B, Holcmann M, Amberg N, Swiecki M, Grundtner R, Hammer M, Colonna M, Sibilia M (2012) Imiquimod clears tumors in mice independent of adaptive immunity by converting pDCs into tumor-killing effector cells. J Clin Invest 122:575–585. doi:10.1172/JCI61034
Tamada K, Chen L (2006) Renewed interest in cancer immunotherapy with the tumor necrosis factor superfamily molecules. Cancer Immunol Immunother 55:355–362. doi:10.1007/s00262-005-0081-y
Kwong B, Gai SA, Elkhader J, Wittrup KD, Irvine DJ (2013) Localized immunotherapy via liposome-anchored Anti-CD137+ IL-2 prevents lethal toxicity and elicits local and systemic antitumor immunity. Cancer Res 73:1547–1558. doi:10.1158/0008-5472.CAN-12-3343
Quetglas JI, Dubrot J, Bezunartea J, Sanmamed MF, Hervas-Stubbs S, Smerdou C, Melero I (2012) Immunotherapeutic synergy between anti-CD137 mAb and intratumoral administration of a cytopathic Semliki Forest virus encoding IL-12. Mol Ther 20:1664–1675. doi:10.1038/mt.2012.56
Marabelle A, Kohrt H, Caux C, Levy R (2014) Intratumoral immunization: a new paradigm for cancer therapy. Clin Cancer Res 20:1747–1756. doi:10.1158/1078-0432.CCR-13-2116
Marabelle A, Kohrt H, Levy R (2013) Intratumoral anti-CTLA-4 therapy: enhancing efficacy while avoiding toxicity. Clin Cancer Res 19:5261–5263. doi:10.1158/1078-0432.CCR-13-1923
Fransen MF, Ossendorp F, Arens R, Melief CJ (2013) Local immunomodulation for cancer therapy: providing treatment where needed. Oncoimmunology 2:e26493. doi:10.4161/onci.26493
Ishikawa H, Barber GN (2008) STING is an endoplasmic reticulum adaptor that facilitates innate immune signalling. Nature 455:674–678. doi:10.1038/nature07317
Gajewski TF, Corrales L (2015) New perspectives on type I IFNs in cancer. Cytokine Growth Factor Rev 26:175–178. doi:10.1016/j.cytogfr.2015.01.001
Nakhaei P, Hiscott J, Lin R (2010) STING-ing the antiviral pathway. J Mol Cell Biol 2:110–112. doi:10.1093/jmcb/mjp048
Burdette DL, Vance RE (2013) STING and the innate immune response to nucleic acids in the cytosol. Nat Immunol 14:19–26. doi:10.1038/ni.2491
Fuertes MB, Kacha AK, Kline J, Woo SR, Kranz DM, Murphy KM, Gajewski TF (2011) Host type I IFN signals are required for antitumor CD8+ T cell responses through CD8{alpha} + dendritic cells. J Exp Med 208:2005–2016. doi:10.1084/jem.20101159
Ishikawa H, Ma Z, Barber GN (2009) STING regulates intracellular DNA-mediated, type I interferon-dependent innate immunity. Nature 461:788–792. doi:10.1038/nature08476
Woo SR, Fuertes MB, Corrales L et al (2014) STING-dependent cytosolic DNA sensing mediates innate immune recognition of immunogenic tumors. Immunity 41:830–842. doi:10.1016/j.immuni.2014.10.017
Woo SR, Corrales L, Gajewski TF (2015) The STING pathway and the T cell-inflamed tumor microenvironment. Trends Immunol 36:250–256. doi:10.1016/j.it.2015.02.003
Ohkuri T, Ghosh A, Kosaka A, Zhu J, Ikeura M, David M, Watkins SC, Sarkar SN, Okada H (2014) STING contributes to antiglioma immunity via triggering type I IFN signals in the tumor microenvironment. Cancer Immunol Res 2:1199–1208. doi:10.1158/2326-6066.CIR-14-0099
Woodmansee C, Pillow J, Skinner RB Jr (2006) The role of topical immune response modifiers in skin cancer. Drugs 66:1657–1664
Alessi SS, Sanches JA, Oliveira WR, Messina MC, Pimentel ER, Festa Neto C (2009) Treatment of cutaneous tumors with topical 5% imiquimod cream. Clinics (Sao Paulo) 64:961–966. doi:10.1590/S1807-59322009001000005
Garland SM, Sellors JW, Wikstrom A, Petersen CS, Aranda C, Aractingi S, Maw RD, Imiquimod Study G (2001) Imiquimod 5% cream is a safe and effective self-applied treatment for anogenital warts–results of an open-label, multicentre Phase IIIB trial. Int J STD AIDS 12:722–729
Ooi T, Barnetson RS, Zhuang L, McKane S, Lee JH, Slade HB, Halliday GM (2006) Imiquimod-induced regression of actinic keratosis is associated with infiltration by T lymphocytes and dendritic cells: a randomized controlled trial. Br J Dermatol 154:72–78. doi:10.1111/j.1365-2133.2005.06932.x
Stockfleth E, Trefzer U, Garcia-Bartels C, Wegner T, Schmook T, Sterry W (2003) The use of Toll-like receptor-7 agonist in the treatment of basal cell carcinoma: an overview. Br J Dermatol 149(Suppl 66):53–56
Smirnov D, Schmidt JJ, Capecchi JT, Wightman PD (2011) Vaccine adjuvant activity of 3M-052: an imidazoquinoline designed for local activity without systemic cytokine induction. Vaccine 29:5434–5442. doi:10.1016/j.vaccine.2011.05.061
Hofmann MA, Kors C, Audring H, Walden P, Sterry W, Trefzer U (2008) Phase 1 evaluation of intralesionally injected TLR9-agonist PF-3512676 in patients with basal cell carcinoma or metastatic melanoma. J Immunother 31:520–527. doi:10.1097/CJI.0b013e318174a4df
Carpentier A, Metellus P, Ursu R et al (2010) Intracerebral administration of CpG oligonucleotide for patients with recurrent glioblastoma: a phase II study. Neuro Oncol 12:401–408. doi:10.1093/neuonc/nop047
Salazar AM, Erlich RB, Mark A, Bhardwaj N, Herberman RB (2014) Therapeutic in situ autovaccination against solid cancers with intratumoral poly-ICLC: case report, hypothesis, and clinical trial. Cancer Immunol Res 2:720–724. doi:10.1158/2326-6066.CIR-14-0024
Vom Berg J, Vrohlings M, Haller S, Haimovici A, Kulig P, Sledzinska A, Weller M, Becher B (2013) Intratumoral IL-12 combined with CTLA-4 blockade elicits T cell-mediated glioma rejection. J Exp Med 210:2803–2811. doi:10.1084/jem.20130678
Sondergaard H, Galsgaard ED, Bartholomaeussen M, Straten PT, Odum N, Skak K (2010) Intratumoral interleukin-21 increases antitumor immunity, tumor-infiltrating CD8+ T-cell density and activity, and enlarges draining lymph nodes. J Immunother 33:236–249. doi:10.1097/CJI.0b013e3181c0c1cb
Cha E, Daud A (2012) Plasmid IL-12 electroporation in melanoma. Hum Vaccin Immunother 8:1734–1738. doi:10.4161/hv.22573
Chinnasamy D, Yu Z, Kerkar SP, Zhang L, Morgan RA, Restifo NP, Rosenberg SA (2012) Local delivery of interleukin-12 using T cells targeting VEGF receptor-2 eradicates multiple vascularized tumors in mice. Clin Cancer Res 18:1672–1683. doi:10.1158/1078-0432.CCR-11-3050
Yang RK, Kalogriopoulos NA, Rakhmilevich AL et al (2012) Intratumoral hu14.18-IL-2 (IC) induces local and systemic antitumor effects that involve both activated T and NK cells as well as enhanced IC retention. J Immunol 189:2656–2664. doi:10.4049/jimmunol.1200934
Pan J, Zhang M, Wang J, Wang Q, Xia D, Sun W, Zhang L, Yu H, Cao X (2005) Intratumoral injection of interferon-gamma gene-modified dendritic cells elicits potent antitumor effects: effective induction of tumor-specific CD8+ CTL response. J Cancer Res Clin Oncol 131:468–478. doi:10.1007/s00432-004-0651-y
Van der Jeught K, Joe PT, Bialkowski L, Heirman C, Daszkiewicz L, Liechtenstein T, Escors D, Thielemans K, Breckpot K (2014) Intratumoral administration of mRNA encoding a fusokine consisting of IFN-beta and the ectodomain of the TGF-beta receptor II potentiates antitumor immunity. Oncotarget 5:10100–10113
Heinzerling L, Burg G, Dummer R, Maier T, Oberholzer PA, Schultz J, Elzaouk L, Pavlovic J, Moelling K (2005) Intratumoral injection of DNA encoding human interleukin 12 into patients with metastatic melanoma: clinical efficacy. Hum Gene Ther 16:35–48. doi:10.1089/hum.2005.16.35
Weide B, Eigentler TK, Pflugfelder A et al (2014) Intralesional treatment of stage III metastatic melanoma patients with L19-IL2 results in sustained clinical and systemic immunologic responses. Cancer Immunol Res 2:668–678. doi:10.1158/2326-6066.CIR-13-0206
Okano S, Kondoh H, Toshima T et al (2013) Fas-deficient fully allogeneic dendritic cells administered via an intratumoral injection route show efficient antitumor effects in murine models. Fukuoka Igaku Zasshi 104:15–26
Liu C, Lou Y, Lizee G et al (2008) Plasmacytoid dendritic cells induce NK cell-dependent, tumor antigen-specific T cell cross-priming and tumor regression in mice. J Clin Invest 118:1165–1175. doi:10.1172/JCI33583
Mito K, Sugiura K, Ueda K et al (2010) IFN{gamma} markedly cooperates with intratumoral dendritic cell vaccine in dog tumor models. Cancer Res 70:7093–7101. doi:10.1158/0008-5472.CAN-10-0600
Fujimura T, Nakagawa S, Ohtani T, Ito Y, Aiba S (2006) Inhibitory effect of the polyinosinic-polycytidylic acid/cationic liposome on the progression of murine B16F10 melanoma. Eur J Immunol 36:3371–3380. doi:10.1002/eji.200636053
Shevtsov MA, Kim AV, Samochernych KA, Romanova IV, Margulis BA, Guzhova IV, Yakovenko IV, Ischenko AM, Khachatryan WA (2014) Pilot study of intratumoral injection of recombinant heat shock protein 70 in the treatment of malignant brain tumors in children. Onco Targets Ther 7:1071–1081. doi:10.2147/OTT.S62764
Galili U (2011) Conversion of tumors into autologous vaccines by intratumoral injection of alpha-Gal glycolipids that induce anti-Gal/alpha-Gal epitope interaction. Clin Dev Immunol. doi:10.1155/2011/134020
Doukas J, Rolland A (2012) Mechanisms of action underlying the immunotherapeutic activity of Allovectin in advanced melanoma. Cancer Gene Ther 19:811–817. doi:10.1038/cgt.2012.69
Sandin LC, Eriksson F, Ellmark P, Loskog AS, Totterman TH, Mangsbo SM (2014) Local CTLA4 blockade effectively restrains experimental pancreatic adenocarcinoma growth in vivo. Oncoimmunology 3:e27614. doi:10.4161/onci.27614
Mahvi DM, Henry MB, Albertini MR, Weber S, Meredith K, Schalch H, Rakhmilevich A, Hank J, Sondel P (2007) Intratumoral injection of IL-12 plasmid DNA-results of a phase I/IB clinical trial. Cancer Gene Ther 14:717–723. doi:10.1038/sj.cgt.7701064
Hofbauer GF, Baur T, Bonnet MC, Tartour E, Burg G, Berinstein NL, Dummer R (2008) Clinical phase I intratumoral administration of two recombinant ALVAC canarypox viruses expressing human granulocyte-macrophage colony-stimulating factor or interleukin-2: the transgene determines the composition of the inflammatory infiltrate. Melanoma Res 18:104–111. doi:10.1097/CMR.0b013e3282f702cf
Kaufman HL, Kim DW, DeRaffele G, Mitcham J, Coffin RS, Kim-Schulze S (2010) Local and distant immunity induced by intralesional vaccination with an oncolytic herpes virus encoding GM-CSF in patients with stage IIIc and IV melanoma. Ann Surg Oncol 17:718–730. doi:10.1245/s10434-009-0809-6
Khorana AA, Rosenblatt JD, Sahasrabudhe DM et al (2003) A phase I trial of immunotherapy with intratumoral adenovirus-interferon-gamma (TG1041) in patients with malignant melanoma. Cancer Gene Ther 10:251–259. doi:10.1038/sj.cgt.7700568
Rochlitz C, Dreno B, Jantscheff P et al (2002) Immunotherapy of metastatic melanoma by intratumoral injections of Vero cells producing human IL-2: phase II randomized study comparing two dose levels. Cancer Gene Ther 9:289–295. doi:10.1038/sj.cgt.7700441
Triozzi PL, Khurram R, Aldrich WA, Walker MJ, Kim JA, Jaynes S (2000) Intratumoral injection of dendritic cells derived in vitro in patients with metastatic cancer. Cancer 89:2646–2654
Acknowledgments
This work was supported by the National Institutes of Health (NIH) Grants R01 1CA143077 (Willem W. Overwijk), P01 CA128913 (Patrick Hwu/Willem W. Overwijk).
Conflict of interest
The authors disclose no potential conflicts of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
This paper is a Focussed Research Review based on a presentation given at the Twelfth Annual Meeting of the Association for Cancer Immunotherapy (CIMT), held in Mainz, Germany, 6th–8th May, 2014. It is part of a CII series of Focussed Research Reviews and meeting report.
Rights and permissions
About this article

Cite this article
Singh, M., Overwijk, W.W. Intratumoral immunotherapy for melanoma. Cancer Immunol Immunother 64, 911–921 (2015). https://doi.org/10.1007/s00262-015-1727-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00262-015-1727-z