
Abstract
Purpose
To test the applicability of National Comprehensive Cancer Network (NCCN v 3.2017) resectability criteria for pancreatic ductal adenocarcinoma (PDAC) in clinical practice, at a high-volume tertiary referral center.
Materials and methods
102 consecutive patients (53 female; mean age 66.2 years, range 34–90 years) with biopsy proven, non-metastatic PDAC were evaluated by our multidisciplinary pancreatic cancer program between July 2013 and February 2016. Retrospective review of staging pancreatic CT angiography was performed, and radiographic features were categorized as conforming to or non-conforming to existing v 3.2017 definitions.
Results
Among 102 patients, 10 (10%) had CTA evidence of vascular involvement that did not conform to existing NCCN Guidelines. Six new scenarios of vascular involvement were identified. The remaining 92 patients presented with resectable (n = 20 [22%]), borderline resectable (n = 42 [45.6%]), or unresectable (n = 30 [33%]) PDAC. Approximately half (n = 21 [51%]) of borderline resectable patients’ tumors demonstrated isolated venous involvement, whereas 39% had both arterial and venous involvement. A minority (11%) demonstrated only major arterial involvement. Assignment to unresectable status reflected both arterial and venous involvement (11, 37%), arterial involvement only (10, 33%) patients, and unreconstructible venous involvement in 9 (30%).
Conclusion
In our experience, current NCCN resectability guidelines for PDAC do not accurately classify vascular involvement identified in approximately 10% of patients. Revision of the current guidelines could be helpful to clinical practice.
We’re sorry, something doesn't seem to be working properly.
Please try refreshing the page. If that doesn't work, please contact support so we can address the problem.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Pancreatic cancer is the third leading cause of cancer-associated death in the United States of America, and its incidence has been increasing by 1.3% each year between 2006 and 2010 [1]. Utilization of high-quality cross-sectional CT or MRI imaging for the diagnosis and adequate staging of pancreatic adenocarcinoma (PDAC) is crucial for patient management. Accurate imaging is critical to identify patients at potentially curable stages of disease and to prevent misallocation of local treatment among patients with unresectable cancer [2].
At present, there are many different systems throughout the world utilized for the staging of PDAC. However, one of the most applied systems that define resectability by analyzing the extent of vascular involvement is the National Comprehensive Cancer Network (NCCN) guidelines. The NCCN criteria determine the resectability status as three different scenarios: ‘resectable,’ ‘borderline resectable (BLR),’ and ‘unresectable.’ The criteria assign these categories by determining the extent of arterial and venous involvement by the PDAC [3]. In the absence of distant metastasis, the presence and degree of contact between the tumor and the peripancreatic vessels are considered the most important parameters for defining surgical resectability, and hence, the NCCN Guidelines are recommended as a valuable tool in aiding medical and surgical decision-making strategies [4, 5]. The current resectability criteria table is different from earlier versions (v 2.2016) by wording differences. “Presence of variant anatomy” was modified to say: “Solid tumor contact with variant arterial anatomy” also, the authors added the possibility to perform an Appleby procedure on a specific celiac artery involvement scenario. All active NCCN Guidelines are reviewed and updated at least annually and the guidelines are evaluated and updated on a continuing basis to guarantee that the recommendations take into account the most current evidence [6].
Among all imaging modalities available for the evaluation of pancreatic pathology, multi-detector computed tomography (MDCT) CT angiography has demonstrated the best accuracy in the assessment of vascular involvement showing excellent sensitivity (100%), specificity (72%), and high positive predictive value (89%) [7]. MDCT pancreatic CTA is, therefore, currently the primary imaging modality in the evaluation of patients with known or suspected pancreatic malignancy.
This study tests the applicability of current v3.2017 NCCN Guidelines in defining the resectability of patients with pancreatic ductal adenocarcinoma using the state-of-the-art MDCT pancreatic CTA and demonstrates significant omissions relevant in common clinical practice.
Materials and methods
Sample population
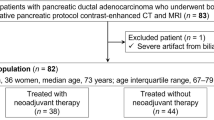
This study was approved by our Institutional Review board and was compliant with the Health Insurance Portability and Accountability Act (HIPPA). Waiver of informed patient consent was obtained for this retrospective study. Patients were evaluated by our multidisciplinary pancreatic cancer program that included but not limited to abdominal radiologists, expert liver and pancreatic surgeons, radiotherapists and oncologists. The inclusion and exclusion criteria included patients with non-metastatic, treatment naïve, biopsy-proven PDAC, that underwent MDCT staging (n = 102) between July 2013 and February 2016 and that were assessed by our multidisciplinary clinic (MDC) team. Patients that underwent MRI/MRCP staging were excluded from the study (n = 8). After the patients were evaluated and the treatment was decided by the MDC, the staging MDCT was re-reviewed by our expert radiologist for our study.
Imaging technique
Staging MDCT scans were acquired from various helical 64 multi-detector row CT scanners (Siemens, Toshiba, and GE). We used two cups of water as an oral contrast medium 15 min prior for better visualization of the duodenum. Next, we used a split-bolus injection pancreas CTA protocol that is being used consistently in our practice for staging primary pancreatic tumors [8, 9]. A 40-cc saline bolus was injected prior to contrast administration at a rate of 4.5 cc/s. The total volume of contrast (Omnipaque 350, GE Healthcare, Milwaukee, WIS, USA) was injected at a rate of 4.5 cc/s depending on the patient’s body mass index (BMI) and with a pause between the initial and second bolus: 150 cc (100/50 cc split, 33 s pause) for BMI < 25 kg/m2, 170 cc (120/50 cc split, 29 s pause) for BMI between 25 and 35 kg/m2, and 200 cc (150/50 cc split, 22 s pause) for BMI > 35 kg/m2. A 40-cc saline chaser followed contrast injection at a rate of 4.5 cc/s. Scanning was started after an 80-s delay. Routine coronal and sagittal reformatted images reconstructed images were also available for review.
Imaging analysis
All MDCT angiography images were reviewed by a single radiologist (KJM) with 19 years of experience interpreting pancreatic and abdominal cross-sectional high-resolution images. All cases were reviewed, staged and allocated to one of three categories regarding their resectability status according to NCCN Guidelines Version 3.2017 [5] (Table 1). We determined the resectability status of each patient by identifying the extent and location of both arterial and venous contacts of the tumor. For each patient, we recorded two facts: the presence or absence of tumor contact and the degree of contact of the tumor with the peripancreatic arteries and veins. The reader was aware that all cases had the pathological diagnosis of PDAC, and had access to the patient’s age and gender, but blinded to all additional relevant clinical history. The review was performed using a commercially available Picture Archiving and Communications System (PACS—GE Healthcare/Milwaukee, USA). The radiological evaluation was not time-limited, and the radiologist was free to change the zoom level and the window settings to his preference.
After all the patients were reviewed, only the radiological scenarios that did not fit with the current NCCN table were evaluated with our expert surgeon (AJM) to independently classify findings according to their resectability status based on his expertise.
Results
Patient demographics
The final study population consisted of 102 patients: 53 females (52%) and 49 males (48%) with a mean age of 66.2 years (range 34–90 years). The PDAC were located in the pancreatic head and neck (n = 93; 91%), body (n = 8; 8%), and tail (n = 1, 1%).
Pancreatic CTA findings
Existing NCCN Guidelines classified 20 patients (20%) as resectable, 42 patients (41%) as borderline resectable, and 30 patients (29%) unresectable. Radiographic findings in 10 patients (9.8%) did not conform to existing scenarios of vascular involvement (Fig. 1). These previously uncategorized scenarios were classified as resectable (n = 1, 10%), borderline (n = 6, 60%), or unresectable (n = 3, 30%).

The total number of patients staged according to the NCCN 3.2017 resectability criteria. BRL borderline resectable
Six specific scenarios were identified (Table 2): (1) solid head tumor contact with the common hepatic artery (CHA) with extension to the proper hepatic artery (PHA) and hepatic artery bifurcation (n = 4) (Fig. 2); (2) solid body tumor contact with the CHA ≤ 180° (n = 2) (Fig. 3); (3) solid body tumor contact with the CHA of > 180° (n = 1) (Fig. 4); solid body tumor contact with the CHA of > 180° with extension to celiac axis (CA) (n = 1) (Fig. 5); (5) solid neck tumor contact with the CHA of > 180° (n = 1) (Fig. 6); and (6) solid tumor contact to adjacent organs (kidney, stomach, spleen) (n = 1) (Fig. 7).

A 65-year-old woman presenting with abdominal pain and weight loss with unresectable disease. A Contrast-enhanced axial CT image shows encasement of the proper hepatic artery (white arrowhead) with extension to the left hepatic artery (black arrow). B Contrast-enhanced axial CT image shows also tumor encasement of the right hepatic artery (arrow). C Maximum intensity projection (MIP) image from CTA dataset shows irregularity of the common hepatic artery (arrow), and irregularity of left and right hepatic arteries (arrowheads)

Borderline resectable if the GDA is spared. A 61-year-old woman presenting with moderate abdominal pain. A Maximum intensity projection (MIP) image from CTA dataset shows the presence of body tumor (arrow); superior mesenteric vein (asterisk). B Contrast-enhanced coronal CT image shows tumor contact of less than 180° with the common hepatic artery (arrow)

A 73-year-old woman presenting with abdominal pain. Borderline resectable if GDA is spared; unresectable if not. A Contrast-enhanced axial CT image shows encasement of the common hepatic artery by the body tumor; superior mesenteric vein (asterisk). B Maximum intensity projection (MIP) image from CTA dataset shows narrowing of the common hepatic artery (arrowheads) by the tumor

A 85-year-old woman presenting with abdominal pain and weight loss. A Contrast-enhanced axial CT image shows a head tumor surrounding the common bile duct which has a metallic stent in place (white arrowhead). B Contrast-enhanced axial CT image shows tumor encasement of the common hepatic artery by more than 180° (black arrowhead) and tumor extension to the celiac axis (arrow). C Maximum intensity projection (MIP) image from CTA dataset shows encasement of the common hepatic artery (CHA), the splenic artery (SA), and extension of the tumor to the celiac axis (CA) (white arrow) demonstrating unresectable disease

A 64-year-old female with jaundice. A Contrast-enhanced axial CT image shows the location of the tumor in the neck of the pancreas (delineated area) and normal pancreatic tissue in the head (asterisk). B Contrast-enhanced axial CT image shows encasement of both the common hepatic artery (white arrow) and the right hepatic artery (black arrow). There is a common bile duct stent in place (white arrowhead) with unresectable disease. C Maximum intensity projection (MIP) image from CTA dataset shows narrowing of the common hepatic artery (arrowheads)

Contrast-enhanced axial CT images from a 51-year-old female presenting with left abdominal pain show resectable tumor (asterisk) with invasion of the kidney (arrow), stomach (white arrowheads), and spleen (black arrowheads) presenting with borderline resectable disease due to the need for multi-visceral resection
Types and frequency of vascular involvement
NCCN criteria were applicable in 92 patients, of whom 20 were resectable, 42 borderline, and 30 unresectable. Among 42 borderline resectable patients, 21 (50%) demonstrated isolated venous involvement, 16 (38%) had both arterial and venous involvement, and 5 (12%) had arterial involvement alone. Unresectable patients demonstrated prohibitive arterial and venous involvement in 11 (37%), advanced arterial involvement (10, 33%), and unreconstructible vein involvement in 9 (30%) (Fig. 8).

Arterial and venous involvement on each of the status accordingly to the NCCN 3.2017 criteria defining resectability status. BRL borderline resectable
Follow-up
All of our patients underwent neoadjuvant therapy to downsize the tumor for a probable resection of the tumor. At the end of this study, 35 (34.3%) patients underwent surgical resection [26 Whipple procedure (pancreatoduodenectomy), 8 distal pancreatectomies and one Appleby modified resection].
Discussion
Pancreatic ductal adenocarcinoma (PDAC) is the third leading cause of cancer-related deaths in the United States with incidence equaling mortality [2]. According to the American Joint Commission on Cancer (AJCC), PDAC is staged based on the TNM system, which categorizes the primary mass by size (T), the spread of nearby lymph nodes (N), and the presence of metastases (M). For resectability purposes, however, a staging system based on computed tomography angiography (CTA) findings has been created by the National Comprehensive Cancer Network (NCCN) with its primary focus on the vascular involvement of the tumor. This system is intended for the assessment and categorization of resectability status in PDAC into three groups: ‘resectable,’ ‘borderline resectable’ (BLR), and ‘unresectable’ [10]. To the best of our knowledge, no comprehensive report has described the radiological applicability of the NCCN Guidelines (current version: 3.2017 for PDAC) in a large cohort of patients. A proper review of the applicability of the NCCN Guidelines for PDAC would present substantial advantages and implications. First, the radiological features and clinical presentations of PDAC, as shown in multiple studies, vary widely from patient to patient [2, 5, 11, 12]. Second, an adequate determination of the extent of disease on imaging at the time of staging is one of the most important steps in optimal patient management for pancreatic cancer [12].
Therefore, in this study, we evaluated the applicability of the defining resectability criteria using the current NCCN Guidelines for a total of 102 consecutive patients with pathologically proven PDAC encountered in our clinical practice. A total of 90% of patients were able to be grouped following the NCCN resectability criteria, while 10% presented with radiological scenarios that are not depicted on the current guidelines criteria. Within this subgroup, more than half of the patients (n = 6) were accordingly grouped as “borderline resectable” due to additional solid tumor involvement found according to the following scenarios. The absence of radiological scenarios in these commonly used standardized criteria such as the aforementioned findings can lead to an incorrect treatment decision, by either overestimating or underestimating the extent of disease.
Modification of current NCCN Guidelines regarding major arterial involvement is a necessary prerequisite to accurately compare the scenarios based on the preoperative status prior to multimodality therapy. Evolving multimodality approaches to preoperative treatment of pancreatic cancer may impact the likelihood of prolonged disease-free survival after advanced surgical resection among some classes of patients treated at expert centers [13,14,15]. These data will remain heterogeneous and subject to significant selection bias until radiological classification precisely defines the location and extent of regional disease upon entry to intent-to-treat protocols designed to maximize survival after potentially curative surgery matched to attendant major postoperative morbidity [16].
With regard to the analysis of how frequent and why patients were classified in one of three groups, we identified that the BLR category comprised 51% of patients due to solid tumor contact with SMV or PV of less than 180°. As for the arterial standpoint, only 10% were found to be BLR due to solid tumor contact with either CA or SMA of less than 180° or, due to solid tumor contact to the CHA without extension to celiac axis or hepatic artery. In the unresectable category, 37% were deemed unresectable due to an unreconstructible SMV/PV or due to contact with the most proximal draining jejunal branch into the SMV. Thirty-three percent were considered unresectable due to solid tumor contact with SMA/CA greater than 180° or solid tumor contact to the first jejunal branch (Fig. 7).
Our study has various limitations. First, it was a retrospective study performed in a single institution. Second, only one radiologist was involved in the CT staging of the pancreatic cancers. Further research into the study’s findings may assist to anchor the above data.
In conclusion, the current NCCN resectability criteria lack six radiological scenarios found in 10% of the patients in our study. Henceforth, we believe that these broadly used resectability criteria could be reviewed so medical centers, which do not have the convenience of having expert abdominal radiologists, expert pancreatic/vascular surgeons and a weekly based multidisciplinary clinics as we do in our institution, can base their treatment approach aided by a more generalizable table (Table 3).
References
Ferlay J, Soerjomataram I, Ervik M, Dikshit R, Eser S, Mathers C, Rebelo M, Parkin D, Bray F (2013) GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11 [Internet]. International Agency for Research on Cancer. http://globocan.iarc.fr. Accessed 7 July 2017
American Cancer Society (2014) Pancreatic cancer. https://www.cancer.org/cancer/pancreatic-cancer.html. Accessed 7 July 2017
Tempero MA, Arnoletti JP, Behrman S, et al. (2010) Pancreatic adenocarcinoma. J Natl Compr Canc Netw. 8:972–1017
Wong JC, Raman S (2010) Surgical resectability of pancreatic adenocarcinoma: CTA. Abdom Imaging 35:471–480. https://doi.org/10.1007/s00261-009-9539-2
National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology. Pancreatic adenocarcinoma. NCCN Guidelines version 3.2017 https://www.nccn.org/professionals/physician_gls/f_guidelines.asp. Accessed 7 July 2017
NCCN Guidelines® & Clinical Resources (2017) Updates to the NCCN Guidelines. https://www.nccn.org/professionals/development.aspx. Accessed 10 Dec 2017
Al-Hawary MM, Francis IR, Chari ST (2014) Pancreatic ductal adenocarcinoma radiology reporting template: consensus statement of the Society of Abdominal Radiology and the American Pancreatic Association. Radiology 270:248–260. https://doi.org/10.1148/radiol.13131184
Camacho A, Fang J, Cohen MP, et al. (2017) Split-bolus pancreas CTA protocol for local staging of pancreatic cancer and detection and characterization of liver lesions. Abdom Radiol . https://doi.org/10.1007/s00261-017-1350-x
Brook OR, Gourtsoyianni S, Brook A, et al. (2013) Split-bolus spectral multidetector CT of the pancreas: assessment of radiation dose and tumor conspicuity. Radiology 269:139–148. https://doi.org/10.1148/radiol.13121409
Tempero MA, Malafa MP, Behrman SW, et al. (2008) Pancreatic adenocarcinoma, version 2.2014: featured updates to the NCCN Guidelines. J Natl Compr Cancer Netw 12(8):1083–1093. https://doi.org/10.6004/jnccn.2014.0106
Seufferlein T, Porzner M, Heinemann V, et al. (2014) Ductal pancreatic adenocarcinoma. Dtsch Arztebl Int 111:396–402. https://doi.org/10.3238/arztebl.2014.0396
Isaji S, Kawarada Y, Uemoto S (2004) Classification of pancreatic cancer: comparison of Japanese and UICC classifications. Pancreas 28:231–234
Bockhorn M, Burdelski C, Bogoevski D, et al. (2011) Arterial en bloc resection for pancreatic carcinoma. Br J Surg 98:86–92. https://doi.org/10.1002/bjs.7270
Aosasa S, Nishikawa M, Noro T, et al. (2016) Total pancreatectomy with celiac axis resection and hepatic artery restoration using splenic artery autograft interposition. J Gastrointest Surg 20:644–647. https://doi.org/10.1007/s11605-015-2991-0
Amano H, Miura F, Toyota N, et al. (2009) Is pancreatectomy with arterial reconstruction a safe and useful procedure for locally advanced pancreatic cancer? J Hepatobiliary Pancreat Surg 16:850–857. https://doi.org/10.1007/s00534-009-0190-7
Zakharova OP, Karmazanovsky GG, Egorov VI (2012) Pancreatic adenocarcinoma: outstanding problems. World J Gastrointest Surg 27(5):104–113. https://doi.org/10.4240/wjgs.v4.i5.104
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were by the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Rights and permissions
About this article

Cite this article
Garces-Descovich, A., Beker, K., Jaramillo-Cardoso, A. et al. Applicability of current NCCN Guidelines for pancreatic adenocarcinoma resectability: analysis and pitfalls. Abdom Radiol 43, 314–322 (2018). https://doi.org/10.1007/s00261-018-1459-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-018-1459-6