
Abstract
Purpose
Peptide receptor radionuclide therapy in patients with neuroendocrine tumours has yielded promising results. This prospective study investigated the feasibility of dosimetry of the kidneys and bone marrow during therapy and its impact on efficacy and outcome.
Methods
The study group comprised 200 consecutive patients with metastasized somatostatin receptor-positive neuroendocrine tumours progressing on standard therapy or not suitable for other therapeutic options. A treatment cycle consisted of 7.4 GBq 177Lu-DOTA-octreotate with co-infusion of a mixed amino acid solution, and cycles were repeated until the absorbed dose to the kidneys reached 23 Gy or there were other reasons for stopping therapy. The Ki-67 index was ≤2% in 47 patients (23.5%), 3–20% in 121 (60.5%) and >20% in 16 (8%).
Results
In 123 patients (61.5%) the absorbed dose to the kidneys reached 23 Gy with three to nine cycles during first-line therapy; in no patient was a dose to the bone marrow of 2 Gy reached. The best responses (according to RECIST 1.1) were a complete response (CR) in 1 patient (0.5%), a partial response (PR) in 47 (23.5%), stable disease (SD) in 135 (67.5%) and progressive disease (PD) in 7 (3.5%). Median progression-free survival was 27 months (95% CI 22–30 months) in all patients, 33 months in those in whom the absorbed dose to the kidneys reached 23 Gy and 15 months in those in whom it did not. Median overall survival (OS) was 43 months (95% CI 39–53 months) in all patients, 54 months in those in whom the absorbed dose to the kidneys reached 23 Gy and 25 months in those in whom it did not. Median OS was 60 months in patients with a best response of PR or CR, 42 months in those with SD and 16 months in those with PD. Three patients (1.5%) developed acute leukaemia, 1 patient (0.5%) chronic leukaemia (unconfirmed) and 30 patients (15%) grade 3 or 4 bone marrow toxicity. Eight patients (4%) developed grade 2 kidney toxicity and one patient (0.5%) grade 4 kidney toxicity.
Conclusions
Dosimetry-based therapy with 177Lu-DOTA-octreotate is feasible. Patients in whom the absorbed dose to the kidneys reached 23 Gy had a longer OS than those in whom it did not. Patients with CR/PR had a longer OS than those with SD. Bone marrow dosimetry did not predict toxicity.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Peptide receptor radionuclide therapy (PRRT) has been used successfully in patients with neuroendocrine tumours (NETs) for two decades [1,2,3,4,5]. 177Lu-DOTA-octreotate [5,6,7,8,9], different 90Y–labelled peptides [10,11,12,13,14] and combinations of both have been used. 177Lu-DOTA-octreotate has usually been administered according to a standard protocol with four cycles of 7.4 GBq [5, 8, 9]. When PRRT became available in Sweden, the legal demand for individualized planning of radiotherapy necessitated the development of dosimetry procedures suitable for use under clinical conditions [15,16,17,18,19,20]. The organs at risk are the kidneys and bone marrow, with a growing body of data demonstrating higher nephrotoxicity with 90Y–labelled peptides using several schedules [11, 14, 21] than with 177Lu-DOTA-octreotate [5, 22,23,24]. The physical properties of lutetium-177 are well suited to following the distribution of the radionuclide for dosimetry during therapy. For 177Lu-DOTA-octreotate, a cumulative absorbed dose of 23 Gy to the kidneys was taken from external beam radiation [25], a cautious cut-off value in the setting of PRRT [26, 27]. A 2-Gy cut-off value for the bone marrow was based on experience with radioiodine therapy [28]. From dosimetry data compiled in our department we concluded that about 50% of patients might be undertreated and able to receive more than 4 × 7.4 GBq of 177Lu-DOTA-octreotate before reaching either 23 Gy to the kidneys or 2 Gy to the bone marrow [17].
The present study was designed to investigate the efficacy of treatment with 177Lu-DOTA-octreotate guided by dosimetry in patients with advanced NETs who either have progressive disease or are not suitable for standard care protocols. The primary aims were to evaluate the feasibility of individualized dosimetry in a routine setting, the applicability of dosimetry as a stop criterion for therapy aiming at an absorbed dose of 23 Gy to the kidneys and a maximum of 2 Gy to the bone marrow, and the side effects of PRRT performed under these conditions. Secondary endpoints were objective response according to RECIST 1.1 [29], progression-free survival (PFS) and overall survival (OS).
Patients and methods
A total of 200 patients with NETs with somatostatin receptor expression higher than in normal liver (Krenning score 3 or 4 [30]) based on somatostatin receptor scintigraphy were enrolled after providing written informed consent (EudraCT no. 2009-012260-14). The local ethics and radiation ethics committees approved the study and the study was performed in accordance with the principles of the Declaration of Helsinki. Inclusion criteria were: metastatic NETs progressive on standard of care therapy, and proven intolerance or contraindications to other therapies. Patients with rectal NETs or bronchopulmonary carcinoids were accepted for first-line treatment, since no standard therapy has been established for metastatic disease. Life expectancy had to be more than 3 months, white blood cell count (WBC) >3.0 × 109/L, platelet count >100 × 109/L, bilirubin <40 μmol/L, albumin >25 g/L, creatinine <110 μmol/L or, if higher, glomerular filtration rate (cystatin-C) >50 ml/min/1.73 m2. Exclusion criteria were pregnancy, tumour amenable to surgery or radiofrequency ablation, and inability to stay isolated for 24 h. Of the 200 patients, 55% had small intestinal NETs (SI-NETs); for other tumour types see Table 1. After amendments to the initial study protocol, 16 patients (8%) diagnosed with grade 3 disease (Ki-67 index >20%) were accepted, and included those with a Ki-67 index up to 40%. All patients were receiving somatostatin analogues (SSA), and 43 (21.5%) had received higher than standard doses. SSA treatment was continued in all patients during PRRT. Patient characteristics are shown in Tables 1 and 2. The largest group of patients (84, 42%) were Swedish citizens; the remainder were referred from institutions in several other countries.
Patients were treated with 7.4 GBq 177Lu-DOTA-octreotate per cycle with an intended interval of 6 to 8 weeks. The peptide was a kind gift from Prof. Eric Krenning. Lutetium-177 was purchased from IDB, Holland BV, and labelling was performed in-house. Kidney protection was provided by infusion of 2 L of an amino acid mixture (Vamin, 14 g N/L, electrolyte-free; Kabi Fresenius) over 8 h, starting half an hour before infusion of the radiopeptide. One hour before therapy, 8 mg of betamethasone and 8 mg of ondansetron or 250 μg palonosetron were given intravenously as antiemetic. Before every treatment cycle, WBC had to be >3 × 109/L, granulocytes >1.5 × 109/L and platelets >100 × 109/L. Therapy was terminated if these criteria were not met within 6 months. As an exception, in some patients the activity was decreased by 30% instead of delaying treatment.
Cycles of 7.4 GBq 177Lu-DOTA-octreotate were repeated until the absorbed dose to the kidneys reached 23 Gy or there were other reasons for stopping therapy (Table 3). A cumulative absorbed dose of 2 Gy to the bone marrow was intended to act as a stop criterion, but was not reached in any of the patients during the initial treatment. In 14 patients (7%) with a favourable tumour response, salvage therapy aiming at a cumulative absorbed dose to the kidneys of 45 Gy was offered upon progression, given normal bone marrow and kidney function.
Dosimetry for solid organs and bone marrow was performed as previously described in detail [15,16,17]. For solid organs, dosimetry was based on the small volume method performed on single photon emission tomography with low-dose CT (SPECT/CT) at 1, 4 and 7 days after therapy. Volumes of 4 cm3 were drawn on representative regions with homogeneous uptake. The activity concentrations were fitted to a monoexponential function. To calculate absorbed doses to the kidneys, the time-integrated activity concentrations were multiplied by the appropriate dose concentration factor considering only self-dose:
where DO is the absorbed dose to the organ, and DCF is the dose concentration factor converting CcumO to absorbed dose by self absorption. Similarly, doses to the liver, spleen and representative tumours were calculated (data not shown). For complete bone marrow dosimetry, the dose from the blood activity (self-dose) was calculated from integrated blood activity curves derived from blood samples obtained at 0.5, 1, 2.5, 4, 8 and 24 h. This self-dose derived from the blood was complemented with the photon dose from resident activity in tumours, organs and the remainder of the body in order to calculate the total bone marrow dose. The photon dose was based on consecutive whole-body scans (WBS) at 1, 4 and 7 days after therapy. Regions of interests delineating the kidneys, liver, spleen, tumours and the whole body were drawn on geometrical mean images at 24 h and transferred to the images at 4 and 7 days. For calculation of the absorbed dose to bone marrow, the contribution of other source organs was added to the self-dose derived from the blood measurements as follows:
where DBM is the absorbed dose to the bone marrow, CcumBM is the time-integrated activity concentration in the bone marrow, DCF is the factor converting CcumBM to absorbed dose by self-absorption, AcumT is the time-integrated activity in tissue T (solid organs, tumour and the remainder of the body), and DFBM ← T is the factor converting AcumT to absorbed dose in the bone marrow (cross-fire).
Complete dosimetry was always performed during the first treatment, whenever large changes in tumour volume had occurred, after delay, and at least every fourth cycle. A short dosimetry protocol was performed for all other cycles after 24 h including a SPECT/CT scan over the abdomen and one WBS. The absorbed dose to the kidney was then calculated assuming an unchanged effective half-life, the amplitude for the area under the curve was adjusted for the actual measured activity concentration derived from the SPECT/CT scan at 24 h [16]. The self-dose from blood and the total bone marrow dose were calculated for each treatment with complete dosimetry and extrapolated for the remaining cycles by assuming the higher figure of two measurements for the adjacent unknown values. Radiological response was assessed using RECIST 1.1 criteria [29]. Whenever available, the biochemical response of biomarkers was monitored.
Follow-up, data collection and statistics
Study enrolment was between September 2010 and February 2014. For patients from Sweden and Oslo (72.5%) survival data were derived from the respective national health registries that were accessed until May 2016. The referring institutions supplied all other follow-up data.
Nephrotoxicity, hepatotoxicity and bone marrow toxicity were recorded according to WHO criteria. Time to progression was calculated from the start of therapy to the date of radiologically confirmed progression (RECIST 1.1) except in clinically clear cases of progression based on scintigraphy, tumour markers and/or ultrasonography when CT data were not available (ten patients). OS was calculated based on all deaths that occurred until May 2016. Statistical evaluations including survival analysis using parametric Weibull plots and Kaplan-Meier curves were performed with the JMP 12.0.1 software package (SAS Institute Inc., Cary, NC). Differences between groups were assumed to be significant at p < 0.05 and were calculated using the log-rank, Wilcoxon, Student’s t and Pearson’s chi-squared tests where applicable. All analyses were performed on an intention-to-treat basis; all patients were included in the survival analysis. Time to progression was not reported for one patient who was excluded from the PFS calculation.
Results
The dosimetry protocol applied was feasible. All patients underwent initial dosimetry. Most patients were able to leave hospital after 1 day, with patients who had to travel long distances staying in a hotel during weekdays when complete dosimetry was performed.
Dosimetry
An absorbed dose of 23 Gy to the kidneys was reached after three to nine cycles of 7.4 GBq 177Lu-DOTA-octreotate. During the initial treatment, 98 patients (49%) received more than four (five to ten) cycles of 7.4 GBq, with a maximum of 74 GBq. One patient with pancreatic NET received a tenth cycle upon reaching the 23 Gy level after a favourable response in order to reach a tumour burden qualifying him for surgery of his primary tumour, which was performed several months after the last cycle. He had no signs of haematological or kidney toxicity. Patients in whom the dose to the kidneys reached 23 Gy received one to five cycles. Accumulated absorbed doses to the bone marrow ranged from 0.07 to 1.77 Gy for the complete treatment and from 0.07 to 0.51 for the first single cycle (Table 3). Fifty patients received exactly four cycles. The absorbed dose to the kidneys reached 23 Gy in 33 patients. Therapy was discontinued in 17 patients for other reasons, in six due to bone marrow suppression, in one due to tumour shrinkage by more than 90%, and in all others due to progression, clinical deterioration or death.
Reasons for stopping therapy
First-line therapy was stopped upon reaching 23 Gy absorbed dose to the kidneys in 123 patients (61.5%), and in 114 of these this was the only stop criterion. The cumulative absorbed dose to the bone marrow did not reach 2 Gy in any patient. In 44 patients (22%) bone marrow-related toxicity was the only stop criterion. All reasons for stopping therapy are listed in Table 3.
Objective responses according to RECIST 1.1
Tumour response varied among NET types (Table 4). Patients with SI-NETs showed a significantly lower objective response rate than patients with pancreatic and rectal NETs. Figure 1 illustrates the difference in objective response rates between patients with SI-NET and those with non-SI-NET. The proportions of patients in both groups in whom the absorbed dose to the kidneys reached 23 Gy are indicated. Of patients in whom the dose to the kidneys reached 23 Gy, 30.9% obtained an objective response (complete response and partial response, CR/PR) compared with 13% of patients in whom the dose to the kidneys did not reach 23 Gy for any reason (p < 0.0001). The response rate of 10.6% in patients with tumours with a low proliferation rate (Ki-67 index ≤2%) was lower than in patients with higher proliferation rates (30.6% and 31.3% for Ki-67 index 3–20% and >20%, respectively).

Patients with small intestinal NET (SI NET) show lower objective response rates according to RECIST 1.1 than patients with all other types of tumours (Non-SI NET). The proportions of patients in the respective groups with complete and partial responses (CR/PR), stable disease (SD) and progressive disease (PD) or data not available for radiological evaluation (NA) are indicated. Shaded areas Proportions of patients in whom the absorbed dose to the kidneys reached 23 Gy (numbers of patients are given in Table 4)
Biochemical responses
Tumour markers including chromogranin A were available for analysis in 85 patients. A decrease of more than 50% in initially elevated levels occurred in 67% of patients, and was associated with a longer survival (median OS 60 months, 95% CI 42 months, upper limit not reached, NR) than a decrease of ≤50% (28 patients, 33%, median OS 35 months, 95% CI 17–52 months; p = 0.03). Tumour markers decreased by 50% or more in 80% of patients in whom the absorbed dose to the kidneys reached 23 Gy, but in only 45% of those in whom it did not (p = 0.0011). Of patients with an objective response (CR/PR), 91.3% (21 of 23) showed a decrease in tumour markers of more than 50%, in contrast to 62.5% of patients (35 of 56) with SD and 16.7% of nonresponders (1 of 6).
Overall and progression-free survival
Median follow-up was 31 months (range 1–68 months). Of the 200 patients, 106 (53%) were alive at the time of analysis, and of these, 29% were progression-free. The main cause of death was tumour progression (65 of 94 patients, 70%). In 16 patients (15%), the cause of death was unknown. Median OS was 43 months (95% CI 39–53 months) in all patients. Median OS in the patients in whom the absorbed dose to the kidneys reached 23 Gy was 54 months (95% CI 44 months, NR) and 25 months (95% CI 18–30 months) in those in whom it did not (p < 0.0001; Fig. 2, Table 5).

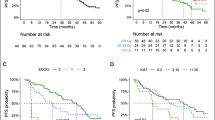
Progression-free survival (PFS; a, c, e) and overall survival (OS; b, d, f) from the start of therapy with 177Lu-DOTA-octreotate in relation to absorbed dose to the kidneys, best morphological response according to RECIST 1.1 and proliferation rate (Ki-67 index). a, b PFS (a) and OS (b) in 123 of 124 patients in whom the absorbed dose to the kidneys reached 23 Gy (blue line) and in 76 patients in whom it did not (red line); grey line combined data. c, d PFS (c) and OS (d) in relation to best response according to RECIST 1.1: progressive disease (PD, red line), median PFS 6 months (95% CI 3–9 months), median OS 15.5 months (95% CI 5–36 months); stable disease (SD, green line), median PFS 28 months (95% CI 21–31 months), OS 42 months (95% CI 34–51.5 months); partial response/complete response (PR&CR, blue line), median PFS 31 months (95% CI 23–35 months), OS 60 months (95% CI 43 months, upper limit not reached, NR). e, f PFS (e) and OS (f) in relation to proliferation rate (Ki-67 index): grade 1, Ki-67 index ≤2% (red line), PFS 33 months (95% CI 24–41 months), OS 48 months (95% CI 40 months, NR); grade 2, Ki-67 index 3–20% (green line), median PFS 23 months (95% CI 19–28 months), median OS 41 months (95% CI 32.5–60 months); grade 3, Ki-67 index >20% (blue line), median PFS 14 months (95% CI 10–21 months), median OS 31 months (95% CI 19–39 months)
Median PFS was 27 months (95% CI 22–30 months) in all patients, 33 months (95% CI 29–36 months) in patients in whom the absorbed dose to the kidneys reached 23 Gy during the initial treatment, and 15 months (95% CI 12–17 months) in those in whom it did not (p < 0.0001). In order to compensate for bias due to therapy discontinuation related to progression or deterioration of the patient during therapy, PFS and OS were also calculated after exclusion of 46 patients who stopped therapy for these reasons (Fig. 3). In the remaining 154 patients, PFS and OS were 34 and 60 months in those in whom the absorbed dose to the kidneys reached 23 Gy and 20 and 33 months in those in whom it did not, respectively (p = 0.001 for PFS, p = 0.0004 for OS). A subgroup analysis of patients who received exactly four cycles of 177Lu-DOTA-octreotate is shown in Fig. 4. OS, but not PFS, was significantly longer in patients with an objective response (CR/PR) than in patients with SD (median OS 60 months, 95% CI 43 months, NR, versus 42 months, 95% CI 34–52 months, p = 0.004; median PFS 31 months, 95% CI 23–35 months, versus 28 months, 95% CI 21–31 months, not significant; Fig. 2, Table 5). Patients with a lower Ki-67 index had longer PFS (Fig. 2).

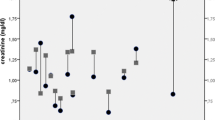
Progression-free survival (PFS, a) and overall survival (OS, b) in 154 patients who stopped therapy for reasons other than progression or clinical deterioration. In 114 patients in whom the absorbed dose to the kidneys reached 23 Gy, PFS was 34 months (95% CI 31–37 months) and OS was 60 months (95% CI 47 months, NR). In 39 of 40 patients in whom a dose of 23 Gy was not reached, PFS was 20 months (95% CI 16–28 months) and OS was 33 months (95% CI 29–48 months; p < 0.0001 for PFS, p = 0.0004 for OS); grey line combined data, red symbols patient died, blue symbols patient alive, triangles patient received salvage therapy

Progression-free survival (PFS, a) and overall survival (OS, b) in all 50 patients who received exactly four cycles of 177Lu-DOTA-octreotate. In 33 patients in whom the absorbed dose to the kidneys reached 23 Gy, PFS was 35 months (95% CI 23 months, NR) and OS was 60 months (95% CI 47 months, NR). In 17 patients in whom a dose of 23 Gy was not reached, PFS was 16 months (95% CI 9–18 months) and OS was 19 months (95% CI 15 months, NR; p = 0.0003 for PFS, p = 0.0006 for OS, log-rank test; grey line combined data, red symbols patient died, blue symbols patient alive, triangles patient received salvage therapy
Toxicity, side effects and serious adverse events
In 69 patients (34.5%), one or several cycles had to be delayed due to thrombocytopenia and/or leucopenia, alone or in combination with anaemia (Table 3). Grade 3 or 4 bone marrow toxicity of any kind was seen in 30 (15%) of the 200 patients. Bone marrow toxicity was generally transient and therapy was continued after the nadir had passed. The treatment was stopped in 44 patients (22%) for bone marrow-related reasons, including 5 patients with tumour progression while awaiting bone marrow recovery.
Grade 1 nephrotoxicity at any time was seen in 38 patients (19%), most of whom were stable or improved during therapy. Grade 2 nephrotoxicity was seen in 8 patients (4%), all but one with concomitant risk factors (arterial hypertension, cardiac insufficiency and/or diabetes mellitus). Grade 2 toxicity was seen in all patients at the time of progression during general deterioration prior to death. No grade 3 toxicity was seen. Grade 4 nephrotoxicity was seen in one female patient 3 years after therapy. This patient had a history of arterial hypertension, and treatment was stopped after cycle 2 because of an unexplained increase in the absorbed kidney dose from 6.1 to 9.1 Gy (right) and 6.4 to 9.6 Gy (left), resulting in cumulative absorbed doses of 15.2 to the right kidney and 16 Gy to the left kidney. Hypertensive nephrosclerosis was confirmed histologically.
Six patients died from cardiac events (infarction or progressive carcinoid heart failure) and four patients died from infections, two of them with cytopenic fever. Two patients developed and subsequently died from acute leukaemia, one myeloid (AML) and one lymphoblastic (ALL). One patient developed massive leucocytosis following a jaw infection and chronic myeloid leukaemia (CML) was suspected. The patient died due to the underlying infection before a final diagnosis could be established. One patient developed AML and was alive at the time of follow-up. This patient had previously received streptozotocin/capecitabine and temozolomide upon progression after PRRT. The patients with ALL and suspected CML had received temozolomide before PRRT. All four patients had bone marrow metastases. Leukaemia was diagnosed between 18 and 46 months after the start of PRRT.
Discussion
To our knowledge, this is the first prospective study to explore the outcome of PRRT with 177Lu-DOTA-octreotate in patients with NET applying systematic, individualized dosimetry of the kidneys and bone marrow. The study provides evidence supporting our assumption that about half of the patients can tolerate more than four cycles of 7.4 GBq 177Lu-DOTA-octreotate [17]. The question to be answered is whether outcome is improved in the substantial proportion of patients who would receive a higher activity than given using the widely accepted Rotterdam protocol of four cycles of 7.4 GBq 177Lu-DOTA-octreotate. In Table 6, the number of cycles per patient during the initial treatment is given, along with information as to whether 23 Gy to the kidneys was reached and the number of surviving patients at the time of analysis.
Data so far published are not easily compared since the studies were inhomogeneous regarding tumour type, risk factors and previous therapy as well as endpoints. In the present study, several risk factors were more prevalent than in the majority of other larger studies (Table 7). In 8% of patients the Ki-67 index was >20% and in 29% >10%, a level found to affect survival [7]. PFS was significantly lower in patients with a Ki-67 index >20% (Fig. 2), but a median PFS of 14 months (95% CI 10–21 months) and a median OS of 31 months (95% CI 19–39 months) in our 16 patients still compares well with previous published data on patients with high-grade NETs [31, 32]. This confirms that patients with a high-grade tumour and sufficient somatostatin receptor expression may benefit from PRRT, as described in previous case reports [33,34,35]. In these patients, higher accumulated activities and an individualized protocol may be of special importance, and fractionation may partially explain improved tumour-to-background ratios as previously discussed [35]. The response rates in patients with a Ki-67 index >20% were higher than in those reported by Ezziddin et al., who aimed at four cycles of 7.9 GBq 177Lu-DOTATATE with an intended interval of 10 to 14 weeks [34]. Among their seven patients with a Ki-67 index >20%, only one had PR and SD (14%), respectively, while five patients (71%) progressed. In our study, 43.8% of patients received more than four (five to seven) cycles of 7.4 GBq with an intended interval of 6 to 8 weeks. PR was seen in 5 of 16 patients (31%) and SD in 69%, and no progression at first follow-up examination.
Few observations of a dose-response relationship in PRRT have been reported [36, 37]. To prescribe tumour doses in PRRT, as in external beam radiation, is not possible, but the present results indicate that the absorbed dose to the kidneys can serve as a substitute for tumour dose and the tolerance of the individual patient. Bodei et al. found a positive correlation between objective response and cumulative activity, that was in turn related to higher absorbed tumour doses [6].
The relationships among absorbed dose, objective tumour shrinkage and survival are not easy to determine in patients with NETs undergoing PRRT, since the time from the start of therapy to best response varies and can be several years [5], in our study up to 54 months. Based on best response, patients with CR or PR had a significantly longer OS than those with SD (Fig. 2). Kwekkeboom et al. found no significant difference in survival between patients with CR or PR and those with SD based on their radiological response 3 months after therapy [5], which may be attributable to the earlier time point for evaluation. In a recent update, the Rotterdam group have also reported longer survival in patients with CR or PR as best response than in those with SD [9]. On the other hand, we found no difference between these groups in terms of PFS. One explanation for this may be that at the time of progression, patients become amenable to further treatment after previous substantial tumour regression. An example of this is presented in Fig. 5 that shows the WBS findings in a patient with massive liver metastases of a VIPoma. After the first cycle of 177Lu-DOTA-octreotate, she developed a hormonal crisis with life-threatening diarrhoea requiring intensive care. After three cycles, vasoactive intestinal peptide levels normalized and the diarrhoea stopped completely. The best morphological result was a PR with a decrease by 45% according to RECIST 1.1 after cycle 5. By 40 months after the start of therapy, the tumour had progressed and salvage therapy was given with another two cycles. At this time-point, the tumour burden was still lower than at the start of therapy, and the patient’s general condition had improved. In the current series, 14 patients were able to receive salvage therapy, of whom 9 (64.2%) were alive at the time of analysis.

A 43-year-old female patient with VIPoma. a Cropped whole-body scans (WBS) obtained on day 1 after treatment with 177Lu-DOTA-octreotate during initial treatment (cycles 1–5) and salvage therapy. Note the change in size and uptake intensity of the different tumours throughout therapy. Imaging at the time of salvage therapy after progression shows new uptake in the skeleton, but the total tumour burden is still lower than at the start of therapy. b Absorbed organ doses (in absolute values and in relation to administered activity) to the kidneys, liver parenchyma and spleen , and to three representative tumour lesions with homogeneous uptake, measured in the same area during each cycle of initial treatment and during salvage therapy. c Layout of the dosimetry programme (implemented on a Hermes platform, Nuclear Diagnostics International AB). The hair cross is positioned on the metastatic uptake in the liver, the small circle corresponds to a 4-cm3 volume of interest (VOI). For tumour and solid organ dosimetry, calculations of absorbed doses were based on volume concentrations in small VOIs drawn on SPECT/CT images at three time-points (24 h, 4 days and 7 days after infusion). In this patient, three SPECT/CT scans were acquired during cycles 1, 2 and 4 and cycle 1 of salvage therapy. For the other cycles, one SPECT/CT scan was acquired at 24 h and the absorbed dose was calculated assuming unchanged kinetics from the previous therapy
There is a relationship between objective responses and decrease of tumour markers, which is in turn related to OS, and according to Khan et al. [38] is also associated with improvement in quality of life. In this study, decreases in tumour markers by more than 50% from increased baseline levels in 65% of 85 patients were associated with longer survival with a median OS of 60 months (95% CI 42 months, NR) versus 35 months (95% CI 17–52 months; p = 0.01). Furthermore, more patients in whom the absorbed dose to the kidneys reached 23 Gy showed a decrease in tumour markers.
In agreement with other studies, in the present study the objective response rate was lower in patients with SI-NETs than in those with other NETs [4, 14], but the survival rate was not lower (Tables 4 and 5, Fig. 1). In the present study, 24% of patients obtained an objective response (RECIST 1.1 CR/PR), with better results in those with pancreaticoduodenal NETs (42.9%) and rectal NETs (45.4%) than in those with SI-NETs (12%). In the NETTER-1 study, four cycles of 7.4 GBq 177Lu-DOTA-octreotate was compared with an increased dose of SSA in a group of patients with grade 1 and grade 2 SI-NETs, and a higher objective response rate with PRRT (18.8% versus 3%) was found with an estimated PFS rate of 65.2% (95% CI 50–76.8%) at 20 months [8]. This is comparable to 68% (95% CI 59–75%) found in the present study (parametric Weibull fit, supported by Kaplan-Meier analysis), despite the fact that 31.5% of the patients had increased doses of SSA on enrolment and risk factors such as liver and bone metastases being more frequent in our study (liver metastases 84% versus 97%, bone metastases 11% versus 49%). Table 8 compares patient groups with similar inclusion characteristics from the NETTER-1 study [8], the recent update from the Rotterdam group (table adapted from Brabander et al. [9]) and the present study.
We conclude that an absorbed dose of 23 Gy is generally well tolerated by all patients in whom this limit can be reached, regardless of the number of cycles. The only case of grade 4 nephrotoxicity observed was found to be related to hypertensive nephrosclerosis before this dose had been reached, at cumulative doses of 15.2 and 16 Gy to the right and left kidney, respectively. Therapy was stopped because of an increase of about 50% between cycle 1 and cycle 2, so that further damage was avoided. We interpreted this toxicity as primarily caused by the patient’s hypertension, but probably worsened by the treatment. A grade 2 kidney toxicity was seen in eight patients (4%) at the time of progression as part of general deterioration, and was probably unrelated to the treatment. and seven of these patients had cardiovascular risk factors and/or diabetes mellitus. On the other hand, risk factors for kidney toxicity (cardiovascular disease including arterial hypertension and diabetes mellitus) were present in 79 patients (39.5%), and in 43 of these patients (54%) the absorbed dose to the kidneys reached 23 Gy, with 37 of these 43 patients receiving more than four cycles (five to seven) without toxicity. This demonstrates that even in the presence of risk factors, the limit of 23 Gy to the kidneys is generally safe, and patients with risk factors need not automatically be excluded from the attempt to reach this goal with higher activities if they show clinical benefit. Kidney dosimetry can help reveal abnormal dose changes and levels and minimize damage. Figure 6 illustrates the range of absorbed doses to the kidneys that were observed per cycle and patient and the changes over time.

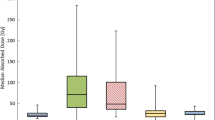
Absorbed doses to the kidneys in the first cycle (a, b) and the last cycle in each patient (cycles 2 to 10; c, d) during initial treatment. Throughout therapy, doses could decrease or increase. Shaded bars indicate patients who received an absorbed dose of 3 to 4 Gy to their right kidney in the first cycle (a). In their last cycle, absorbed doses to the right kidney varied between 2 and 6 Gy (c). Dose distributions in the left kidneys of the same patients correspond to shaded areas in b and d
Even higher cumulative absorbed doses to the kidneys (with maximum absorbed doses to the right and left kidney of 46.6 and 43.3 Gy, respectively) were reached in 14 patients (7%) who underwent retreatment without nephrotoxicity worse than grade 1. This implies that higher absorbed doses from 177Lu-DOTA-octreotate may be possible in patients without risk factors. The tolerability of higher biological effective doses (BED) to the kidneys is currently being studied [39]. The relationship between absorbed doses (as reported in the current study) and BED is discussed by Cremonesi et al. [40] and in a recent report from our group [41].
The Rotterdam protocol of four cycles of 7.4 GBq 177Lu-DOTA-octreotate has been widely accepted. In patients who received four cycles during initial treatment, those in whom the absorbed dose to the kidneys reached 23 Gy showed a significantly longer survival (median OS 60 months) than those in whom it did not (median OS 19 months, p < 0.0006; Fig. 4). The majority of patients in whom the dose to the kidneys did not reach 23 Gy had progression or bone marrow suppression. Still, the comparison implies that a cut-off defined by four cycles of 7.4 GBq will exclude patients who might benefit from further therapy. This view is supported by the finding that differences in survival between the patient groups could still be observed when patients who stopped treatment because of tumour progression or deterioration for other reasons were excluded. In the remaining patients therapy was stopped due to kidney dosimetry, slow bone marrow recovery without other complications, decrease in tumour burden and the patient’s wish to stop after four cycles (Table 3).
Although more than half of our patients had bone metastases, the morphological response rate was similar or superior to that in other studies (Table 7) and the subacute haematotoxicity was not higher in this group (Table 3). Unlike in other studies, the diagnosis of bone and bone marrow metastases was based on posttreatment scans during therapy, which has to be regarded as more sensitive than somatostatin receptor scintigraphy, and this may be one possible explanation for this high figure. Although in none of our patients was an absorbed dose of 2 Gy to the bone marrow reached, 22% had to stop therapy due to bone marrow-related events.
In agreement with others [22, 30, 40], we found a considerable interindividual variation in calculated bone marrow doses, and similar median values in patients with and without therapy-limiting bone marrow toxicity (Table 3). Although a correlation between absorbed dose and bone marrow toxicity has previously been shown by applying a dosimetry method based on planar imaging supported with SPECT/CT [42], our finding emphasizes that bone marrow dosimetry at the current state of our knowledge cannot be used to predict bone marrow toxicity in the individual patient. In line with the view of these authors, both their method and the method used in the current study will underestimate bone marrow doses in patients with bone marrow metastases. Also, the interindividual variation mentioned above will contribute to uncertainty in predicting toxicity.
The incidence of bone marrow malignancies in four patients (2%) is in line with reports from other centres [43]. Of previously documented risk factors, all had bone metastases and one had extensive liver metastases. Three patients (75%) had received the alkylating agent temozolomide, and one had also received streptozotocin. In this series, temozolomide is over-represented among patients with bone marrow malignancies despite the fact that streptozotocin (in combination with 5-fluorouracil) was the predominant alkylator used in 23.9% of all patients compared with 15.3% who had received temozolomide. This finding is an isolated observation and must be interpreted with caution. Still, as a comparatively new agent in the therapeutic arsenal of NETs, this toxicity should be observed more closely. As discussed by Bodei et al. [43], bone marrow malignancy is a fairly infrequent finding in larger PRRT series, even though one recent study showed a much higher incidence of bone marrow malignancies in a small group of heavily pretreated patients (20%, 4 of 20 patients) [44]. The present study, in line with several others, showed favourable tumour responses and survival data that compare well with alternative treatments. Especially in rectal NETs and bronchopulmonary carcinoids [23], the outcome is most encouraging.
In our opinion, this study provides important findings in favour of an individualized, dose-driven PRRT protocol. A prospective randomized study comparing the treatment protocol involving four cycles of 7.4 GBq of 177Lu-DOTA-octreotate with a protocol based on kidney dose might answer the question as to whether the observed superior outcome in patients in whom the absorbed dose to the kidneys reached 23 Gy was a result of optimization of the tumour dose or depended on individual patient and tumour characteristics.
Conclusion
Dosimetry-based planning of therapy with 177Lu-DOTA-octreotate is feasible. In the majority of patients (61.5%) the intended absorbed dose of 23 Gy to the kidneys was reached after three to nine cycles of 7.4 GBq 177Lu-DOTA-octreotate. In no patient was a cumulative dose of 2 Gy to the bone marrow reached. Bone marrow toxicity was in line with previous reports even though the majority of patients had bone marrow metastases and/or advanced disease. No major nephrotoxicity entirely related to the treatment was found, but 4% of patients developed grade 2 toxicity at the time of progression, and one patient (0.5%), later diagnosed with arteriosclerotic nephrosclerosis, developed grade 4 toxicity without the dose limit of 23 Gy to the kidneys having been reached. Patients in whom this absorbed dose was reached, had significantly longer PFS and OS, and significantly more patients obtained CR/PR as well as biochemical responses. Patients with CR/PR survived longer than those with SD.
References
Otte A, Mueller-Brand J, Dellas S, Nitzsche EU, Herrmann R, Maecke HR. Yttrium-90-labelled somatostatin-analogue for cancer treatment. Lancet. 1998;351(9100):417–8.
Otte A, Herrmann R, Heppeler A, Behe M, Jermann E, Powell P, et al. Yttrium-90 DOTATOC: first clinical results. Eur J Nucl Med. 1999;26(11):1439–47.
Kwekkeboom DJ, Teunissen JJ, Bakker WH, Kooij PP, de Herder WW, Feelders RA, et al. Radiolabeled somatostatin analog [177Lu-DOTA0,Tyr3]octreotate in patients with endocrine gastroenteropancreatic tumors. J Clin Oncol. 2005;23(12):2754–62.
Kwekkeboom DJ, Mueller-Brand J, Paganelli G, Anthony LB, Pauwels S, Kvols LK, et al. Overview of results of peptide receptor radionuclide therapy with 3 radiolabeled somatostatin analogs. J Nucl Med. 2005;46(Suppl 1):62S–6S.
Kwekkeboom DJ, de Herder WW, Kam BL, van Eijck CH, van Essen M, Kooij PP, et al. Treatment with the radiolabeled somatostatin analog [177Lu-DOTA 0,Tyr3]octreotate: toxicity, efficacy, and survival. J Clin Oncol. 2008;26(13):2124–30. https://doi.org/10.1200/JCO.2007.15.2553.
Bodei L, Cremonesi M, Grana CM, Fazio N, Iodice S, Baio SM, et al. Peptide receptor radionuclide therapy with (177)Lu-DOTATATE: the IEO phase I-II study. Eur J Nucl Med Mol Imaging. 2011;38(12):2125–35. https://doi.org/10.1007/s00259-011-1902-1.
Ezziddin S, Attassi M, Yong-Hing CJ, Ahmadzadehfar H, Willinek W, Grunwald F, et al. Predictors of long-term outcome in patients with well-differentiated gastroenteropancreatic neuroendocrine tumors after peptide receptor radionuclide therapy with 177Lu-octreotate. J Nucl Med. 2014;55(2):183–90. https://doi.org/10.2967/jnumed.113.125336.
Strosberg J, El-Haddad G, Wolin E, Hendifar A, Yao J, Chasen B, et al. Phase 3 trial of 177Lu-Dotatate for midgut neuroendocrine tumors. N Engl J Med. 2017;376(2):125–35. https://doi.org/10.1056/NEJMoa1607427.
Brabander T, van der Zwan WA, Teunissen JJM, Kam BLR, Feelders RA, de Herder WW, et al. Long-term efficacy, survival, and safety of [177Lu-DOTA0,Tyr3]octreotate in patients with gastroenteropancreatic and bronchial neuroendocrine tumors. Clin Cancer Res. 2017;23(16):4617–24. https://doi.org/10.1158/1078-0432.CCR-16-2743.
Valkema R, Pauwels S, Kvols LK, Barone R, Jamar F, Bakker WH, et al. Survival and response after peptide receptor radionuclide therapy with [90Y-DOTA0,Tyr3]octreotide in patients with advanced gastroenteropancreatic neuroendocrine tumors. Semin Nucl Med. 2006;36(2):147–56.
Valkema R, Pauwels SA, Kvols LK, Kwekkeboom DJ, Jamar F, de Jong M, et al. Long-term follow-up of renal function after peptide receptor radiation therapy with (90)Y-DOTA(0),Tyr(3)-octreotide and (177)Lu-DOTA(0),Tyr(3)-octreotate. J Nucl Med. 2005;46(Suppl 1):83S–91S.
Bushnell DL Jr, O'Dorisio TM, O'Dorisio MS, Menda Y, Hicks RJ, Van Cutsem E, et al. 90Y-edotreotide for metastatic carcinoid refractory to octreotide. J Clin Oncol. 2010;28(10):1652–9.
Cwikla JB, Sankowski A, Seklecka N, Buscombe JR, Nasierowska-Guttmejer A, Jeziorski KG, et al. Efficacy of radionuclide treatment DOTATATE Y-90 in patients with progressive metastatic gastroenteropancreatic neuroendocrine carcinomas (GEP-NETs): a phase II study. Ann Oncol. 2010;21(4):787–94. https://doi.org/10.1093/annonc/mdp372.
Imhof A, Brunner P, Marincek N, Briel M, Schindler C, Rasch H, et al. Response, survival, and long-term toxicity after therapy with the radiolabeled somatostatin analogue [90Y-DOTA]-TOC in metastasized neuroendocrine cancers. J Clin Oncol. 2011;29(17):2416–23.
Sandstrom M, Garske U, Granberg D, Sundin A, Lundqvist H. Individualized dosimetry in patients undergoing therapy with (177)Lu-DOTA-D-Phe(1)-Tyr(3)-octreotate. Eur J Nucl Med Mol Imaging. 2010;37(2):212–25. https://doi.org/10.1007/s00259-009-1216-8.
Garske U, Sandstrom M, Johansson S, Sundin A, Granberg D, Eriksson B, et al. Minor changes in effective half-life during fractionated (177)Lu-Octreotate therapy. Acta Oncol. 2012;51(1):86–96. https://doi.org/10.3109/0284186X.2011.618511.
Sandstrom M, Garske-Roman U, Granberg D, Johansson S, Widstrom C, Eriksson B, et al. Individualized dosimetry of kidney and bone marrow in patients undergoing 177Lu-DOTA-octreotate treatment. J Nucl Med. 2013;54(1):33–41.
Garkavij M, Nickel M, Sjogreen-Gleisner K, Ljungberg M, Ohlsson T, Wingardh K, et al. 177Lu-[DOTA0,Tyr3] octreotate therapy in patients with disseminated neuroendocrine tumors: analysis of dosimetry with impact on future therapeutic strategy. Cancer. 2010;116(4 Suppl):1084–92. https://doi.org/10.1002/cncr.24796.
Sward C, Bernhardt P, Ahlman H, Wangberg B, Forssell-Aronsson E, Larsson M, et al. [177Lu-DOTA 0-Tyr 3]-octreotate treatment in patients with disseminated gastroenteropancreatic neuroendocrine tumors: the value of measuring absorbed dose to the kidney. World J Surg. 2010;34(6):1368–72. https://doi.org/10.1007/s00268-009-0387-6.
Larsson M, Bernhardt P, Svensson JB, Wangberg B, Ahlman H, Forssell-Aronsson E. Estimation of absorbed dose to the kidneys in patients after treatment with 177Lu-octreotate: comparison between methods based on planar scintigraphy. EJNMMI Res. 2012;2(1):49. https://doi.org/10.1186/2191-219X-2-49.
Barone R, Borson-Chazot F, Valkema R, Walrand S, Chauvin F, Gogou L, et al. Patient-specific dosimetry in predicting renal toxicity with (90)Y-DOTATOC: relevance of kidney volume and dose rate in finding a dose-effect relationship. J Nucl Med. 2005;46(Suppl 1):99S–106S.
Bodei L, Kidd M, Paganelli G, Grana CM, Drozdov I, Cremonesi M, et al. Long-term tolerability of PRRT in 807 patients with neuroendocrine tumours: the value and limitations of clinical factors. Eur J Nucl Med Mol Imaging. 2015;42(1):5–19. https://doi.org/10.1007/s00259-014-2893-5.
Mariniello A, Bodei L, Tinelli C, Baio SM, Gilardi L, Colandrea M, et al. Long-term results of PRRT in advanced bronchopulmonary carcinoid. Eur J Nucl Med Mol Imaging. 2016;43(3):441–52. https://doi.org/10.1007/s00259-015-3190-7.
Bodei L, Cremonesi M, Ferrari M, Pacifici M, Grana CM, Bartolomei M, et al. Long-term evaluation of renal toxicity after peptide receptor radionuclide therapy with 90Y-DOTATOC and 177Lu-DOTATATE: the role of associated risk factors. Eur J Nucl Med Mol Imaging. 2008;35(10):1847–56. https://doi.org/10.1007/s00259-008-0778-1.
Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, et al. Tolerance of normal tissue to therapeutic irradiation. Int J Radiat Oncol Biol Phys. 1991;21(1):109–22.
Konijnenberg M, Melis M, Valkema R, Krenning E, de Jong M. Radiation dose distribution in human kidneys by octreotides in peptide receptor radionuclide therapy. J Nucl Med. 2007;48(1):134–42.
Eberlein U, Cremonesi M, Lassmann M. Individualized dosimetry for theranostics: necessary, nice to have, or counterproductive? J Nucl Med. 2017;58(Suppl 2):97S–103S. https://doi.org/10.2967/jnumed.116.186841.
Benua RS, Cicale NR, Sonenberg M, Rawson RW. The relation of radioiodine dosimetry to results and complications in the treatment of metastatic thyroid cancer. Am J Roentgenol Radium Ther Nucl Med. 1962;87:171–82.
Eisenhauer EA, Therasse P, Bogaerts J, Schwartz LH, Sargent D, Ford R, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45(2):228–47.
Krenning EP, de Jong M, Kooij PP, Breeman WA, Bakker WH, de Herder WW, et al. Radiolabelled somatostatin analogue(s) for peptide receptor scintigraphy and radionuclide therapy. Ann Oncol. 1999;10(Suppl 2):S23–9.
Sorbye H, Strosberg J, Baudin E, Klimstra DS, Yao JC. Gastroenteropancreatic high-grade neuroendocrine carcinoma. Cancer. 2014;120(18):2814–23. https://doi.org/10.1002/cncr.28721.
Sorbye H, Welin S, Langer SW, Vestermark LW, Holt N, Osterlund P, et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): the NORDIC NEC study. Ann Oncol. 2013;24(1):152–60.
Fazio N, Grana C, Pelosi G, Torrisi R, Di Meglio G, Tradati N, et al. Successful chemotherapy and 90Y-DOTATOC in a patient with mediastinal highly aggressive neuroendocrine carcinoma. Acta Oncol. 2006;45(5):627–9.
Ezziddin S, Opitz M, Attassi M, Biermann K, Sabet A, Guhlke S, et al. Impact of the Ki-67 proliferation index on response to peptide receptor radionuclide therapy. Eur J Nucl Med Mol Imaging. 2011;38(3):459–66. https://doi.org/10.1007/s00259-010-1610-2.
Garske U, Sandström M, Johansson S, Granberg D, Lundqvist H, Lubberink M, et al. Lessons on tumour response: imaging during therapy with 177Lu-DOTA-octreotate. A case report on a patient with a large volume of poorly differentiated neuroendocrine carcinoma. Theranostics. 2012;2(5):459–71.
Pauwels S, Barone R, Walrand S, Borson-Chazot F, Valkema R, Kvols LK, et al. Practical dosimetry of peptide receptor radionuclide therapy with (90)Y-labeled somatostatin analogs. J Nucl Med. 2005;46(Suppl 1):92S–8S.
Ilan E, Sandstrom M, Wassberg C, Sundin A, Garske-Roman U, Eriksson B, et al. Dose response of pancreatic neuroendocrine tumours treated with peptide receptor radionuclide therapy using 177Lu-DOTATATE. J Nucl Med. 2015;56(2):177–82. https://doi.org/10.2967/jnumed.114.148437.
Khan S, Krenning EP, van Essen M, Kam BL, Teunissen JJ, Kwekkeboom DJ. Quality of life in 265 patients with gastroenteropancreatic or bronchial neuroendocrine tumors treated with [177Lu-DOTA0,Tyr3]octreotate. J Nucl Med. 2011;52(9):1361–8.
Sundlov A, Sjogreen-Gleisner K, Svensson J, Ljungberg M, Olsson T, Bernhardt P, et al. Individualised 177Lu-DOTATATE treatment of neuroendocrine tumours based on kidney dosimetry. Eur J Nucl Med Mol Imaging. 2017;44(9):1480–9. https://doi.org/10.1007/s00259-017-3678-4.
Cremonesi M, Botta F, Di Dia A, Ferrari M, Bodei L, De Cicco C, et al. Dosimetry for treatment with radiolabelled somatostatin analogues. A review. Q J Nucl Med Mol Imaging. 2010;54(1):37–51.
Sandstrom M, Garske-Roman U, Johansson S, Granberg D, Sundin A, Freedman N. Kidney dosimetry during 177Lu-DOTATATE therapy in patients with neuroendocrine tumors: aspects on calculation and tolerance. Acta Oncol. 2017. https://doi.org/10.1080/0284186X.2017.1378431.
Svensson J, Ryden T, Hagmarker L, Hemmingsson J, Wangberg B, Bernhardt P. A novel planar image-based method for bone marrow dosimetry in (177)Lu-DOTATATE treatment correlates with haematological toxicity. EJNMMI Phys. 2016;3(1):21. https://doi.org/10.1186/s40658-016-0157-0.
Bodei L, Modlin IM, Luster M, Forrer F, Cremonesi M, Hicks RJ, et al. Myeloid neoplasms after chemotherapy and PRRT: myth and reality. Endocr Relat Cancer. 2016;23(8):C1–7. https://doi.org/10.1530/ERC-16-0258.
Brieau B, Hentic O, Lebtahi R, Palazzo M, Ben Reguiga M, Rebours V, et al. High risk of myelodysplastic syndrome and acute myeloid leukemia after 177Lu-octreotate PRRT in NET patients heavily pretreated with alkylating chemotherapy. Endocr Relat Cancer. 2016;23(5):L17–23. https://doi.org/10.1530/ERC-15-0543.
Acknowledgements
We are grateful to Prof. Eric Krenning for generously supplying the peptide. We are indebted to Dr. Hanna Mäenpää, Prof. Dermot O’Toole, Dr. Mona-Elisabeth Revheim and Dr. Espen Thiis-Evensen for their invaluable help with data collection, and to the staff in the Department of Endocrine Oncology and the Department of Nuclear Medicine at Uppsala University Hospital for their skilful and relentless work.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
The study was entirely conducted by Uppsala University; no other funding was received.
Conflicts of interest
One of the authors (A.S.) is advisor to Advanced Accelerator Applications, France. All other authors declare no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Garske-Román, U., Sandström, M., Fröss Baron, K. et al. Prospective observational study of 177Lu-DOTA-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (NETs): feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity. Eur J Nucl Med Mol Imaging 45, 970–988 (2018). https://doi.org/10.1007/s00259-018-3945-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-018-3945-z