
Abstract
Purpose
Perfusion gated single photon emission computed tomography (SPECT) can assess with good reproducibility left ventricular (LV) volumes and ejection fraction (EF). Whether this reproducibility is maintained in long-term follow-up is unknown.
Methods
We compared LV end-diastolic (ED) and end-systolic (ES) volumes (V) as well as EF calculated using gated SPECT and QGS software in 103 coronary artery disease patients studied twice at > 1-year interval because of standard clinical indications. Patients were divided into two groups: (A) 67 patients without major clinical changes and with stable resting perfusion and (B) 36 with modified clinical status or resting perfusion.
Results
The relationship between gated SPECT 2 EF (=y) and gated SPECT 1 EF (=x) was for group A: y = 0.91 x + 5.34, r = 0.92, p < 0.0001, SEE=4 and for group B: y = 0.67 x + 13.6, r = 0.63, p < 0.0001, SEE=10. The 95% limit of agreement was 8 EF units for group A and 20.6 EF units for group B. For EDV, the 95% limit of agreement was 22 ml for group A and 52 ml for group B. For ESV, the 95% limit of agreement was 13 ml for group A and 44 ml for group B.
Conclusion
In stable patients with an unmodified resting perfusion pattern the functional parameters derived from perfusion gated SPECT have good reproducibility even after a prolonged time interval. This supports the value of gated SPECT for serial evaluations of LV function.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Perfusion gated single photon emission computed tomography (SPECT) is currently regarded as a reliable method for the measurement of left ventricular (LV) ejection fraction (EF) [1–5]. Although differences as compared to more precise modalities exist, the feasibility and robustness of gated SPECT EF are well known [6–12]. Most recently, a study on a large patient population demonstrated the good agreement between resting and post-stress gated SPECT EF with the corresponding measures obtained by equilibrium radionuclide angiocardiography [13]. Moreover, the gated SPECT EF has been demonstrated to be reproducible in repeated acquisitions during the same session or in studies performed few days apart [14–20]. This has opened the way to the use of gated SPECT for the serial assessment of LV function in various clinical settings [21–23]. On the other hand, in the single study that examined the repeatability of EF and volume measurements at a 1-year interval the limits of agreement appear wider, making the detection of serial changes uncertain [24]. The aim of the present study was to verify the differences in resting LV function assessed by gated SPECT using the same hardware and software in coronary artery disease patients who underwent two separate studies after a long time interval, taking into account not only the intervening changes in clinical status, but also the modifications in the resting perfusion pattern.
Materials and methods
Patient population and study protocol
We identified in our archives the patients who had undergone two separate perfusion gated SPECT studies in our laboratory between April 2003 and June 2009. We considered only the patients who had performed the study with the same dual day imaging protocol and on the same gamma camera in both occurrences and for whom clinical data and original image files were available and complete. After all data had been retrieved, clinical information was examined and tabulated, with particular attention to the occurrence of major events or clinical changes between the two studies (acute myocardial infarction, coronary artery bypass grafting, percutaneous clinical intervention, stable left bundle branch block, important variations in medical therapy). The raw gated SPECT studies of the patients were newly processed by an experienced observer unaware of the patient’s identity and of image sequence. We excluded from analysis the patients with atrial fibrillation or severe arrhythmias that prevented a reliable gating in at least one of the two studies. Patients with major image artefacts that precluded the automatic definition of LV borders by the processing software were excluded as well. The study was approved by the Ethics Committee of our Institution.
Gated SPECT
For the purpose of the study we considered only the resting gated SPECT of the dual day protocol. Gated SPECT was acquired 1 h after the injection at rest of 740 MBq of 99mTc-sestamibi, using a dual-head gamma camera (Skylight, Philips, Milpitas, CA, USA) equipped with high-resolution collimators and using a 15% window centred on the 140-keV photopeak of 99mTc. SPECT was acquired in step-and-shoot mode using a 180° elliptical orbit, matrix size 64 × 64, with 32 projections and 60 s/projection, 8 frames/cardiac cycle. The studies were reconstructed using filtered backprojection without attenuation or scatter correction and realigned along the heart axis. Regional myocardial perfusion was assessed visually by one blinded experienced observer (V.B.), unaware of the patient’s data and image sequence, and scored using a 5-point scale (0=normal, 1=mildly reduced, 2=moderately reduced, 3=severely reduced, 4=absent uptake) [25]. The summed rest score (SRS) was obtained by adding the scores of the 20 segments in resting images and was considered to be normal if it was ≤ 3 [17, 26]. LV end-diastolic and end-systolic volumes were automatically calculated using the QGS program and EF was derived from the LV volumes as usual [1].
Statistical analysis
Continuous variables are expressed as mean ± standard deviation or as median (25th, 75th percentile) as appropriate. The comparisons within groups were performed with Student’s t test for paired samples or the Wilcoxon non-parametric test as appropriate. The comparisons between groups were performed with Student’s t test for independent samples or the Mann-Whitney U test as appropriate. The comparison of proportion was made using Fisher’s exact test. The agreement between the two LVEF measurements was assessed using linear regression analysis and the Bland-Altman analysis. A p value < 0.05 was considered statistically significant.
Results
General findings
During the considered time interval a total of 121 patients had performed two separate rest-stress perfusion gated SPECT studies. Of them, 111 fulfilled the inclusion criteria of completely retrievable clinical information and data files. After data recovery, six patients were excluded from data analysis because of atrial fibrillation or severe arrhythmias during one or both acquisitions. Finally, there were two additional patients who had to be excluded because the automated processing procedure was impossible owing to bad image quality or major extracardiac activity. Therefore, the final study cohort included 103 patients (22 women, mean age: 63.6 ± 8.1 years, range: 40–81). The SRS of the entire study group in first gated SPECT was 0 (0, 5), and the same value was registered in the second gated SPECT (NS). We divided the patient population into two groups. Group A included 67 patients in whom (1) there had been no major clinical events as defined above between the first and the second gated SPECT and (2) the SRS was normal in gated SPECT 1, with a maximal SRS difference ≤ 2 in gated SPECT 2, or was abnormal but unchanged in the two gated SPECT. Group B included the remaining 36 patients. Table 1 summarizes the demographic and clinical features of the patient population. The SRS values within the two groups, reported in the table, did not change significantly between the first and the second gated SPECT. Table 2 describes the changes between the two gated SPECT in group B patients.
LVEF reproducibility
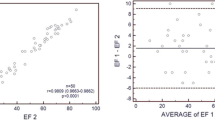
In the whole patient population the mean EF in the two resting gated SPECT studies was not significantly different (55.1 ± 13 vs 54.6 ± 13.5%, p = 0.49). According to linear regression analysis, in group A the relationship between gated SPECT 2 EF (=y) and gated SPECT 1 EF (=x) was: y = 0.91 x + 5.34, correlation coefficient=0.92, p < 0.0001, SEE=4 (Fig. 1). In group B, the corresponding relationship was: y = 0.67 x + 13.6, correlation coefficient=0.63, p < 0.0001, SEE=10 (Fig. 2). Using the Bland-Altman analysis, the 95% limit of agreement was 8 EF units for group A and 20.6 EF units for group B (Fig. 3).

Scatterplot of LVEF in gated SPECT 1 (x-axis) vs LVEF in gated SPECT 2 (y-axis) in group A. The dashed line represents the line of identity

Scatterplot of LVEF in gated SPECT 1 (x-axis) vs LVEF in gated SPECT 2 (y-axis) in group B. The dashed line represents the line of identity

Bland-Altman analysis of agreement for resting EF between gated SPECT 1 and 2. Group A is represented by closed circles and solid lines, group B by open circles and dashed lines, thick line mean difference, thin lines 95% limits of agreement
Reproducibility of LV volumes
In the whole patient population the mean end-diastolic volume (EDV) and the mean end-systolic volume (ESV) in the two resting gated SPECT studies were not significantly different (105 ± 49 vs 103 ± 50 ml, p = 0.23, and 52 ± 44 vs 52 ± 46 ml, p = 0.97, respectively). According to linear regression analysis, in group A the relationship between gated SPECT 2 EDV (=y) and gated SPECT 1 EDV (=x) was: y = 0.97 x –0.7, correlation coefficient=0.95, p < 0.0001, SEE=11 ml. In group B, the corresponding relationship was: y = 0.9 x + 12.3, correlation coefficient=0.91, p < 0.0001, SEE=26 ml. Using the Bland-Altman analysis, the 95% limit of agreement was 22 ml for group A and 52 ml for group B (Fig. 4). As regards ESV, in group A the relationship between gated SPECT 2 (=y) and gated SPECT 1 ESV (=x) was: y=1.046 x –3.14, correlation coefficient=0.97, p < 0.0001, SEE=7 ml. In group B, the corresponding relationship was: y = 0.92 x + 8.3, correlation coefficient=0.93, p < 0.0001, SEE=22 ml. Using the Bland-Altman analysis, the 95% limit of agreement was 13 ml for group A and 44 ml for group B (Fig. 5).

Bland-Altman analysis of agreement for resting EDV between gated SPECT 1 and 2. Same symbols as in Fig. 3

Bland-Altman analysis of agreement for resting ESV between gated SPECT 1 and 2. Same symbols as in Fig. 3
Discussion
It is well known that the EF assessment by gated SPECT is a robust measurement, which for instance is relatively unaffected by gating errors caused by arrhythmias [27, 28]. Therefore, the good reproducibility of EF in serial gated SPECT acquisitions is not surprising and the limits of agreement are constantly reported to range approximately from 5 to 7 EF units [14–18]. As regards the day-to-day variability, De Winter et al. examined 20 patients with LV dysfunction (EF < 40%) and confirmed the same reproducibility, with 95% limits of agreement of 6 EF units and of 20 ml for both EDV and ESV [19]. The authors concluded that gated SPECT can be used for the follow-up of global LV function in these patients. On the other hand, in the single study comparing the repeatability of functional data in two gated SPECT acquired at approximately a 1-year interval in patients without apparent changes in clinical status, Thorley and Smith found less satisfactory values, concluding that the repeatability of EF is acceptable but that of LV volumes is too low for a clinical use in patient follow-up [24]. However, their results are quite difficult to interpret, because the data reported in the tables apparently do not coincide with those in the Bland-Altman plots, with the latter showing wider 95% limits of agreement [24]. It appears therefore still unclear whether gated SPECT is suitable or not for identifying clinically important EF and LV volume changes in long-term follow-up.
We performed a retrospective analysis of more than 100 patients studied twice with perfusion gated SPECT at our institution. The main finding of our study is that the resting EF and LV volume measurements by gated SPECT have a satisfactory repeatability in patients in stable clinical conditions and with unchanged resting perfusion, even if they are studied at an interval of more than 2 years. Conversely, patients re-examined after important clinical changes or in whom resting perfusion is significantly modified show a wide variability.
There are various implications of our findings. First, we confirm that the good reproducibility of gated SPECT functional data is an intrinsic feature of this technique that is maintained over a prolonged time span and is not remarkably influenced by other conditions, given that the perfusion pattern is stable and that there are no differences in the acquisition details. The good reproducibility of baseline resting LV EF and volumes implies that the recognition of unexpected changes over a relatively narrow threshold should prompt for the search of otherwise undetected abnormalities. Therefore, the availability of comparable resting functional values would be an additional value of gated SPECT perfusion scintigraphy in patients with chronic coronary artery disease. With regard to this point, a recent study suggests that EF values are interchangeable because major post-stress variations are seldom registered [29]. However, Verberne et al. had already demonstrated that ischaemia is related to larger differences between resting and post-stress EF [18]. Accordingly, the value of the comparison between resting and post-stress EF to identify the presence of ischaemic stunning has been extensively demonstrated [30–32]. The possibility to perform a reliable serial evaluation of LV function using gated SPECT would discourage the use of post-stress EF as a surrogate for resting EF.
Finally, taking into account the current scenario of close competition among the various imaging modalities and of extreme cost consciousness, the demonstration that gated SPECT functional data that can be obtained without additional expenses during perfusion assessment are both robust and highly reproducible could contribute to reinforce the role of nuclear cardiology in various clinical settings [23]. In general, the reproducibility of functional parameters assessed by the other imaging modalities, such as cardiac magnetic resonance, three-dimensional echocardiography and multislice computed tomography, does not appear clearly superior to that of gated SPECT [19, 33–35]. Furthermore, there are no available data about the long-term repeatability of LV functional measurements using those techniques to be compared with the results of the present study. Interestingly, in a most recent report comparing two separate cardiac magnetic resonance exams at an interval of approximately 2 months, the EF coefficient of variability was very similar to our data [36]. Therefore, although it is clear that the radiation burden of gated SPECT must be taken into account, the repeatability of functional measurements after a very prolonged time interval is certainly an additional value of this modality.
Some limitations of the present study must be considered. The study is retrospective and the patient selection could not be planned. Therefore, the criteria used to differentiate the patients with from those without anticipated EF changes are imperfect. However, it is reasonable to suppose that a more precise definition of unchanged functional status would reduce the number of eligible patients but also improve the reproducibility of gated SPECT measurements. The number of patients with SRS changes (group B) is too small to evaluate whether there is a correlation between differences in resting perfusion and in LV function from gated SPECT 1 to gated SPECT 2. Similarly, because of the relatively small patient population, we could not perform a reasonable separate analysis on specific subgroups, such as women or patients with depressed LV function. As regards this latter point, however, the visual analysis of the Bland-Altman plot does not show any trend towards a different behaviour in patients with low EF, independently of the group to which they belong. Studies on wider patient populations are probably needed to identify the relationship between type and degree of perfusion changes, including variations in ischaemic burden and functional modifications. Our data are based on a single processing software. Therefore, the same comparison using other programs would be desirable. We used 8-frame gated SPECT for EF measurement. Although the higher precision of 16-frame gated SPECT has been advocated and recently confirmed [13], there are enough data to support the opinion that 8 intervals are adequate for most clinical purposes, and therefore are the most widely used modality [1, 17–19, 24, 37, 38].
Conclusion
This study demonstrates that the functional parameters derived from perfusion gated SPECT have a good reproducibility even after prolonged time intervals in patients with stable clinical conditions and unmodified resting perfusion pattern. Therefore, the use of gated SPECT for long-term serial evaluations of LV function should be considered reliable and this represents an important additional value of this imaging modality.
References
Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med 1995;36:2138–47.
Cullom SJ, Case JA, Bateman TM. Electrocardiographically gated myocardial perfusion SPECT: technical principles and quality control considerations. J Nucl Cardiol 1998;5:418–25.
Paul AK, Nabi HA. Gated myocardial perfusion SPECT: basic principles, technical aspects, and clinical applications. J Nucl Med Technol 2004;32:179–87.
Sciagrà R, Leoncini M. Gated single-photon emission computed tomography. The present-day “one-stop-shop” for cardiac imaging. Q J Nucl Med Mol Imaging 2005;49:19–29.
Abidov A, Germano G, Hachamovitch R, Berman DS. Gated SPECT in assessment of regional and global left ventricular function: major tool of modern nuclear imaging. J Nucl Cardiol 2006;13:261–79.
Gunning MG, Anagnostopoulos C, Davies G, Forbat SM, Ell PJ, Underwood SR. Gated technetium-99m-tetrofosmin SPECT and cine MRI to assess left ventricular contraction. J Nucl Med 1997;38:438–42.
Manrique A, Faraggi M, Véra P, Vilain D, Lebtahi R, Cribier A, et al. 201Tl and 99mTc-MIBI gated SPECT in patients with large perfusion defects and left ventricular dysfunction: comparison with equilibrium radionuclide angiography. J Nucl Med 1999;40:805–9.
Cwajg E, Cwajg J, He ZX, Hwang WS, Keng F, Nagueh SF, et al. Gated myocardial perfusion tomography for the assessment of left ventricular function and volumes: comparison with echocardiography. J Nucl Med 1999;40:1857–65.
Tadamura E, Kudoh T, Motooka M, Inubushi M, Shirakawa S, Hattori N, et al. Assessment of regional and global left ventricular function by reinjection Tl-201 and rest Tc-99m sestamibi ECG-gated SPECT: comparison with three-dimensional magnetic resonance imaging. J Am Coll Cardiol 1999;33:991–7.
Bavelaar-Croon CD, Kayser HW, van der Wall EE, de Roos A, Dibbets-Schneider P, Pauwels EK, et al. Left ventricular function: correlation of quantitative gated SPECT and MR imaging over a wide range of values. Radiology 2000;217:572–5.
Nakajima K, Higuchi T, Taki J, Kawano M, Tonami N. Accuracy of ventricular volume and ejection fraction measured by gated myocardial SPECT: comparison of 4 software programs. J Nucl Med 2001;42:1571–8.
Schaefer WM, Lipke CS, Standke D, Kühl HP, Nowak B, Kaiser HJ, et al. Quantification of left ventricular volumes and ejection fraction from gated 99mTc-MIBI SPECT: MRI validation and comparison of the Emory Cardiac Tool Box with QGS and 4D-MSPECT. J Nucl Med 2005;46:1256–63.
Acampa W, Caprio MG, Nicolai E, Liuzzi R, De Luca S, Capasso E, et al. Assessment of poststress left ventricular ejection fraction by gated SPECT: comparison with equilibrium radionuclide angiocardiography. Eur J Nucl Med Mol Imaging 2010;37:349–56.
Lee DS, Cheon GJ, Ahn JY, Chung JK, Lee MC. Reproducibility of assessment of myocardial function using gated 99Tc(m)-MIBI SPECT and quantitative software. Nucl Med Commun 2000;21:1127–34.
Lee DS, Ahn JY, Kim SK, Oh BH, Seo JD, Chung JK, et al. Limited performance of quantitative assessment of myocardial function by thallium-201 gated myocardial single-photon emission tomography. Eur J Nucl Med 2000;27:185–91.
Huyn IY, Kwan J, Park KS, Lee WH. Reproducibility of Tl-201 and Tc-99m sestamibi gated myocardial perfusion SPECT measurement of myocardial function. J Nucl Cardiol 2001;8:182–7.
Vallejo E, Chaya H, Plancarte G, Victoria D, Bialostozky D. Variability of serial same-day left ventricular ejection fraction using quantitative gated SPECT. J Nucl Cardiol 2002;9:377–84.
Verberne HJ, Dijkgraaf MG, Somsen GA, van Eck-Smit BL. Stress-related variations in left ventricular function as assessed with gated myocardial perfusion SPECT. J Nucl Cardiol 2003;10:456–63.
De Winter O, De Bondt P, Van De Wiele C, De Backer G, Dierckx RA, De Sutter J. Day-to-day variability of global left ventricular functional and perfusional measurements by quantitative gated SPECT using Tc-99m tetrofosmin in patients with heart failure due to coronary artery disease. J Nucl Cardiol 2004;11:47–52.
Nakajima K, Nishimura T. Inter-institution preference-based variability of ejection fraction and volumes using quantitative gated SPECT with 99mTc-tetrofosmin: a multicentre study involving 106 hospitals. Eur J Nucl Med Mol Imaging 2006;33:127–33.
Fukuchi K, Yasumura Y, Kiso K, Hayashida K, Miyatake K, Ishida Y. Gated myocardial SPECT to predict response to beta-blocker therapy in patients with idiopathic dilated cardiomyopathy. J Nucl Med 2004;45:527–31.
Sciagrà R, Giaccardi M, Porciani MC, Colella A, Michelucci A, Pieragnoli P, et al. Myocardial perfusion imaging using gated SPECT in heart failure patients undergoing cardiac resynchronization therapy. J Nucl Med 2004;45:164–8.
Sciagrà R. The expanding role of left ventricular functional assessment using gated myocardial perfusion SPECT: the supporting actor is stealing the scene. Eur J Nucl Med Mol Imaging 2007;34:1107–22.
Thorley PJ, Smith JM. Repeatability of left ventricular ejection fraction and volume measurement for 99mTc-tetrofosmin gated single photon emission computed tomography (SPECT). Nucl Med Commun 2005;26:345–9.
Hachamovitch R, Berman DS, Shaw LJ, Kiat H, Cohen I, Cabico JA, et al. Incremental prognostic value of myocardial perfusion single photon emission computed tomography for the prediction of cardiac death: differential stratification for risk of cardiac death and myocardial infarction. Circulation 1998;97:535–43.
Germano G, Erel J, Lewin H, Kavanagh PB, Berman DS. Automatic quantitation of regional myocardial wall motion and thickening from gated technetium-99m sestamibi myocardial perfusion single-photon emission computed tomography. J Am Coll Cardiol 1997;30:1360–7.
Nichols K, Dorbala S, DePuey EG, Yao SS, Sharma A, Rozanski A. Influence of arrhythmias on gated SPECT myocardial perfusion and function quantification. J Nucl Med 1999;40:924–34.
Nichols K, Yao SS, Kamran M, Faber TL, Cooke CD, DePuey EG. Clinical impact of arrhythmias on gated SPECT cardiac myocardial perfusion and function assessment. J Nucl Cardiol 2001;8:19–30.
Ramakrishna G, Miller TD, Hodge DO, O’Connor MK, Gibbons RJ. Differences in left ventricular ejection fraction and volumes measured at rest and poststress by gated sestamibi SPECT. J Nucl Cardiol 2006;13:668–74.
Johnson LL, Verdesca SA, Aude WY, Xavier RC, Nott LT, Campanella MW, et al. Postischemic stunning can affect left ventricular ejection fraction and regional wall motion on post-stress gated sestamibi tomograms. J Am Coll Cardiol 1997;30:1641–8.
Toba M, Kumita S, Cho K, Ibuki C, Kumazaki T, Takano T. Usefulness of gated myocardial perfusion SPECT imaging soon after exercise to identify postexercise stunning in patients with single-vessel coronary artery disease. J Nucl Cardiol 2004;11:697–703.
Hida S, Chikamori T, Tanaka H, Usui Y, Igarashi Y, Nagao T, et al. Diagnostic value of left ventricular function after stress and at rest in the detection of multivessel coronary artery disease as assessed by electrocardiogram-gated SPECT. J Nucl Cardiol 2007;14:68–74.
Nosir YFM, Lequin MH, Kasprzak JD, van Domburg RT, Vletter WB, Yao J, et al. Measurements and day-to-day variabilities of left ventricular volumes and ejection fraction by three-dimensional echocardiography and comparison with magnetic resonance imaging. Am J Cardiol 1998;82:209–14.
Sugeng L, Mor-Avi V, Weinert L, Niel J, Ebner C, Steringer-Mascherbauer R, et al. Quantitative assessment of left ventricular size and function: side-by-side comparison of real-time three-dimensional echocardiography and computed tomography with magnetic resonance reference. Circulation 2006;114:654–61.
Soliman OI, Kirschbaum SW, van Dalen BM, van der Zwaan HB, Mahdavian Delavary B, Vletter WB, et al. Accuracy and reproducibility of quantitation of left ventricular function by real-time three-dimensional echocardiography versus cardiac magnetic resonance. Am J Cardiol 2008;102:778–83.
Gandy SJ, Waugh SA, Nicholas RS, Simpson HJ, Milne W, Houston JG. Comparison of the reproducibility of quantitative cardiac left ventricular assessments in healthy volunteers using different MRI scanners: a multicenter simulation. J Magn Reson Imaging 2008;28:359–65.
Hesse B, Tägil K, Cuocolo A, Anagnostopoulos C, Bardiés M, Bax J, et al. EANM/ESC procedural guidelines for myocardial perfusion imaging in nuclear cardiology. Eur J Nucl Med Mol Imaging 2005;32:855–97.
Montelatici G, Sciagrà R, Passeri A, Dona M, Pupi A. Is 16-frame really superior to 8-frame gated SPECT for the assessment of left ventricular volumes and ejection fraction? Comparison of two simultaneously acquired gated SPECT studies. Eur J Nucl Med Mol Imaging 2008;35:2059–65.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sciagrà, R., Berti, V., Genovese, S. et al. Reliability of myocardial perfusion gated SPECT for the reproducible evaluation of resting left ventricular functional parameters in long-term follow-up. Eur J Nucl Med Mol Imaging 37, 1722–1729 (2010). https://doi.org/10.1007/s00259-010-1444-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-010-1444-y