
Abstract
Purpose
Conflicting data exist about the difference between 8- and 16-frame gated single-photon emission computed tomography (SPECT) left ventricular volumes and ejection fraction (EF); moreover, the influence of framing on detection of stress-induced functional changes is unknown.
Methods
In 133 patients, two separate gated SPECT studies, one with 8 and one with 16 frames, were simultaneously acquired during a single gantry orbit using dedicated software. In 33 of 133 patients, two additional studies (with 8 and 16 frames, respectively) were acquired using arrhythmia rejection. Left ventricular EF and volumes were calculated using the QGS software. Stress-induced ischemia was identified on summed perfusion images.
Results
Arrhythmia-rejection did not influence volumes and EF independently of framing rate. Using data without arrhythmia-rejection, there was a significant difference in volumes and EF between 8 and 16 frames both in resting and post-stress gated SPECT. However, the difference was small: 2.6% for resting and 2.8% for post-stress EF. Both using 8 and 16 frames, there were significantly larger volumes and lower EF in patients with than without stress-induced ischemia. A stress-induced decrease >5 EF units was observed in 26 of 133 patients using 8 and in 23 of 133 using 16 frames, respectively, with finding agreement in 19 patients.
Conclusions
Comparing two simultaneously acquired studies, the use of 16 instead of 8 frames has minor and predictable influence on functional data. Furthermore, there are no differences in the detection of stress-induced functional changes. The advantage of 16 over 8 frames in the daily clinical practice appears questionable.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The choice of the best framing interval in myocardial perfusion gated single-photon emission computed tomography (SPECT) is still an unresolved issue [1]. The use of 8 frames is supported by the better count statistics in each frame, but higher framing intervals, namely 16 frames, have been reported to give more accurate results in comparison with reference standards [1–7]. Moreover, recent studies suggest that 16-frame gated SPECT allows to estimate the left ventricular diastolic function as well, although for this aim higher framing rates would be desirable [8]. The direct comparison of two truly independent gated SPECT acquisitions with different framing rates has been so far feasible only in the setting of phantom studies and has not definitively demonstrated the superiority of 16 over 8 frames [9]. Human studies based on reframing of gated SPECT acquired with higher framing rate to simulate lower framing data have given conflicting results [10–12]. Recently, a gamma camera manufacturer has implemented on its system a patented technical modality (Concurrent Imaging, V 2.0, Philips Medical Systems) that allows creating multiple image sets during the same acquisition. This makes possible to acquire simultaneously an 8-frame and a 16-frame gated SPECT and to compare their results without the need of post-acquisition re-framing. We took advantage of this opportunity to directly compare 8- versus 16-interval ejection fraction (EF) and left ventricular volume measurements in a cohort of consecutive patients. Furthermore, we also compared the data of resting and stress gated SPECT to examine whether framing resolution has some influence on the detection of stress-induced functional abnormalities.
Materials and methods
Patient population and study protocol
Our patient population consisted of consecutive patients who were referred to our institution for the execution of myocardial perfusion gated SPECT on the basis of the standard clinical indications. Patients were not considered for this study if they had major arrhythmias preventing reliable gating (>1 ectopic beat every six heart cycles) or paced rhythm [13]. Similarly, eligible patients were excluded from subsequent evaluation if at the moment of gated SPECT quantitative analysis the automated identification of the left ventricular borders was ineffective. Gated SPECT images were acquired using a dual day protocol. The same 99mTc sestamibi dosage (740 MBq) was injected at rest and at peak exercise or during pharmacologic stress, and the image collection began at least 60 min later for resting studies and after 30 min for stress scans.
Gated SPECT
Gated SPECT was acquired using a dual-head gamma camera (Skylight, Philips, Milpitas, CA, USA) equipped with high-resolution collimators and using a 15% window centred on the 140-keV photopeak of 99mTc. SPECT was acquired in step-and-shoot mode using a 180° elliptical orbit, matrix size 64 × 64, with 32 projections and 60 s/projection.
Using the Concurrent Imaging V 2.0 software, two separate gated SPECT studies, one with 8 frames and the other with 16 frames per cardiac cycle, were created. The Concurrent Imaging V 2.0 software allows creating multiple image sets with different characteristics such as gating, energy window, dynamic framing and zooming, starting from event data obtained by a common behaviour of the gamma camera gantry. The unchangeable parameters in case of SPECT studies are collimator type, patient orientation, gantry position, gantry orbit and angular sampling.
In the standard acquisition protocol, no arrhythmia rejection was used. A subgroup of patients was studied both with and without arrhythmia rejection (AR). The AR protocol automatically determines the average R–R interval of the studied patient based on the first five beats. The allowable variance was set at 50%. One heartbeat was rejected after the detection of an unacceptable beat. SPECT images were reconstructed using filtered back-projection without attenuation or scatter correction and realigned along the heart axis.
Data analysis
Quantification of gated SPECT data was performed using the quantitative gated SPECT (QGS) method. For each framing modality, end-diastolic volumes (EDV) and end-systolic volumes (ESV) and EF were calculated according to a fully automatic procedure [3]. Perfusion defects were visually evaluated on summed images by an experienced observer blind to patient’s data and expressed as summed rest score, summed stress score and summed difference score [14]. The presence of a summed difference score ≥2 was regarded as indicative of stress-induced ischemia. To define a significant stress-induced EF decrease, we analyzed the data according to two different criteria. First, we considered as significant an EF decrease larger than the 95% confidence interval of delta EF in the non-ischemic patients [15]. Alternatively, we considered significant a decrease in EF greater than five EF units [16].
Statistical analysis
Continuous variables are expressed as mean ± standard deviation and were compared using the two-tailed Student’s t test for paired or unpaired data as appropriate, with the Bonferroni’s correction for multiple comparisons. The agreement between the two framing modalities was assessed using the Bland–Altman analysis [17]. A p value <0.05 was considered statistically significant.
Results
General findings
Of 144 eligible patients, 11 were excluded because the QGS program failed to automatically detect the left ventricle borders, mainly because of extracardiac activity. The final study population included 133 patients (103 men and 30 women; mean age 64 ± 11 years) referred to gated SPECT for the following indications: diagnosis of coronary artery disease (CAD; 67 patients), re-assessment of known CAD (29) and follow-up after revascularization (37). The stress test was exercise stress testing in 83 cases and pharmacological stress with dipyridamole in 50 cases.
According to the analysis of myocardial perfusion on summed gated SPECT images, we found a resting perfusion defect in 44 patients; a stress-induced perfusion defect was registered in 49 patients (34 with abnormal and 15 with normal resting perfusion).
Among the group of 33 patients that underwent arrhythmia-corrected and non-arrhythmia-corrected gated SPECT, 21 had normal electrocardiogram, five had ectopic beats, four had right bundle branch block, two had extreme left axis deviation and one had left bundle branch block.
Influence of arrhythmia rejection
As shown in Table 1, in our population of patients without major arrhythmias, the use of AR did not significantly influence the volume and ejection fraction measurements with 8- and with 16-frame acquisition. Therefore, the comparison between the two framing protocols was performed using the data without AR of the entire study population.
Left ventricular volumes
Resting 16-frame EDV (107 ± 44 ml) was significantly larger (p < 0.00001) than 8-frame EDV (105 ± 44 ml). Resting 16-frame ESV (49 ± 35 ml) was significantly smaller (p < 0.00001) than 8-frame ESV (51 ± 36 ml). Similar differences were registered for post-stress volumes. Post-stress 16-frame EDV (104 ± 46 ml) was larger than 8-frame EDV (102 ± 46 ml, p < 0.00001), and post-stress 16-frame ESV (48 ± 38 ml) was smaller than 8-frame ESV (50 ± 38 ml, p < 0.00001). According to Bland–Altman plot analysis, the mean difference between resting 16- and 8-frame EDV was 2.0 ml [95% confidence interval (CI) 1.6–2.4 ml; Fig. 1]. The corresponding values for post-stress EDV were 2.1 ml, 95% CI 1.7–2.5 ml. For ESV, the related values were −2.1 ml (95% CI −1.6 to −2.6 ml) for 16-frame versus 8-frame resting gated SPECT (Fig. 2) and −2.0 ml (95% CI −1.7 to −2.4 ml) for 16-frame versus 8-frame post-stress gated SPECT.

Bland–Altman analysis of agreement for resting EDV between 16- (16-fr) and 8-frame (8-fr) gated SPECT

Bland–Altman analysis of agreement for resting ESV between 16- (16-fr) and 8-frame (8-fr) gated SPECT
Ejection fraction
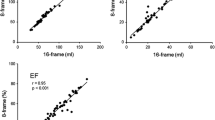
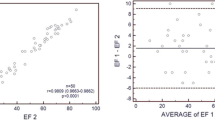
Resting 16-frame EF (57.8 ± 13.0%) was significantly higher (p < 0.00001) than resting 8-frame EF (55.2 ± 12.9%). Furthermore, post-stress 16-frame EF (58.4 ± 13.5%) was significantly higher (p < 0.00001) than post-stress 8-frame EF (55.6 ± 13.4%). According to Bland–Altman plot analysis, the mean difference between resting 16- and 8-frame EF was 2.7% (95% CI 2.3–3.1%; Fig. 3). The corresponding values for post-stress EF were 2.8% (95% CI 2.5–3.2%; Fig. 4).

Bland–Altman analysis of agreement for resting EF between 16- (16-fr) and 8-frame (8-fr) gated SPECT

Bland–Altman analysis of agreement for post-stress EF between 16- (16-fr) and 8-frame (8-fr) gated SPECT
Stress-induced functional abnormalities
As shown in Table 2, patients with stress-induced ischemia were found to have significantly larger volumes and lower EF than patients without ischemia. These differences were not influenced by the framing rate. Delta (post-stress—resting) EDV was significantly different in ischemic versus non-ischemic patients using both framing rates, with the ischemic patients showing a slight EDV increase and the non-ischemic patients some EDV decrease after stress. Delta ESV showed a similar behaviour, but the difference between ischemic and non-ischemic patients was just borderline significant in 16-frame gated SPECT and did not reach statistical significance in 8-frame gated SPECT (Table 3). The delta EF was not significantly different in ischemic patients versus non-ischemic patients according to both 8- and 16-frame gated SPECT data (Table 3). An EF drop larger than the 95% CI of delta EF in the non-ischemic patients was registered in one single severely ischemic (summed difference score = 8) patient according to 8-frame gated SPECT and in the same patient and in another severely ischemic (summed difference score = 11) patient in 16-frame gated SPECT. In 19 patients (nine with inducible ischemia), an EF decrease greater than five EF units was registered both using 8- and 16-frame gated SPECT. In seven additional patients (four with inducible ischemia), such an EF drop was observed only in 8-frame gated SPECT. Finally, in four other patients (all without inducible ischemia), the EF decrease was detected solely by 16-frame gated SPECT.
Discussion
Since the early 1990s, when gated SPECT was introduced in the clinical practice, 8-interval framing has been the standard modality for data acquisition [2, 3]. The choice of 8 frames was supported by the need to achieve a high count statistics in each frame for the good definition of the cardiac walls and the reliable assessment of regional wall motion, without unduly prolonging the total acquisition time [1]. Already in 1995, however, Germano et al., in their first description of the QGS quantitative algorithm, reported an underestimation of ejection fraction using 8-frame instead of 16-interval gated SPECT, but since the difference was predictable, constant over a wide range of values and fairly small, they concluded that 8 frames were nevertheless to be preferred [3]. This underestimation was mainly confirmed by studies that compared the left ventricular EF obtained by 8-frame gated SPECT with other reference standards, such as equilibrium radionuclide angiocardiography, contrast ventriculography and magnetic resonance imaging [4–7]. Just few studies directly compared the different framing modalities in the same patients. Kumita et al. performed a 32-frame acquisition and its reframing in 16- and in 8-interval gated SPECT [10]. The results obtained using the QGS algorithm were compared with those of equilibrium radionuclide angiocardiography and confirmed the EF underestimation, which was just moderate using 16 frames but appeared quite remarkable using 8 frames. Navare et al. performed a 16-frame gated SPECT and the subsequent reframing to 8 frames [11]. Using a quantitative algorithm different from QGS, they observed significantly larger end-diastolic volumes, smaller end-systolic volumes and higher EF using 16-interval gated SPECT and concluded that 16-interval framing should be preferred. Most recently, Schaefer et al. compared both the QGS and the 4D-MSPECT algorithms and detected little differences for EF and volumes between 8- and 16-interval, with slightly smaller variability for QGS [12]. A limitation of all these studies is that it was not possible to compare two truly independent gated SPECT acquisitions, but it was necessary to reframe the originally acquired data. With regard to this point, Visser et al., using a dedicated phantom and two consecutive independent acquisitions, showed that the EF measured by the QGS software were overestimated as compared to the actual value and that the overestimation was larger in the 16-frame gated SPECT [9]. Moreover, the difference between the two types of framing appeared smaller than that reported in the above cited human studies. Therefore, the actual difference between 8-frame versus 16-frame gated SPECT EF and volumes using the most widely adopted quantitative algorithm, the QGS, is still unclear.
In the present study, we had the possibility to compare two independent gated SPECT acquisitions, one with 8 and the other with 16 frames, collected simultaneously during the same detector orbit. This opportunity is based on the patented software of one major gamma camera manufacturer. In theory, this would eliminate the problem of choosing between different framing rates because it is possible to acquire simultaneously a non-gated and one or more gated SPECT studies with different framing rates. On the other hand, it offers the ideal tool to directly compare the influence of framing on gated SPECT results, and this remains an important issue, both because other gamma camera systems do not allow this simultaneous acquisition capability and because acquiring more than one study implies greater memory occupation and longer processing times.
According to our results, it is confirmed that 8-frame gated SPECT slightly underestimates the EDV and overestimates the ESV both in resting and in post-stress gated SPECT, but the differences are very limited and appear clearly lower than that reported by others [11]. Consequently, EF is slightly underestimated as well, but again, the difference is almost negligible, as formerly pointed out by Germano et al. [3]. Our results do not confirm the superiority of 16 over 8 frames that had been suggested in prior reports [10, 11]. As an additional, secondary finding, our data show that in patients without major arrhythmias the use of AR does not influence the QGS results.
To our best knowledge, the influence of framing rates on the comparison between resting and post-stress functional data had not been examined before. Several reports suggest that the detection of post-stress EF changes might be useful to identify patients with severe and extensive coronary artery disease [16, 18–20]. The main finding of the present study is that there are no major differences between 8- and 16-frame gated SPECT in the capability to detect stress-induced volumetric or EF changes. In particular, the proportion of patients with major stress-induced EF drop is the same in the two gated SPECT, and hence there are no data to suggest that 16-frame gated SPECT is more effective than 8-frame for the detection of ischemic functional changes in spite of its theoretically more accurate definition of left ventricular volumes and EF.
The study limitations must be considered when interpreting our results. The patient population was unselected, and thus there is not an external gold standard to evaluate the meaning of stress-induced functional changes. We could only correlate these changes with the perfusion pattern in gated SPECT itself, so that it is impossible to assess whether patients with stress-induced functional changes without ischemia are false positive or patients with severe diffuse coronary artery disease. On the other hand, this patient population reflects the daily reality of a busy Nuclear Medicine Laboratory, and this would reinforce the concept that 16 frames do not improve significantly the reliability of gated SPECT calculations in everyday clinical routine. We used one processing algorithm only, and we cannot exclude that other programs would have given different results. Further studies using the simultaneous acquisition capability that we employed could be helpful to definitively establish the relationship between the different processing algorithms and framing rates.
Conclusions
This study suggests that in a direct comparison within an unselected population of patients submitted to myocardial perfusion gated SPECT, the difference between 8 and 16 frames has a very small and predictable influence on the functional measurements, so that there are no reasons to prefer a higher framing rate for the calculation of left ventricular volumes and EF. Moreover, the comparison between resting and post-stress measurements does not suggest that a higher framing rate could be useful to improve the recognition of stress-induced functional changes.
References
Hesse B, Tagil K, Cuocolo A, Anagnostopoulos C, Bardiés M, Bax J, et al. EANM/ESC procedural guidelines for myocardial perfusion imaging in nuclear cardiology. Eur J Nucl Med Mol Imaging 2005;32:855–97.
DePuey EG, Nichols K, Dobrinsky C. Left ventricular ejection fraction assessed from gated technetium-99 m-sestamibi SPECT. J Nucl Med 1993;34:1871–6.
Germano G, Kiat H, Kavanagh PB, Moriel M, Mazzanti M, Su HT, et al. Automatic quantification of ejection fraction from gated myocardial perfusion SPECT. J Nucl Med 1995;36:2138–47.
Stollfuss JC, Haas F, Matsunari I, Neverve J, Nekolla S, Schneider-Eicke J, et al. Regional myocardial wall thickening and global ejection fraction in patients with low angiographic left ventricular ejection fraction assessed by visual and quantitative resting ECG-gated 99 m Tetrofosmin single-photon emission tomography and magnetic resonance imaging. Eur J Nucl Med 1998;25:522–30.
Nichols K, Amis J, dePuey G, Mieres J, Malhotra S, Rozanski A. Relationship of gated SPECT ventricular function parameters to angiographic measurements. J Nucl Cardiol 1998;5:295–303.
Manrique A, Faraggi M, Vera P, Vilain D, Lebtahi R, Cribier A, et al. 201-Tl and 99 m-Tc-MIBI gated SPECT in patients with large perfusion defects and left ventricular dysfunction: comparison with equilibrium radionuclide angiography. J Nucl Med 1999;40:805–9.
Vaduganathan P, He ZX, Vick W, Mahmarian JJ, Verani MS. Evaluation of left ventricular wall motion, volumes and ejection fraction by gated myocardial tomography with technetium 99 m-labeled tetrofosmin: a comparison with cine magnetic resonance imaging. J Nucl Cardiol 1999;6:3–10.
Akincioglu C, Berman DS, Nishina H, Kavanagh PB, Slomka PJ, Abidov A, et al. Assessment of diastolic function using 16-frame 99mTc-sestamibi gated myocardial perfusion SPECT: normal values. J Nucl Med 2005;46:1102–8.
Visser JJ, Busemann Sokole E, Verberne HJ, Habraken JB, van de Stadt HJ, Jaspers JE, et al. A realistic 3-D gated cardiac phantom for quality control of gated myocardial perfusion SPET: the Amsterdam gated (AGATE) cardiac phantom. Eur J Nucl Med Mol Imaging 2004;31:222–8.
Kumita S, Cho K, Nakajo H, Toba M, Uwamori M, Mizumura S, et al. Assessment of left ventricular diastolic function with electrocardiography-gated myocardial perfusion SPECT: comparison with multigated equilibrium radionuclide angiography. J Nucl Cardiol 2001;8:568–74.
Navare SM, Wackers FJ, Liu YH. Comparison of 16-frame and 8-frame gated SPET imaging for determination of left ventricular volumes and ejection fraction. Eur J Nucl Med Mol Imaging 2003;30:1330–7.
Schaefer WM, Kaiser HJ, Kuehl H, Koch KC, Nowak B, Buell U. Quantification of left ventricular volumes and ejection fraction from 16- and rebinned 8-frame gated (99 m)Tc-tetrofosmin SPECT — Comparison of 4D-MSPECT and QGS. Nuklearmedizin 2007;46:22–8.
ASNC Executive Council. American Society of Nuclear Cardiology position statement on electrocardiographic gating of myocardial perfusion SPECT scintigrams. J Nucl Cardiol 1999;6:470–1.
Sharir T, Germano G, Waechter PB, Kavanagh PB, Areeda JS, Gerlach J, et al. A new algorithm for the quantitation of myocardial perfusion SPECT. II: validation and diagnostic yield. J Nucl Med 2000;41:720–7.
Ramakrishna G, Miller TD, Hodge DO, O’Connor MK, Gibbons RJ. Differences in left ventricular ejection fraction and volumes measured at rest and poststress by gated sestamibi SPECT. J Nucl Cardiol 2006;13:668–74.
Hida S, Chikamori T, Tanaka H, Usui Y, Igarashi Y, Nagao T, et al. Diagnostic value of left ventricular function after stress and at rest in the detection of multivessel coronary artery disease as assessed by electrocardiogram-gated SPECT. J Nucl Cardiol 2007;14:68–74.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986;1:307–10.
Johnson LL, Verdesca SA, Aude WY, Xavier RC, Nott LT, Campanella MW, et al. Postischemic stunning can affect left ventricular ejection fraction and regional wall motion on post-stress gated sestamibi tomograms. J Am Coll Cardiol 1997;30:1641–8.
Sharir T, Bacher-Stier C, Dhar S, Lewin HC, Miranda R, Friedman JD, et al. Identification of severe and extensive coronary artery disease by postexercise regional wall motion abnormalities in Tc-99 m sestamibi gated single-photon emission computed tomography. Am J Cardiol 2000;86:1171–5.
Toba M, Kumita S, Cho K, Ibuki C, Kumazaki T, Takano T. Usefulness of gated myocardial perfusion SPECT imaging soon after exercise to identify postexercise stunning in patients with single-vessel coronary artery disease. J Nucl Cardiol 2004;11:697–703.
Conflict of interest statement
None declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Montelatici, G., Sciagrà, R., Passeri, A. et al. Is 16-frame really superior to 8-frame gated SPECT for the assessment of left ventricular volumes and ejection fraction? Comparison of two simultaneously acquired gated SPECT studies. Eur J Nucl Med Mol Imaging 35, 2059–2065 (2008). https://doi.org/10.1007/s00259-008-0866-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-008-0866-2