
Abstract
Objective
The purpose of this study was to evaluate the incidence and risk factors associated with adjacent vertebral fracture after percutaneous vertebroplasty (PVP) to treat osteoporotic vertebral compression fractures. We also investigated the effect of intradiscal cement leakage on adjacent vertebral fracture formation after PVP.
Materials and methods
From January 2003 to March 2009, 188 patients (163 women, 25 men; mean age, 70.9 years; range, 42–92 years) who underwent 214 PVP sessions at 351 levels for osteoporotic vertebral compression fractures were retrospectively enrolled in this study. The effect of intradiscal cement leakage on new adjacent vertebral fracture formation after PVP was evaluated. Possible other risk factors were also analyzed using univariate and multivariate methods. The risk factors included age, gender, mean bone mineral density (BMD), the vertebral level treated, presence of an intravertebral cleft or cyst before treatment, kyphosis angle, wedge angle, and the injected cement volumes.
Results
During the follow-up periods, new adjacent vertebral fractures developed in 36 (10.3%) of 351 treated levels. For 91 (25.9%) levels, intradiscal cement leakage was detected on procedural fluoroscopic radiographs. There was no statistically significant association between intradiscal cement leakage and new adjacent vertebral compression fracture (p = 0.789). Among the other risk factors, only the vertebral levels treated, especially the thoracolumbar junction, showed a significant relationship to new adjacent vertebral fractures (univariate analysis, p = 0.037; multivariate analysis, p = 0.043).
Conclusions
Intradiscal cement leakage does not seem to be related to subsequent adjacent vertebral compression fracture in patients who underwent PVP for treatment of an osteoporotic compression fracture. The thoracolumbar location of the initial compression fracture is the only factor correlated with an adjacent vertebral fracture after PVP.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Percutaneous vertebroplasty (PVP) is an efficient procedure to treat pain due to osteoporotic vertebral compression fractures. Previous reports have shown that 8–52% of patients treated with vertebroplasty return with pain due to a new compression fracture. The new fractures often occur in adjacent vertebral bodies [1–9]. Possible explanations for these new fractures are preexistent bone fragility in osteoporotic patients, immediate increases in stiffness and strength of the treated vertebral body, and improved mobility that causes a new load on vertebral bodies [1–5, 7, 8, 10–12].
Cement leakage outside the treated vertebral body is relatively common but is generally of no clinical significance. Some previous studies have shown that cement leakage into an adjacent disc space is a risk factor for new vertebral fracture after PVP [6, 9, 11, 13, 14]. In our clinical work, we have often observed multiple incidents of cement leakage into the disc space during initial PVP. However, many of these patients have not returned with new adjacent vertebral fracture. Based on this observation, we postulated that intradiscal cement leakage does not increase the risk of a new adjacent vertebral fracture.
The purpose of this study was to evaluate the incidence and the risk factors of adjacent fracture after PVP in osteoporotic vertebral compression fractures. The causal relationship of intradiscal cement leakage to adjacent vertebral fracture formation after PVP was also studied.
Materials and methods
Patient population
Our institutional review board approved this retrospective study and waived the requirement of informed consent. From January 2003 to March 2009, 188 patients (163 women, 25 men; mean age, 70.9 years; range, 42–92 years) who underwent 214 PVP sessions at 351 levels for osteoporotic vertebral compression fractures (OCF) at our institution were retrospectively enrolled in this study. The mean follow-up duration was 38.5 months (range 1–74 months).
All patients underwent preoperative spinal magnetic resonance (MR) imaging less than 1 month before the PVP. The following MR imaging features indicative of acute fracture activity were part of the inclusion criteria: (1) acute vertebral marrow edema with low signal intensity on T1-weighted MR images, and high signal intensity on T2-weighted images with or without fracture lines or (2) intravertebral cleft or cyst with air and/or fluid collection in the vertebral body. MR imaging was also used to rule out other spinal diseases including infection or malignancy.
Of the 188 patients, 106 underwent a single PVP session for their single level of osteoporotic compression fracture. There were 82 patients with multiple OCFs that were treated during the single or multiple PVR sessions as they developed: two levels in 43 patients, three levels in 20 patients, four levels in 11 patients, and five or more levels in 8 patients.
Follow-up with conventional radiographs or MR was conducted in the patients who experienced continued or new back pain (n = 120). New vertebral compression fractures were diagnosed when plain radiography showed a definite decrease in the height of the vertebral body or when MRI showed low signal intensity of bone marrow within the vertebral body on T1-weighted images in a matched site of pain and tenderness. The time from the date of the initial intervention with PVP to the diagnosis of subsequent fractures was calculated (fracture-free interval). Patients who did not complain of back pain during the follow-up period did not require further imaging and were satisfied with the procedure (n = 68). Follow-up phone calls were made for the 68 patients who did not revisit the hospital after the PVP procedure. All of these patients were asymptomatic and did not require an additional imaging study.
PVP technique
All of the PVPs were performed by three musculoskeletal radiologists in our institute using an established technique. Under single or biplane angiography units, bipedicular or unipedicular approaches were adopted by using an 11- or 13-gauge single beveled needle (“J” type bone marrow needle, Manan; MDTech, Wheeling, IL, USA). The mixed polymethyl methacrylate (PMMA) bone cement (Exolent Spine; Elmdown, London, England) was injected into the vertebral body under direct fluoroscopic control. The procedure was immediately terminated if the cement reached the posterior fourth of the vertebral body or if the cement leakage occurred outside of the vertebral body. After the procedure, plain radiographs of each treated vertebral level were assessed to characterize the deposition of cement.
Comparison parameters
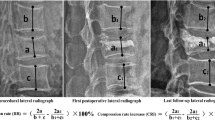
The following parameters were evaluated for possible relationships with the occurrence of adjacent new vertebral fracture after PVP. First, the presence or absence of intradiscal cement leakage was analyzed. Any cement leakage beyond the endplate and into the disc was checked on the procedural or immediate postoperative lateral radiographs. The injected cement volume per each treated vertebral body was also analyzed. Parameters related to the vertebral body treatment were considered, including the vertebral levels treated, the presence of intravertebral cleft/cyst before treatment, the kyphosis angle (Cobb’s angle), and the wedge angle. The treated vertebral levels were categorized as T3 through T9 (n = 74), T10 through L2 (n = 210), and L3 through L5 (n = 67) (Fig. 1). The presence of an intraosseous cleft or cyst containing gas and/or fluid in the compressed vertebrae was recorded in the preoperative plain radiographs or MRI. On the preoperative radiographs, the kyphosis angle and the wedge angle were calculated. The kyphosis angle was determined using the Cobb method on a lateral view of the spine. The wedge angle was defined as the angle between the superior endplate line and the inferior endplate line of the fractured vertebral body [12]. All images were reviewed by consensus of a musculoskeletal radiologist and a resident. Patient demographics, including age, gender, and BMD at the time of intervention, were also analyzed.

Number of treatments per vertebral level
Statistical analysis
All statistical analysis was performed using SPSS 16.0 software (SPSS, Chicago, IL, USA). Data were presented as the mean ± SD. Univariate and multivariate binary logistic regression analyses were used to determine if the individual factors were independently associated with a subsequent adjacent vertebral fracture. A p value of less than 0.05 was considered statistically significant, and the corresponding 95% confidence limits were calculated.
Results
We identified new adjacent fractures in 36 (10.3%) of the 351 treated vertebral levels during the follow-up period. The mean time between vertebroplasty and a new adjacent vertebral fracture was 6.8 months (range 1–47 months). Intradiscal cement leakage was detected in 91 (25.9%) of the 351 treated vertebral levels. Adjacent new compression fractures occurred in 10 of 91 (11%) levels with intradiscal cement leakage (Fig. 2) and in 26 of 260 (10%) levels without intradiscal cement leakage. For 81 of 91 levels with intradiscal cement leakage, a new adjacent vertebral fracture did not develop during the follow-up period (Fig. 3). Table 1 shows the correlation between incidence of new adjacent fracture and intradiscal cement leakage; no statistically significant association was observed (p = 0.789).

A 74-year-old man with a new adjacent vertebral compression fracture with intradiscal cement leakage after vertebroplasty. Preoperative T1-weighted (a), T2-weighted (b), and fat-suppressed T1-weighted enhanced (c) magnetic resonance images show a fracture line with adjacent marrow edema in the T12 body, suggesting acute osteoporotic compression fracture of T12 (white solid arrows). d Lateral radiograph during vertebroplasty shows intradiscal cement leakage (arrow). Frontal (e) and lateral (f) radiographs 2 months after surgery show a new compression fracture at the T11 vertebral body (dotted arrows)

A 70-year-old woman without adjacent compression fractures after vertebroplasty with intradiscal cement leakage. Preoperative lateral radiograph (a), T1-weighted (b), and T2-weighted (c) sagittal magnetic resonance images show an acute compression fracture in the L1 body (arrows). Frontal (d) and lateral (e) radiographs acquired during percutaneous vertebroplasty show intradiscal cement leakage (arrows). f During 25 months of follow-up, no new adjacent compression fracture developed
The characteristics of patients with new adjacent fracture versus those without new adjacent fracture are summarized in Table 2. Among the patients with adjacent fracture, 3 were men, and 25 were women; among those without adjacent fracture, 22 were men, and 138 were women. The patients with a new adjacent fracture and without an adjacent fracture had mean ages of 71.1 ± 7.2 and 70.9 ± 9.2 years and mean bone mineral densities (BMD; T-score) of −3.1 ± 1.5 and −2.7 ± 1.5, respectively. The percentage of new adjacent vertebral fractures during follow-up periods was 4.1% (3 of 74) for treated vertebrae located in T3 through T9, while the thoracolumbar junction (T10 through L2) had 13.8% (29 of 210), and L3 through L5 showed had a fracture rate of 6.0% (4 of 67). Among the 80 of 351 vertebrae with an intraosseous cleft/cyst before the procedure, 8 levels showed a new adjacent fracture and 72 levels showed no adjacent fracture after PVP. The mean injected cement volumes in the groups with and without new adjacent fractures were 2.8 ± 1.4 and 2.6 ± 1.2 cc, the mean kyphosis angles were 35.1 ± 1.6 and 32.1 ± 0.5, and the mean wedge angles were 11.6 ± 5.2 and 11.9 ± 6.5, respectively. According to the univariate and multivariate analyses, only the treated vertebral levels at the thoracolumbar junction showed a statistically significant relationship to new adjacent fractures (univariate analysis, p = 0.037; multivariate analysis, p = 0.043). None of the following covariates showed an associated risk of new adjacent fracture: age, gender, BMD, presence of intraosseous cleft/cyst before treatment, kyphosis angle, wedge angle, injected cement volume per each vertebra, or intradiscal cement leakage (p > 0.05).
Discussion
Reported rates of cement leaks after PVP are between 11 and 73% [15–17], but these leaks show no clinical significance. Over the past few years, many convincing studies have been undertaken on the subject of cement leakage and cement volume. Lin et al. [11] found that cement leakage into the disc increases the risk of fractures of the adjacent vertebral bodies. This observation was contradicted by several reports that intradiscal leakage does not have a specific impact on the occurrence of adjacent fractures [18, 19].
In our study, we found an intradiscal cement leakage rate of 25.9% during the initial PVP. In contrast to prior results [6, 9, 11, 13, 14], there was no statistically significant increase in the risk of new fractures in the adjacent vertebral body with cement leakage into the disc space. Nor could we identify a statistically significant relationship between injected cement volume and the incidence of new adjacent vertebral fractures. Therefore, most of the new vertebral fractures that were found next to the intradiscal cement leakage might be primarily due to the natural progression of osteoporosis. The difference between the high rate of adjacent fracture formation associated with intradiscal cement leakage in the study by Lin et al. [11] and our analysis is probably related to the difference in the sample sizes and the rates of intradiscal cement leakage. The sample size was smaller (n = 38 patients) and the rate of intradiscal cement leakage was higher (18/38 patients, 47.4%) in the study by Lin et al. than our study (n = 188 patients; rate of intradiscal cement leakage, 91/351 levels, 25.9%). The efforts to reduce the rate of intradiscal cement leakage should be made during vertebroplasty. One of the previously suggested ways is to use a smaller volume of injected cement, which may decrease the risk of leakage [18, 20]. In our study, the mean cement volume per each vertebra was 2.8 ± 1.4 cc in patients with new adjacent vertebral fractures and 2.6 ± 1.2 cc in patients without new adjacent fracture. With low-volume filling, less intradiscal leakage was likely to occur [18]. In cases of severe central compression, the needle tip should be placed more laterally to decrease the frequency of intradiscal cement leakage by keeping the needle tip farther away from the central endplate fracture site [20].
The degree of osteoporosis may be a potential predictor for subsequent fractures [18, 21], but there was no intergroup difference in the BMD in our study population. The BMD may be affected by degenerative changes or osteoarthropathy. Thus, when a weak vertebra is associated with spinal degenerative osteoarthropathy, a high BMD does not necessarily indicate stronger bones, and the risk of vertebral fracture is not diminished [6, 22].
The degree of kyphosis could be one of the possible geometrical factors for new adjacent vertebral fracture after PVP. Theoretically, the kyphotic alignment may exaggerate the hammer effect, causing a subsequent fracture; however, in our study the degree of kyphosis was not significantly related to a new adjacent fracture.
In the present study, the thoracolumbar location of the initial compression fracture is the only correlating factor for a new adjacent vertebral fracture after vertebroplasty. This finding could have been due to the fact that flexion and extension of the spine are at the maximum at the thoracolumbar junction compared to those at other levels, which are relatively immobile [1].
A limitation to our study is that the volume or shape of intradiscal cement leakage was not analyzed. We analyzed only the total amount of injected cement during vertebroplasty but could not calculate the exact volume of intradiscal cement leakage because we did not check post-operative volumetric CT scan routinely. Also, most patients of our study had disc space with moderate to severe degeneration so there was a difficulty in sub-grouping the shape and distribution of the cement leakage. The shape of the cement leakage was flat or vertical in some cases, but most cases had complex shapes. Second, our study did not consider postoperative factors such as the type of medical treatment or the level of physical activity after the procedure. Increased physical activity after the vertebroplasty may cause subsequent fractures. We mainly focused on preoperative or procedure-related factors.
In conclusion, intradiscal cement leakage was not a risk factor for new adjacent vertebral fracture after PVP in patients with osteoporotic vertebral compression fracture. The only significant factor related to a new adjacent fracture after vertebroplasty was a treated vertebral level in the thoracolumbar region. We think that the collapse of an adjacent vertebral body reflects the natural evolution of osteoporosis in the spine regardless of the presence of vertebroplasty.
References
Kim SH, Kang HS, Choi JA, Ahn JM. Risk factors of new compression fractures in adjacent vertebrae after percutaneous vertebroplasty. Acta Radiol. 2004;45(4):440–5.
Dublin AB, Hartman J, Latchaw RE, Hald JK, Reid MH. The vertebral body fracture in osteoporosis: restoration of height using percutaneous vertebroplasty. AJNR Am J Neuroradiol. 2005;26(3):489–92.
Trout AT, Kallmes DF, Kaufmann TJ. New fractures after vertebroplasty: adjacent fractures occur significantly sooner. AJNR Am J Neuroradiol. 2006;27(1):217–23.
Lee WS, Sung KH, Jeong HT, Sung YS, Hyun YI, Choi JY, et al. Risk factors of developing new symptomatic vertebral compression fractures after percutaneous vertebroplasty in osteoporotic patients. Eur Spine J. 2006;15(12):1777–83.
Berlemann U, Ferguson SJ, Nolte LP, Heini PF. Adjacent vertebral failure after vertebroplasty. A biomechanical investigation. J Bone Joint Surg Br. 2002;84(5):748–52.
Ahn Y, Lee JH, Lee HY, Lee SH, Keem SH. Predictive factors for subsequent vertebral fracture after percutaneous vertebroplasty. J Neurosurg Spine. 2008;9(2):129–36.
Lin WC, Cheng TT, Lee YC, Wang TN, Cheng YF, Lui CC, et al. New vertebral osteoporotic compression fractures after percutaneous vertebroplasty: retrospective analysis of risk factors. J Vasc Interv Radiol. 2008;19(2 Pt 1):225–31.
Uppin AA, Hirsch JA, Centenera LV, Pfiefer BA, Pazianos AG, Choi IS. Occurrence of new vertebral body fracture after percutaneous vertebroplasty in patients with osteoporosis. Radiology. 2003;226(1):119–24.
Hiwatashi A, Ohgiya Y, Kakimoto N, Westesson PL. Cement leakage during vertebroplasty can be predicted on preoperative MRI. AJR Am J Roentgenol. 2007;188(4):1089–93.
Bartynski WS, Heller MT, Grahovac SZ, Rothfus WE, Kurs-Lasky M. Severe thoracic kyphosis in the older patient in the absence of vertebral fracture: association of extreme curve with age. AJNR Am J Neuroradiol. 2005;26(8):2077–85.
Lin EP, Ekholm S, Hiwatashi A, Westesson PL. Vertebroplasty: cement leakage into the disc increases the risk of new fracture of adjacent vertebral body. AJNR Am J Neuroradiol. 2004;25(2):175–80.
Teng MM, Wei CJ, Wei LC, Luo CB, Lirng JF, Chang FC, et al. Kyphosis correction and height restoration effects of percutaneous vertebroplasty. AJNR Am J Neuroradiol. 2003;24(9):1893–900.
Mirovsky Y, Anekstein Y, Shalmon E, Blankstein A, Peer A. Intradiscal cement leak following percutaneous vertebroplasty. Spine. 2006; 31(10):1120–1124.
Schmidt R, Cakir B, Mattes T, Wegener M, Puhl W, Richter M. Cement leakage during vertebroplasty: an underestimated problem? Eur Spine J. 2005;14(5):466–73.
Garfin SR, Yuan HA, Reiley MA. New technologies in spine: kyphoplasty and vertebroplasty for the treatment of painful osteoporotic compression fractures. Spine. 2001; 26(14):1511–1515.
Watts NB, Harris ST, Genant HK. Treatment of painful osteoporotic vertebral fractures with percutaneous vertebroplasty or kyphoplasty. Osteoporos Int. 2001;12(6):429–37.
Shapiro S, Abel T, Purvines S. Surgical removal of epidural and intradural polymethylmethacrylate extravasation complicating percutaneous vertebroplasty for an osteoporotic lumbar compression fracture. Case report. J Neurosurg. 2003;98(1 Suppl):90–2.
Syed MI, Patel NA, Jan S, Harron MS, Morar K, Shaikh A. Intradiskal extravasation with low-volume cement filling in percutaneous vertebroplasty. AJNR Am J Neuroradiol. 2005;26(9):2397–401.
Pitton MB, Herber S, Bletz C, Drees P, Morgen N, Koch U, et al. CT-guided vertebroplasty in osteoprotic vertebral fractures: incidence of secondary fractures and impact of intradiscal cement leakages during follow-up. Eur Radiol. 2008;18(1):43–50.
Peh W, Gillula L, Peck D. Percutaneous vertebroplasty for severe osteoporotic vertebral compression fractures. Radiology. 2002;223:121–6.
Ross PD, Davis JW, Epstein RS, Wasnich RD. Pre-existing fractures and bone mass predict vertebral fracture incidence in women. Ann Intern Med. 1991;114(11):919–23.
Arden NK, Griffiths GO, Hart DJ, Doyle DV, Spector TD. The association between osteoarthritis and osteoporotic fracture: the Chingford Study. Br J Rheumatol. 1996;35(12):1299–304.
Acknowledgments
This study was conducted with the Korea University Research Grant.
All authors have no financial relationships with commercial entities.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lee, KA., Hong, SJ., Lee, S. et al. Analysis of adjacent fracture after percutaneous vertebroplasty: does intradiscal cement leakage really increase the risk of adjacent vertebral fracture?. Skeletal Radiol 40, 1537–1542 (2011). https://doi.org/10.1007/s00256-011-1139-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-011-1139-x