
Abstract
Purpose
To develop a new mathematical model for calculating the volumetric wear of polyethylene cups from known values of the radius of the prosthesis head, the extent of linear wear and the direction of linear wear determined from standard antero-posterior radiographs.
Method
A new mathematical model was developed. The results of this new mathematical model were compared with the results obtained using the standard, frequently used mathematical model, which takes into consideration only the radius of the prosthesis head and the extent of linear wear of the polyethylene cups. The results of both mathematical models were further compared with the results obtained by direct measurement of volumetric wear using the fluid displacement method.
Results
Comparison of the mathematical models shows that the average volumetric wear calculated using the new mathematical model is 8.5% smaller than the average volumetric wear determined by the fluid displacement method, while the average volumetric wear calculated by standard mathematical model is 17.5% higher. The results of the new mathematical model are, thus, notably less biased than those of the standard one.
Conclusion
In calculating the volumetric wear from antero-posterior radiographs, not only the radius of the prosthesis head and the extent of the linear wear but also the direction of the latter has to be considered.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Aseptic loosening remains the major long-term problem in total hip replacement [1, 2, 3, 4]. Polyethylene wear particles have been held responsible for the development of chronic periprosthetic inflammation, which over a period of several years leads to typical changes visible on radiographs [5] and finally to overt clinically manifested loosening and failure of the prosthesis [6, 7]. During walking, several hundred thousands of polyethylene wear particles are released in each step [8]. The decrease in thickness of the prosthesis cup due to wear is measured by determining the geometrical parameters of the prosthesis from the radiographs and can be expressed as linear wear. It usually amounts to 0.09–0.25 mm/year [9, 10, 11, 12]. The volumetric wear, i.e. the decrease in volume of the prosthesis cup due to wear, is linearly proportional to the linear wear and to the square of the radius of the head of the prosthesis [13, 14].
The extent of linear and volumetric wear should be as low as possible in order to delay aseptic loosening of the prosthesis. Several methods have been developed to determine the linear wear from routine antero-posterior radiographs [13, 15]. In calculating the volumetric wear on the basis of measured linear wear, a simple mathematical model is usually applied, where the direction of maximal linear wear is not taken into account [8, 13, 14, 16, 17].
In this study we were interested in the influence of the direction of the maximal linear wear on the calculated volumetric wear. The volumetric wear as a function of the direction of the maximal linear wear was calculated using a new mathematical model and compared with the calculated volumetric wear determined using the standard model where the direction of maximal wear is not taken into account [8, 13, 14, 16, 17]. In addition, we have compared the volumetric wear, calculated with the standard and new mathematical model, with the volumetric wear determined by the fluid displacement method [18, 19].
Materials and methods
Patients
Our research included 34 patients (11 males, 23 females) who had the polyethylene cup of a total hip prosthesis removed due to loosening. The average age of the patients was 64.1 years (min. 41, max. 84 years), while their average weight was 73.8 kg (min. 54 kg, max. 100 kg). All polyethylene cups were made of ultra high molecular weight polyethylene, with an inner surface diameter of 32 mm. The average implantation time of prosthetic implant was 130.3 months (min. 48, max. 205 months).
Radiographs
Two radiographs of each patient's hip were selected for the study. The first radiograph (radiograph-1) was made immediately after the implantation, on average 5 days after the surgery (min. 0, max. 17 days). The second radiograph (radiograph-2) was made before the revision arthroplasty, on average 28 days before surgery (min. 3 days, max. 4 months).
Determination of the extent and direction of linear wear (d) by the radiographic method
Standard radiographic method, first described by Livermore and others [13] was slightly modified and applied to determine the linear wear. The Livermore method first defines the centre of the prosthesis head and the shortest distance to the outer edge of the polyethylene cup in radiograph-1. The same is done in radiograph-2. The difference between both distances is taken as the extent of the linear wear of the polyethylene cup. The direction of linear wear is defined by the angle of the line of linear wear and the vertical through the centre of the prosthesis head.
According to our modified method, centres of the prosthesis head and polyethylene cup on both radiographs were determined (Fig. 1). Both centres on radiograph-1 were transferred to radiograph-2. Transfer was made in such a way that the centres of the polyethylene cup coincide. Due to the fact that radiographs differ in magnification, this is not a straightforward procedure. It was achieved by enlarging or reducing the circles in radiograph-1 until the circle above the polyethylene cup of radiograph-1 matched the circle above the polyethylene cup of radiograph-2 (Fig. 2). The magnification was determined from the known diameter of the prosthesis head, which was 32 mm in all cases. Since measurement is influenced by the degree of anteversion of the polyethylene cup [20], cups with more than 20° of anteversion were excluded (ratio of maximum to minimum diameter of the wire marker less than 3.0) [21].

Determination of the centre of the prosthesis head and the polyethylene cup in radiograph-1. The same is done in radiograph-2

Transferring the centres of radiograph-1 to radiograph-2. After transferring and correcting the difference in the magnification of radiographs, the centres of the polyethylene cups on both radiographs overlap. For better presentation, the circle above the prosthesis head and the polyethylene cup in radiograph-2 is indicated by a dotted line. The extent of the linear wear is defined as the length of the line that connects the centres of the prosthesis heads of both radiographs (d). Direction of the linear wear (angle β) is determined from the angle between elongated line d and the line through both poles of the polyethylene cup (line A)
We defined the extent of linear wear as the length of the straight line between the centres of both prosthesis heads (Fig. 2, d). The direction of the linear wear (Fig. 2, angle β) is given by the angle between this straight line and the line through both poles of the polyethylene cup (Fig. 2, line A).
Determination of the volumetric wear of polyethylene cup (V) from radiographic data using the standard mathematical model
We calculated the volumetric wear in cubic millimetres from the results previously determined by the radiographic method. For this purpose we compared the two mathematical models. The standard, widely used one takes into account only the radius of the prosthesis head (R) and the size of the linear wear (d) [8, 13, 14, 16, 17].
Determination of the volumetric wear of polyethylene cup (V) from radiographic data using the new mathematical model
We developed a new mathematical model for the determination of volumetric wear, which includes the direction of linear wear (Fig. 2, angle β) in addition to the radius of the head and the extent of the linear wear.
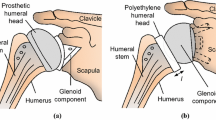
The calculation starts from a spherical head which is in close contact with the semi-spherical cup (Fig. 3A). The head penetrates into the semi-spherical cup (Fig. 3B). This means that the centre of the head is shifted by distance d in the direction of greatest penetration, denoted by the angle β. This means that a certain part of the cup is displaced, as shown by the dark coloured area in Fig. 3B. We are interested in the volume of the displaced part, when the centre of the cup and the spherical head are moved apart by the distance d in the direction of greatest penetration. The volume of displaced part (Fig. 3B) is:

Schematic presentation of semi-spherical cup, spherical head (A) and relative shift of the spherical head into the semi-spherical cup (B). T denotes a random point on the spherical head, d is the distance of the shift of the centre of the prosthesis head in the direction of the greatest penetration, R is the distance between the centre of the prosthesis head after the shift and the selected point after shift, R' is the distance between the centre of the prosthesis head before the shift and the selected point after shift
where R is the distance between the centre of the head and the selected point on its surface (equal to radius of head), R' the distance between the centre of the head before the shift and this same point after the shift (Fig. 3B), and dS the infinitesimal surface area element. The integration takes place in that part of the surface where the head penetrates the cup (Fig. 3B, shaded area).
The following relation can be used to combine distances R and R' (Fig. 3):
By taking into account that the distance d is small in comparison to distances R and R', we can neglect the term d2 in Eq. 3:
Taking into account that the d/R' is small, the expression (Eq. 4) can be approximated as:
so that:
Rotation of the coordinate system is performed in such a way that the point of greatest penetration lies in the xz plane of the rotated system, in the direction of z axis (Fig. 4). In the rotated system, the surface contact area is symmetrical with regard to xz plane and the angle α is the same as before (Fig. 4). One border of the surface contact area lies at a spatial angle of π/2 from the point of greatest penetration. The border on the other side is determined by the geometry of the plastic cup (Figs. 3 and 4). The angle (π/2 - β) gives the direction of greatest penetration of the head relative to the axis of the rotational symmetry of the semi-spherical cup.

Surface intersection in the rotated co-ordinate system
Introducing the coordinates ϕ and ϑ (Fig. 5) so that:

Schematic presentation of the area of the contact between the prosthesis head and the polyethylene cup in the rotated co-ordinate system (shaded area). The meaning of the angles ϑ and ϕ is indicated. Angle β denotes the disection of the linear wear
the infinitesimal element of the surface area can be expressed as:
In order to calculate the volume, V, we insert the expressions (Eqs. 6 and 10) into Eq. 2:
Considering that
and integrating over ϑ from -π/2 to π/2 and over ϕ from -π/2 to β gives a new expression for the volumetric wear:
Determination of the volumetric wear by the fluid displacement method
We compared the relevance of both mathematical models by comparing the results with the results of directly measured volumetric wear of the polyethylene cups by the fluid displacement method. This method measures the volumetric wear directly by measuring the difference in the volume of the liquid necessary to fill the cavities of the worn and a new polyethylene cup [18, 19].
The mathematical model tending to give results closer to the volumetric wear determined by the fluid displacement method would be considered superior. The results were statistically analysed using the established methodology for method comparison studies [22], with the addition of linear regression primarily as a means of clear illustration of the obtained results.
Results
The extent and direction of linear wear determined by radiographic method are shown in Table 1. This table also shows the volumetric wear of the polyethylene cups calculated from radiographic data by using both mathematical models and the volumetric wear measured by the fluid displacement method.
The average volumetric wear calculated using the standard mathematical model, which takes into consideration only the radius of the prosthesis head and the size of the linear wear, was 1329.1 mm3 (min. 707.7, max 1881.9 mm3). The average volumetric wear determined using our new mathematical model, which takes into consideration also the direction of the linear wear, was 1033.5 mm3 (min. 492.7, max. 1316.2 mm3). The average volumetric wear of the polyethylene cups determined by the fluid displacement method was 1132.7 mm3 (min. 578.4, max. 1476.2 mm3).
These results show that the average volumetric wear calculated using the standard mathematical model exceeds the reference volumetric wear determined by the fluid displacement method by 17.5%, while our new mathematical model yields results on average 8.5% smaller than the fluid displacement method. The new mathematical model is thus clearly less biased than the standard one. Focusing on the differences between the reference and the mathematical model within each subject, one notes that not only is the mean difference (−196.5 vs. 99.2 mm3) larger in absolute value for the standard mathematical model when compared with the new one, but the variability of differences is also larger (SD of differences is 106.2 and 63.8 mm3 for the standard and the new mathematical model, respectively).
From these parameters, confidence intervals (CI) for bias and for the limits of agreement [22] were calculated, whereby the method giving (on average) results higher than the reference is indicated with a negative value of bias, and the method giving (on average) results lower than the reference is indicated with a positive value of bias. For the standard mathematical model, the 95% CI for bias is [−154.4, −238.6] mm3, while for the new mathematical model it is [73.9, 124.5] mm3. For the standard mathematical model, the limits of agreement are −408.9 mm3 (lower limit, i.e. mean difference − 2 × SD of mean difference) and 15.9 mm3 (upper limit, i.e. mean difference + 2 × SD of mean difference), while for the new model the limits of agreement are −28.3 mm3 (lower limit) and 226.8 mm3 (upper limit). For the standard mathematical model, the 95% CI for the lower limit of agreement is [−481.8, −336.0] mm3 and the 95% CI for the upper limit of agreement is [−57.0, 88.8] mm3; for the new mathematical model, the 95% CI for the lower limit of agreement is [−72.1, 15.5] mm3 and the 95% CI for the upper limit of agreement is [183.0, 270.5] mm3. All these parameters serve only to reinforce the general conclusion that in comparison to the standard mathematical model, the new one provides values that are less biased on average, as well as less likely to deviate substantially from the reference value for each individual subject.
Another way to present these results is the plot of difference between the reference volumetric wear determined by the fluid displacement method and the volumetric wear determined by the method in question against the average of the two data points of each subject (Fig. 6), known as the method-comparison chart [22]. A general positive finding, revealed by the two plots, is that the precision of neither of the two mathematical models appears to be dependent on the extent of the wear. It is evident, though, that there are many fewer data points outside the limits of agreement for the new mathematical model.

Method comparison chart for the standard mathematical model and the new mathematical model, with the fluid displacement method taken as reference. Difference between the reference volumetric wear (determined by the fluid displacement method) and volumetric wear determined by the method in question is plotted against the average of the two data points of each subject. The solid line represents perfect equivalence of the method in question with the reference, and the two dashed lines represent the estimated limits of agreement. In the upper diagram, the results of the standard mathematical model are compared to the results of the reference model (with data points depicted by squares), and the behaviour of the new mathematical model is studied in the lower diagram (where data points are depicted by triangles). The overestimation of the standard model is evident from the fact that all differences are negative, and the underestimation of the new model is shown by the fact that all but three differences are positive. The superiority of the new model is indicated by the narrower limits of agreement (note the values on the vertical axis), as well as by only about half as many triangles as squares falling outside the limits of agreement. Neither model shows systematic dependence of the imprecision on the magnitude of the volumetric wear
Comparison of the results of both mathematical models is provided by the scatter-plot, showing that the results of our new mathematical model are closer to those measured with the fluid displacement method (Fig. 7). The conclusion that the new mathematical model, which takes into consideration the direction of the linear wear, is more accurate in calculating the volumetric wear of polyethylene cups on the basis of the radiographic method can also be backed up by simple least-squares linear regression. We regressed the measurements from the fluid displacement method on the estimates of volumetric wear from the standard model (πR2d) and the estimates of volumetric wear from the new model (πR2d(1+sinβ)/2), whereby the regression line was forced through the origin. In this way, the regression coefficient obtained is equal to the "correction factor" by which the results of the respective mathematical model should be multiplied in order to coincide with the reference. For the standard mathematical model, the regression slope was 0.8494, while for our new mathematical model it was 1.0929. The greater accuracy of the new model is evident, especially if one remembers that a value of 1.3012 (i.e. 1/0.8494, and not 1.1506=2−0.8494) would represent underestimation of the new model equivalent to the overestimation of the standard model.

A comparison of the volumetric wear determined by the fluid displacement method with the volumetric wear calculated with the standard (Eq. 1) and new mathematical model (Eq. 13)) from radiographic data. The thick straight line is the ideal, theoretical curve representing the points where the volumetric wear determined by the fluid displacement method and volumetric wear determined from radiographic data would be the same. A deviation of points from this ideal line can be seen. Squares, which denote the interdependence between the volumetric wear determined by the fluid displacement method and volumetric wear calculated using the standard mathematical model, lie above the curve. Triangles, which show the interdependence between the volumetric wear determined by the fluid displacement method and the volumetric wear calculated using the new mathematical model, lie below the curve
Discussion
The radiographic method, first described by Livermore and others [13], is today the most frequently used method for determining the linear wear of polyethylene cups and its direction "in vivo". Martel and Berdia [9] indicated that this method had certain deficiencies, especially in determining the direction of linear wear according to the narrowest part of the polyethylene cup.
In this study, we improved the mathematical model for calculation of volumetric wear from radiographic data. Besides the radius of the prosthesis head and the extent of linear wear, the direction of linear wear was taken into account as well. Therefore, the precise determination of the direction of linear wear was of crucial importance. For this purpose, the direction of linear wear was determined from the direction of the shift of the centre of the prosthesis head, caused by long-term functioning of the prosthesis. We believe that the direction of linear wear determined in this way is more precise compared with the earlier determinations [13].
We provide clear evidence that our new mathematical model, which takes into consideration the direction of linear wear and not only the radius of the prosthesis head and the extent of linear wear, is more accurate for calculating volumetric wear from radiographic data. Method-comparison statistical analyses provide further support for the conclusion that the new mathematical model is more accurate than the standard one.
In addition to the proofs of superiority of the new model, it should be emphasised that the new model is potentially even more accurate than demonstrated by the obtained results, which is argued below.
First, the radiographic method calculates the extent and the direction of the linear wear of the polyethylene cups only in the sagittal plane (we analysed only the antero-posterior radiographs). So we can assume that the measured linear wear is in fact slightly inferior to the real value, since the location of linear wear in the frontal plane is not determined (this could be determined by analyzing lateral radiographs). Due to this fact the volumetric wear determined by mathematical models is slightly smaller than the real value. If we had considered the directions of linear wear in both planes, the graphic presentation, as the one shown in Fig. 7, would have shown the points of volumetric wear slightly higher. This means that the points of volumetric wear calculated by the new mathematical method (triangles in Fig. 7) would have been closer to the theoretical curve, while the points of volumetric wear calculated by the standard mathematical method (squares in Fig. 7) would have been more distant. Consequently, the predictions of the new mathematical model would have been even more accurate, while the standard model would have deviated even more from the ideal model.
Also in favour of this fact are the findings of the study carried out by Kabo et al. [23]. By defining the volumetric wear of polyethylene cups in both planes, they determined that the true volumetric wear was 0.53 times the volumetric wear defined by the standard mathematical model. In our study, which determines the volumetric wear only in the sagittal plane (we analysed only the antero-posterior radiographs of hips), the actual volumetric wear was 0.85 times the volumetric wear, defined by the standard mathematical model. This means that when considering the volumetric wear of polyethylene cups also in the frontal plane (lateral radiographs of hips), our mathematical model would have approached the ideal model, whereas the standard model would diverge from it even further.
Second, volumetric wear determined by the fluid displacement method should be larger than volumetric wear determined from radiographic data due to deep abrasion marks in the inner surface of the polyethylene cup. These marks are the consequence of three-layer abrasion [24, 25] and can increase the extent of the volumetric wear. Contrary to the radiographic method, the fluid displacement method takes into account the volumetric wear hidden in these abrasions. Had this part of volumetric wear been somehow accounted for by both mathematical models, the points in Fig. 7 would have moved upwards, bringing the triangles even closer to and the squares even further away from the line of equivalence with the fluid displacement method. This would have additionally improved the accuracy of the new mathematical model, and additionally worsened the accuracy of the standard model.
Conclusion
The determination of volumetric wear of the polyethylene cups from radiographic data must take into account the direction of the linear wear and not only the radius of the prosthesis head and the extent of the linear wear. Consequently, clinicians might consider including these findings when calculating volumetric wear from radiographic data.
References
Amstutz HC, Campbell P, Kossovsky N, Clarke IC. Mechanism and clinical significance of wear debris induced osteolysis. Clin Orthop 1992; 276:7–18.
Howie DW. Tissue response in relation to type of wear particles around failed hip arthroplasties. J Arthroplasty 1990; 5:337–348.
Maloney WJ, Smith RL. Periprosthetic osteolysis in total hip arthroplasty: the role of particulate wear debris. J Bone Joint Surg 1995; 77-A: 1448–1461.
Milošev I, Minovič A, Antolič V, Herman S, Pavlovčič V, Campbell P, Cör A. Extensive metallosis and necrosis in failed prostheses with cemented titanium-alloy stems and ceramic heads. J Bone Joint Surg 2000; 82-B: 352–357.
McCaskie AW, Brown AR, Thompson JR, Gregg PJ. Radiological evaluation of the interfaces after cemented total hip replacement. J Bone Joint Surg 1996; 78-B: 191–194.
Cooper RA, McAllister CM, Borden LS, Bauer TW. Polyethylene debris-induced osteolysis and loosening in uncemented total hip arthroplasty. A cause of late failure. J Arthroplasty 1992; 7:285–290.
Schmalzried TP, Jasty M, Harris WH. Periprosthetic bone loss in total hip arthroplasty. Polyethylene wear debris and the concept of the effective joint space. J Bone Joint Surg 1992; 74-A: 849–863.
Schmalzried TP, Callaghan JJ. Current concept review. Wear in total hip and knee replacements. J Bone Joint Surg 1999; 81-A: 115–132.
Martel JM, Berdia S. Determination of polyethylene wear in total hip replacements with use of digital radiographs. J Bone Joint Surg 1997; 79-A: 1635–1641.
Salvati EA, Wilson PD, Jolley MN. A ten year follow-up study of our first one hundred consecutive Charnley total hip replacements. J Bone Joint Surg 1985; 67-B: 757–761.
Wroblewski BM. Direction and rate of socket wear in Charnley low friction arthroplasty. J Bone Joint Surg 1985; 67-B: 757–761.
Wroblevski BM. Fifteen-to twenty-one-year results of the Charnley low-friction arthroplasty. Clin Orthop 1986; 211:30–35.
Livermore J, Ilstrup D, Morrey B. Effect of femoral head size on wear of the polyethylene acetabular component. J Bone Joint Surg 1990; 72-A: 518–528.
Cates HE, Faris PM, Keating EM, Ritter MA. Polyethylene wear in cemented metal-backed acetabular cups. J Bone Joint Surg 1993; 75-B: 249–253.
Shaver SM, Brown TD, Hillis SL, Callaghan JJ. Digital edge-detection measurement of polyethylene wear after total hip arthoplasty. J Bone Joint Surg 1997; 79-A: 690–700.
Callaghan JJ, Pedersen DR, Olejniczak JP, Goetz DD, Johnston RC. Radiographic measurement of wear in 5 cohort of patients observed for 5 to 22 years. Clin Orthop 1995; 317:14–18.
Charnley J, Kamangar A, Longfield MD. The optimum size of prosthetic heads in relation to the wear of plastic sockets in total replacement of the hip. Med Biol Engin 1969; 7:31–39.
Jasty M, Goetz DD, Bragdon CR, Lee KR, Hanson AE, Elder JR, Harris WH. Wear of polyethylene acetabular components in total hip arthroplasty. An analysis of one hundred and twenty-eight components retrieved at autopsy or revision operations. J Bone Joint Surg 1997; 79-A: 349–358.
Sychterz CJ, Moon KH, Hashimoto Y, Terefenko KM, Engh CA, Bauer TW. Wear of polyethylene cups in total hip arthroplasty. A study of specimens retrieved post mortem. J Bone Joint Surg 1996; 78-A: 1193–1200.
Buchorn U, Willert HG, Semlitsch M, Weber H. Dimensional changes of polyethylene acetabuli in Muller's hip endoprosthesis. Report on measurement methods and their clinical significance (German). Z Orthop Ihre Grenzgeb 1984; 122:127–135.
McLaren RH. Prosthetic hip angulation. Radiology 1973; 107:705–706.
Bland JM, Altman DG. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986; 1:307–310.
Kabo JM, Gebhard JS, Loren G, Amstutz HC. In vivo wear of polyethylene acetabular components. J Bone Joint Surg 1993; 75-B: 254–258.
Hop JD, Callaghan JJ, Olejniczak JP, Pedersen DR, Brown TD, Johnston RC. Contribution of cable debris generation to accelerated polyethylene wear. Clin Orthop 1997; 344:20–32.
Nasser S, Campbell PA, Kilgus D, Kossovsky N, Amstutz HC. Cementless total joint arthroplasty prostheses with titanium-alloy articular surfaces. A human retrieval analysis. Clin Orthop 1990; 261:171–185.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Košak, R., Antolič, V., Pavlovčič, V. et al. Polyethylene wear in total hip prostheses: the influence of direction of linear wear on volumetric wear determined from radiographic data. Skeletal Radiol 32, 679–686 (2003). https://doi.org/10.1007/s00256-003-0685-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00256-003-0685-2